
I. INTRODUCTION
In each IVF cycle, specialists have to determine the embryo with the best morphology, predicting successful implantation and further development. But the structure of the embryo is not the only indicator of quality; chromosomal abnormalities can be hidden behind it. One of the factors of implantation and early reproductive losses are chromosomal aneuploidies, which lead to a halt in the development of the embryo. Therefore, determining the genetic profile of the embryo is the key to a successful pregnancy outcome.
Preimplantation genetic testing for aneuploidy avoids errors in the selection of the most promising embryo and significantly increases the success of implantation. Despite the fact that assisted reproductive technologies are becoming more and more widespread, the effectiveness of the IVF program is within . The birth of a healthy child in a couple with any type of infertility depends on an incredible number of factors, but one of the key factors is the genotype of the embryo, which determines the survival and development of the latter. The ability to determine the quality of embryos is the cornerstone in a personalized approach to patient management and predicting the success of an IVF cycle.
According to the latest statistics, the number of children born with the help of assisted reproductive technologies (ART) on the globe has reached 8-10 million [2,4,6]. At the same time, despite the impressive figures, still up to of artificially initiated ART cycles do not end in a successful birth of children. In this regard, the continuous search for innovative invasive and non-invasive methods for selecting embryos with the highest potential continues. The new Next Generation Sequencing (NGS) technology is a direct genome analysis method that makes it possible to screen the entire set of chromosomes for quantitative and structural abnormalities, which makes it possible to exclude embryos with corresponding disorders before the transfer procedure. The results of recent scientific work have convincingly proved the effectiveness of preliminary genetic screening for aneuploidy in the selection process in individuals over 35 years of age [7-9]. This is due to the fact that in women older than 35 years, a higher level of quantitative and structural disorders in the chromosome set is determined, and therefore the probability of pregnancy in this group of patients is the lowest [8,10].
The aim of the study was to analyze the feasibility of performing genetic screening of embryos (Next Generation Sequencing - NGS) as part of infertility treatment cycles, to determine the relationship or its absence between the stage of development of the embryo and its survival, as well as an indicator of the successful development of pregnancy with previous genetic screening.
Based on the results of a comprehensive study, the effect of genetic screening, vitrification, oocyte competence and clinical indicators of patients on embryo survival was established.
II. MATERIALS AND METHODS OF RESEARCH
Transvaginal ovarian puncture was carried out at 36-37 hours after the start of the ovulation trigger. The identification of oocyte-cumulus complexes in the follicular fluid was carried out using a Nikon stereomicroscope (Japan), after which they were removed with a sterile micropipette. The complexes were washed and cleaned from liquid and blood using a HEPES buffer solution (G-mops, Vitrolife, Sweden). After counting the oocytes, they were transferred to special cups with a central well (Nunc) containing G-IVF+ culture medium (Vitrolife, Sweden) for pre-incubation for 2-3 hours (conditions: CO2 - 6%, O2 - 5%, at a temperature of 37 C. After incubation, mechanical and enzymatic removal of cumulus cells (denudation of oocytes) was carried out. In this case, the complexes were placed in a hyaluronidase solution for 30 seconds, followed by washing from enzymes in a buffer solution by a mechanical method.
For the vitrification of embryos, nutrient media from Irvine Scientific (USA) were used, based on the manufacturer's recommendations. Cryogenic preservation of embryos was carried out by direct and indirect exposure of the object to liquid nitrogen using open and closed type carriers (CryoTop, manufacturer Kitozato, Japan, Irvine Scientific, Sweden). After that, a retrospective study of cryoprotocol cycles was carried out on the basis of CJSC Medical Company IDK.
4 subgroups of SET (single embryo transfer) patients were selected for work:
- group 1 (n=20): included patients with NGS test cycles who underwent transfer of euploid embryos using their own oocytes;
- group 2 (n=446): included patients without NGS who underwent transfer of euploid embryos using their own oocytes;

Embryos were taken for transfer, in which the number of intact cells was more than .
The embryo biopsy procedure was carried out within 5-6 days of the pre-implantation period. The selection of blastocytes of at least the 3rd category of SWV was carried out on the basis of the developed system for assessing the quality of embryos and the system proposed by D.K. Gardner and Schoolcraft 1999. The RAHR Guidelines (2021) for assessing the quality of developing human embryos in vitro were also taken into account.
The classification we proposed took into account a number of key indicators: the degree of ECM formation, the degree of TB formation, the absence or presence of fragmentation with an indication of its degree (0-10%, 10-25%, 25-50%, more than 50%), the absence or presence of vacuoles, the absence or presence of degeneratively altered cells.
