Extraction Treatment of Severe Bimaxillary Incisor Protrusion in a High-Angle Class II Patient: Three-Dimensional Torque Control using ART and Ricketts Bioprogressive Mechanics
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
Dr. Dao Quang Huy. 2026. \u201cExtraction Treatment of Severe Bimaxillary Incisor Protrusion in a High-Angle Class II Patient: Three-Dimensional Torque Control using ART and Ricketts Bioprogressive Mechanics\u201d. Global Journal of Medical Research, Global Journal of Medical Research - J: Dentistry & Otolaryngology GJMR-J Volume 26 (GJMR Volume 26 Issue J1): .
## I. INTRODUCTION
Bimaxillary incisor protrusion is one of the most common conditions affecting facial esthetics in adolescent patients, particularly when associated with lip protrusion, mentalis muscle strain, and a convex facial profile [1,2]. In many cases, extraction-based orthodontic treatment is indicated to reduce incisor protrusion and improve the soft tissue profile. However, in patients with a vertical growth pattern (high-angle pattern), space closure following extractions is often more challenging due to an increased risk of anterior tooth extrusion, clockwise mandibular rotation, reduced occlusal stability, and difficulty in controlling the soft tissue profile [3-5].
From a biomechanical perspective, in the majority of extraction cases, the space-closing force is applied below the center of resistance of the anterior segment, thereby generating unfavorable moments, particularly negative torque. Consequently, the crowns tend to tip posteriorly while the roots are displaced anteriorly and labially, increasing the risk of labial cortical bone contact or periodontal complications such as fenestration and dehiscence, especially in the mandibular incisor region [6-9]. This risk is further exacerbated when the mandibular incisor roots are initially positioned close to the labial cortical plate, significantly narrowing the biological envelope available for lingual tooth movement [10-12].
Based on these considerations, this clinical case was designed with the following objectives: (i) reduction of incisor protrusion and improvement of soft tissue esthetics; (ii) vertical control in a high-angle patient; and (iii) three-dimensional torque control to protect the mandibular incisor roots from the risk of cortical bone perforation during prolonged space closure, through the combined use of an ART torque spring and segmented mechanics following the Ricketts-Bioprogressive philosophy.
## II. PATIENT INFORMATION AND CHIEF COMPLAINT
A 16-year-old male patient presented with the chief complaint of "protrusive upper and lower incisors, resulting in a protrusive facial appearance and poor esthetics." The patient's primary concern was to improve facial esthetics and reduce lip protrusion [1,2].
## III. CLINICAL EXAMINATION
### a) Extraoral Examination
Extraoral examination revealed a convex facial profile, with both the upper and lower lips positioned markedly anterior to the esthetic E-line [1,3]. Increased mentalis muscle activity was observed during lip closure, reflecting compensatory muscular function associated with mandibular incisor proclination. Overall, facial soft tissue esthetics were significantly compromised by incisor protrusion.


 Figure 1: Pre-Treatment Extraoral Photographs
### b) Intraoral Examination
Intraoral examination revealed severe proclination and protrusion of both the maxillary and mandibular incisors [6]. The occlusal relationship was Class I at the canine (tooth 3) and first molar (tooth 6) levels bilaterally. A critical unfavorable biological factor was the proximity of the mandibular incisor roots to the labial cortical plate, representing a high-risk condition when planning extraction-based anterior retraction mechanics [10-12]. All four third molars were present.




 Figure 2: Pre-Treatment Intraoral Photographs




 Figure 3: Pre-Treatment Intraoral 3D Digital Models
## IV. CEPHALOMETRIC ANALYSIS ACCORDING TO THE RICKETTS ANALYSIS SYSTEM
 Figure 4: Pre-Treatment Lateral Cephalometric Radiograph
Cephalometric analysis according to the Ricketts system revealed a mild skeletal Class II relationship, with a facial convexity of $3.4 \mathrm{~mm}$ [15]. The mandible was mildly retrusive relative to the cranial base, as indicated by a facial depth of $85.8^{\circ}$, while the maxilla demonstrated a relatively neutral position with a maxillary depth of $88.9^{\circ}$ [15,16].
Vertical analysis demonstrated a pronounced vertical growth pattern, with an increased FMA of $36.7^{\circ}$, an increased lower facial height (LFH) of $48^{\circ}$ (compared with the normal range of $45 - 46^{\circ}$ ), and a reduced facial taper of $57.5^{\circ}$ relative to the average value of approximately $68^{\circ}$ [3,15]. These findings reflect a tendency toward clockwise mandibular rotation and vertical facial imbalance.