Based on these indicators, the following were established:
- group 3 : included patients without NGS who underwent embryo transfer using donor oocytes;
- group 4 (n=62): an additional group of patients without NGS who underwent embryo transfer using donor oocytes. This group was singled out due to the relatively smaller number of samples in group 3.
Patients of the 1st, 2nd and 3rd groups were homogeneous with average ages of 34.1; 34.3 and 34.6 years. In the 4th group - 42.3 years. Thus, a total of 536 cryocycles were studied.
To assess the structure of oocytes and embryos, a morphological method for assessing the quality of embryos was used using an inverted microscope OlympusX-73 (Japan) and a Nikon SMZ1000 stereomicroscope (Japan). Embryo vitrification was carried out in accordance with the manufacturer's freeze/thaw protocol (Irvine Scientific, USA). To assess the viability of the embryo, its morphological assessment was performed immediately after thawing (Fig. 1) and 2 hours after thawing (Fig. 2).

- The degree of expansion, that is, an increase in the size of blastocytes:
Based on the assessment of the above parameters in blastocysts, we determined:
i. The degree of expansion (increase in size) of the blastocyst:
- early blastocyst, in which the cavity occupies less than half the volume of the embryo
- blastocyst, in which the cavity occupies half or more of the volume of the embryo
- complete blastocyst, the cavity is completely filled by the embryo, but the zona pellucida is not thinned
- an enlarged blastocyst, the volume of the cavity is greater than the size of early embryos, and the zona pellucida is thinned
- blastocyst, in which trophoblast cells began to emerge through the zona pellucida
- blastocyst, completely out of the zona pellucid
ii. the degree of expression of the inner cell mass (ECM):
grade A - indicates densely packed ECM with many cells
grade B - ECM cells in large numbers, but weakly grouped class C - a small number of cells or their absence iii. assessment of the severity of trophoblast (TB):
class A - TB consists of a large number of cells;
class B - TB is represented by a small number of cells or contains single flattened cells;
class C - TB has very few cells, they are very flattened or absent in some places.
Based on the results of a morphological study of embryos on days 5-6, they were ranked by quality (excellent; good; satisfactory; mediocre quality and stopped in development) (Table 1).
Preimplantation genetic screening included the following steps:
- stage of trophoblast biopsy;
- stage of biopsy washing (3-6 cells);
- the stage of cell fixation in a special buffer solution, followed by a molecular cytogenetic study.
Trophoblast biopsy was carried out on the 5th-6th day (at 120-144 hours after follicle aspiration) of in vitro embryo cultivation, provided that the blastocyst corresponds to art. development (according to D.K. Gardneretal). The procedure was performed using an RI micromanipulator (CooperSurgical, Denmark), a Laser Octa xMTG laser gun (Germany) for cutting the zona pellucida, and a COOK micropipette (Ireland) for cell biopsy and aspiration.
III. RESULTS AND DISCUSSION
One of the factors of implantation and early reproductive losses are chromosomal aneuploidies, which lead to a halt in the development of the embryo. Therefore, determining the genetic profile of the embryo is the key to a successful pregnancy outcome.
The procedure of preimplantation genetic testing for the presence of aneuploidy avoids errors in the selection of the most promising embryo and significantly increases the success of implantation. Despite the fact that assisted reproductive technologies are becoming more and more widespread, the effectiveness of the IVF program is within . The birth of a healthy child in a couple with any type of infertility depends on an incredible number of factors, but one of the key factors is the genotype of the embryo, which determines the survival and development of the latter. The ability to determine the quality of embryos is the cornerstone in a personalized approach to patient management and predicting the success of an IVF cycle.
The proportion of chromosomal abnormalities in the structure of the causes of miscarriage is , and the rate of aneuploidy in the case of positive morphological parameters is (Rubio C., Bellver J. et al., 2017). The most modern and informative method to determine the quality of the embryo at the genetic level is the highly informative sequencing method - NGS. The material of the study was samples of the trophectoderm of embryos of 5-6 days of development obtained in IVF/ICSI cycles from 88 couples who were treated in the laboratory of assisted reproductive technologies of the IDK Clinical Hospital.
The age of women included in the study was up to 48 years. The distribution by age groups was as follows: patients under 35 years old accounted for (34) of the total, women aged 35-37 years old were (18), 38-40 years old - (15), patients over 40 years old - (21). All couples included in the study were divided into two groups - those with chromosomal abnormalities in one or both spouses, and couples with a normal karyotype of both spouses, for whom PGT was recommended for other reasons.
Women with a normal karyotype accounted for (correspondingly, with chromosomal abnormalities - ), and men (violations in the karyotype occurred in ). Couples without chromosomal disorders in any of the spouses were observed in (72 pairs) in this sample, and with such - (16 pairs). When analyzing differences in the studied indicator, the Mann-Whitney test (U) was used.