Dentally, both maxillary and mandibular incisors exhibited markedly increased proclination and protrusion compared with physiological norms (maxillary incisors: protrusion 13.3 mm, inclination $41.6^{\circ}$; mandibular incisors: protrusion 10.7 mm, inclination $36.1^{\circ}$ [6,15]. Overall, this case represents severe bimaxillary incisor protrusion on a background of mild skeletal Class II malocclusion with a high-angle growth pattern, accompanied by an unfavorable biological risk factor characterized by the close proximity of the mandibular incisor roots to the labial cortical plate [10-12].
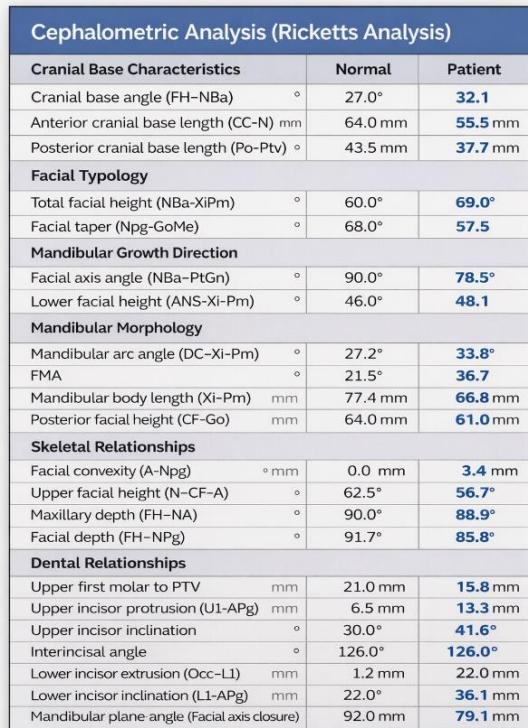 Figure 5: Pre-Treatment Cephalometric Analysis
## V. DIAGNOSIS
- Skeletal Malocclusion: Mild skeletal Class II.
- Growth Pattern: High-angle/vertical growth pattern.
- Dental Findings: Severe bimaxillary incisor protrusion and proclination.
- Occlusion: Bilateral Class I molar and Class I canine relationships.
- Risk Factor: Mandibular incisor roots positioned close to the labial cortical plate.
## VI. TREATMENT OBJECTIVES
1. To reduce protrusion and proclimation of the maxillary and mandibular incisors and improve soft tissue esthetics (reduction of lip protrusion and mentalis strain).
1. To maintain and refine a Class I occlusal relationship with optimal interdigitation.
1. To achieve vertical control during extraction-based treatment in a high-angle patient, minimizing anterior tooth extrusion and further clockwise mandibular rotation.
1. To protect the biological limits of the anterior dentition, particularly the mandibular incisors, through active torque control.
1. To obtain well-aligned dental arches with a stable arch form, facilitating long-term retention.
## VII. REATMENT PLAN
The selected treatment plan consisted of extraction of the four first premolars in both arches, combined with a moderate anchorage strategy. During the initial phase, maxillary anchorage was reinforced using mini-screws during canine retraction; subsequently, the mini-screws were removed during the anterior retraction phase to maintain overall anchorage at a moderate level, which was appropriate given the more cancellous nature of maxillary bone. An MBT 0.022 bracket system was used in combination with continuous archwire mechanics, an ART torque spring for mandibular incisor torque control, and segmented mechanics according to the Ricketts Bioprogressive philosophy to achieve three-dimensional control of tooth movement [6,15,18].
## VIII. TREATMENT PROGRESS
a) Alignment and Leveling
- MBT 0.022 slot brackets were bonded in both arches. The archwire sequence consisted of 0.014, 0.016, $0.016 \times 0.022$, $0.017 \times 0.025$, and $0.019 \times 0.025$ nickel-titanium wires, followed by a $0.019 \times 0.025$ stainless steel archwire to complete alignment and leveling. Each archwire was maintained for approximately 1-1.5 months. Extraction of the four first premolars was performed once stable alignment had been achieved, prior to initiating space closure.
b) Anchorage Setup and Canine Retraction
After progression to a $0.019 \times 0.025$ stainless steel archwire, two interradicular mini-screws measuring $1.6 \times 10 \mathrm{~mm}$ were placed in the maxillary arch between the first and second premolars to reinforce posterior anchorage. Elastomeric chains delivering approximately $150 \mathrm{~g}$ of force were applied from the mini-screws to the maxillary canines to perform canine retraction using sliding mechanics [6,8]. In the mandibular arch, moderate anchorage was established using elastomeric
chains delivering approximately $150\mathrm{g}$ of force from the first molars to the canines.