A total of 274 embryos were obtained using ART, which subsequently underwent PGT using the NGS method, the genetic material isolated from trophoblast cells obtained by blastocyst biopsy on days 5-6 after fertilization served as a sample. According to the results of PGT, 108 embryos were recommended for transfer, and 166 were not recommended. It should also be noted that in 5 cases , the transfer was recommended only with the written consent of the patients, since mosaic embryos were observed. In pairs with a normal karyotype, the following results were observed - (94) of embryos were recommended for transfer, and (123) were not recommended. Among couples with a pathological karyotype in one of the spouses, (14) of the embryos were euploid and recommended for transfer, and (43) had some kind of anomaly. Using the Kruskal-Wallis test, it was shown that in patients with abnormalities in the karyotype, there are no statistically significant differences in the chance of getting an aneuploid embryo between different age groups. In patients with normal karyotypes, the probability of getting a euploid embryo decreased with age. In most cases, women with a healthy karyotype and an embryo recommended for transfer after NGS had a normal pregnancy . It should also be noted that NGS revealed a large proportion of aneuploid embryos in the group of patients with abnormalities in the karyotype, which is very important for making a decision on choosing an embryo for transplantation.
Based on the obtained results, it is fair to speak about the need for PGTA in couples with multiple failures in IVF cycles and chromosomal abnormalities in the karyotype of one of the spouses, since according to the results of NGS sequencing, it was found that most of the embryos in such couples cannot be recommended for transfer due to for chromosomal abnormalities (56% in healthy couples and 75% in couples with abnormalities in the karyotype of one of the spouses). In 5 cases, mosaic embryos were still recommended for transfer, but only with the written consent of the patient, which can be explained by multiple failures in IVF cycles and the hope that the genetic material of the trophectoderm and the inner cell mass is different. Among this sample of patients, we can predict a successful IVF cycle in 43% in healthy couples and 25% in couples with deviations in the karyotype of one of the spouses. In other cases, it is necessary to repeat the fertilization of the egg and subsequent PGTA. In 37.5% of cases, patients had a healthy pregnancy after transplantation of a euploid embryo. Speaking about the age of a woman, it should be noted that the probability of obtaining a euploid embryo is higher in younger women with a normal karyotype. In the case of a genetic abnormality in a woman's karyotype, age does not statistically affect the likelihood of obtaining a healthy embryo (Fig. 4). The blastocyte survival rate was studied to establish the degree of influence of the vitrification process on embryos that had undergone a previous biopsy with the separation of 3-5 trophoblast cells. It is worth noting that biopsies are invasive procedures and carry the risk of damage to the embryo in the process. The results of the study are shown in Figure 1.
The data presented in Figure 1 show that the survival rate of embryos in the study group 1 was , which indicated that vitrification does not reduce the quality and viability of embryos after biopsy. It is possible that the high survival rate may also be associated with the previous selection of embryos with the highest potential. Statistical analysis revealed significant differences in survival rates between groups 1 and 3, as well as between groups 2 and 3, which indicates that survival in the group where donor material was used (group 3) was lower compared to groups 1 and 2, where own cells were used. At the same time, the age indicator did not affect survival in groups 3 and 4, where donor cells were used.
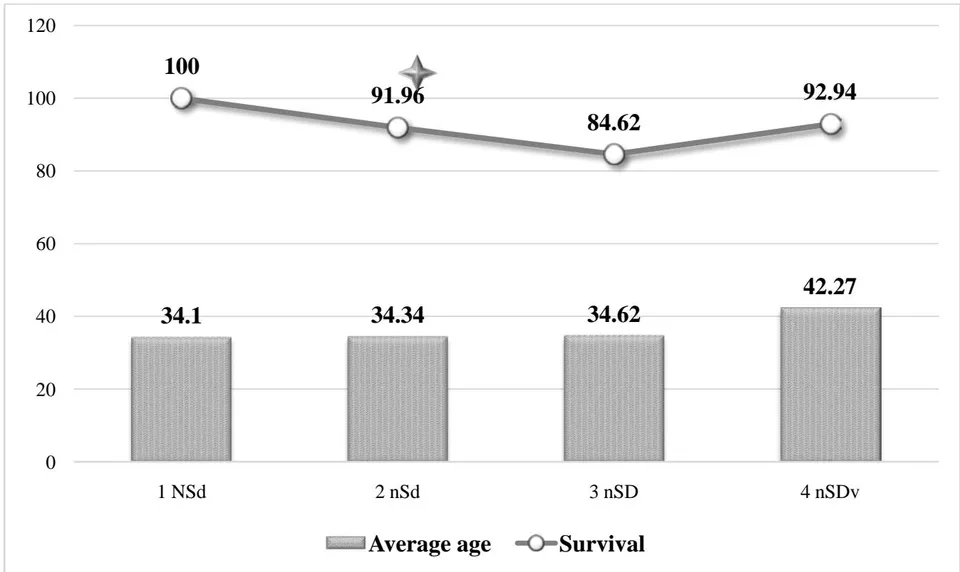
(Note: * - statistical significance in relation to the 3nSD group).
The lowest levels of hCG (+) were recorded in group 2, where own genetic material was used without previous genetic testing). Differences between groups 2 and 3, as well as 3 and 4 were statistically significant.
The study revealed the presence of comparable values in the analysis of CNB and NI in groups 1, 3 and 4, which indicated that genetic screening with the introduction of one's own oocytes makes it possible to obtain results close to the results when using donor material without taking into account the age of the recipients. This fact is also evidence that the
reproductive potential is determined by the properties of oocytes.
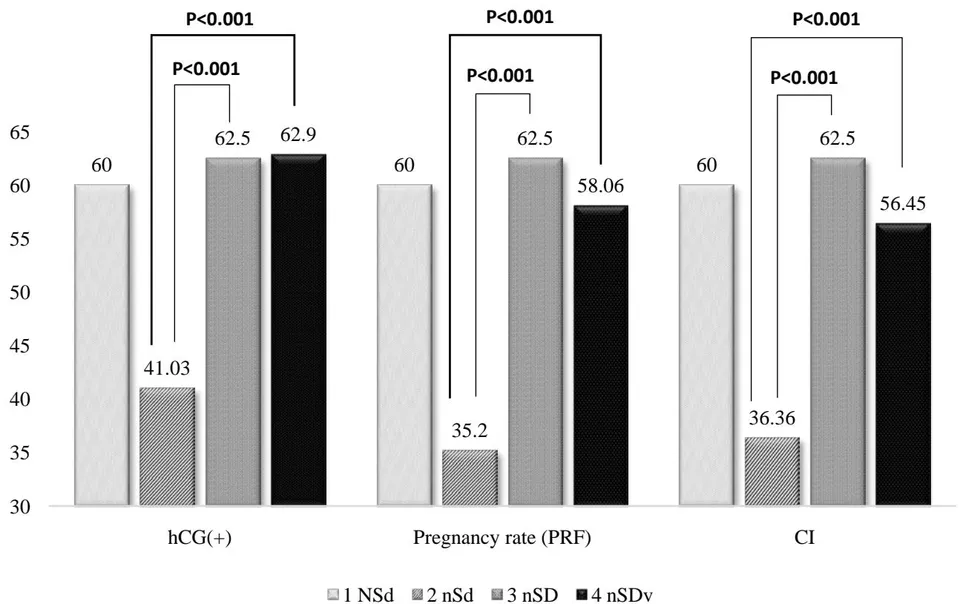
The graph shows that significant differences were established between groups 1 and 2, which confirms the effectiveness of the method of genetic screening and transport of a euploid embryo into the uterine cavity using its own material. Significant differences between the data of groups 2 and 3 also prove the effectiveness of using donor cells without previous genetic screening in the same age group. It also showed the advantage of using cryoprotocols (CNB, hCG frequency and Cl) with transfer after NGS in the group using donor material.
IV. CONCLUSION
Based on the results of a comprehensive study of the impact of genetic screening, vitrification, oocyte competence, and clinical indicators of patients on embryo survival, the following conclusions can be drawn:
- vitrification does not significantly affect the viability and quality of embryos, regardless of the biopsy;
- the main prognostic factor that affects the onset of pregnancy is the quality of oocytes and the degree of their ploidy;
- conducting genetic screening for the detection of aneuploidy significantly improves the results, bringing them closer to the results of patients who used donor material.
PGT is necessary in couples with multiple failures in IVF cycles and chromosomal abnormalities in the karyotype of one of the spouses, since according to the results of NGS sequencing, it was revealed that the majority of embryos in such couples cannot be recommended for transfer due to chromosomal abnormalities (56% in healthy couples and 75% in couples with deviations in the karyotype of one of the spouses).
Among this sample of patients, we can talk about the high competence of embryos and their implantation ability in in healthy couples and in couples with deviations in the karyotype of one of the spouses. In other cases, repeated fertilization of the egg and subsequent PGT are necessary. In of cases, patients of the two groups had a healthy pregnancy after transplantation of an euploid embryo (32% in the first group and in the second).
Speaking about the age of a woman, it should be noted that the probability of obtaining a euploid embryo is higher in younger women with a normal karyotype. In the case of a genetic abnormality in a woman's karyotype, age does not statistically affect the likelihood of obtaining a healthy embryo.
Vitrification of 5-6-day old blastocytes makes it possible to carry out trophoblast biopsy and genetic
screening, which, in turn, increases the likelihood of pregnancy when using euploid material.