 Figure 6: Canine retraction on a $0.019 \times 0.025$ -inch stainless steel archwire using sliding mechanics
During the canine retraction phase, the patient wore intermaxillary elastics (3/16-inch, 3.5 oz) from the maxillary first molars to the mandibular first and second premolars to stabilize posterior occlusal interdigitation, as canine retraction using sliding mechanics tends to generate rotational moments and increases the risk of posterior occlusal disclusion [6,7].
From the rigid archwire stage onward, an ART torque spring was placed in the mandibular four-incisor region and maintained continuously throughout the canine retraction phase. The ART appliance functioned as an auxiliary torque spring, generating active positive torque to direct the incisor roots into cancellous bone and counteract the negative torque moments produced during space closure with force application below the center of resistance [6,9]. Studies on periodontal tissue response have demonstrated that light and continuous torque forces facilitate safe alveolar bone remodeling, particularly in regions where the incisor roots are positioned close to the labial cortical plate [22,23].
 Figure 7: Torque control of the mandibular incisor roots using an ART torque spring during space closure
During canine space closure, a commonly observed side effect is an increased tendency for the roots to approach the cortical bone. At the mandibular canine region (tooth 33), due to the close proximity of
the root to the labial cortical plate, tooth movement was slowed when sliding mechanics were applied [10-12]. Under these circumstances, a single-loop was fabricated on a $0.019 \times 0.025$ -inch TMA archwire to generate a root-directing moment, guiding the root into cancellous bone and thereby "reopening" the biological envelope available for tooth movement. The loop was activated at a rate of approximately $1.5 \mathrm{~mm}$ per month to complete the remaining space closure [19-21].
Following completion of canine space closure, a tendency for maxillary canine extrusion was observed. Therefore, two L-shaped loops with elastomeric elements were applied to deliver an intrusive force, reduce extrusion, and re-establish occlusal plane balance.
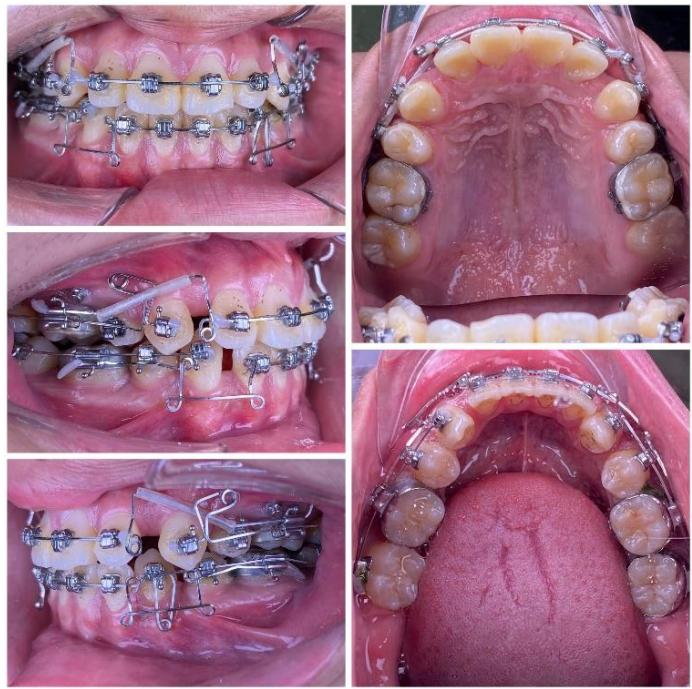 Figure 8: Space closure performed by segmented loop mechanics for canine retraction, followed by anterior space closure using a retraction arch with three-dimensional torque control
### c) Incisor Retraction using Segmented Mechanics
After completion of canine retraction, the incisor segment was retracted using segmented mechanics according to the Ricketts Bioprogressive philosophy. Retraction arches in both arches were designed to achieve three objectives simultaneously: (i) controlled incisor retraction; (ii) activation of an intrusive component of approximately 2-3 mm to counteract anterior tooth extrusion, which is particularly critical in high-angle patients; and (iii) generation of strong and stable positive torque to achieve three-dimensional control of incisor root movement, especially in the mandibular arch [19-21]. The retraction arches were activated at a rate of approximately 1.5 mm per month while maintaining torque and vertical control.
During the finishing phase, the ART torque spring was continuously maintained in the mandibular incisor region to reduce secondary negative torque and to assist in directing the incisor roots into cancellous bone, thereby protecting the labial cortical plate during the stage when retraction forces generate the most unfavorable moments [22-24].
After the occlusal objectives were achieved, the patient was progressed through finishing archwires (0.016 NiTi; 0.016×0.022 NiTi; 0.017×0.025 NiTi; and 0.017×0.025 stainless steel), in combination with intermaxillary elastics (3/16-inch, 3.5 oz) for midline correction and occlusal settling. Subsequently, space reopening was observed between the maxillary lateral incisors (tooth 2) and canines (tooth 3) bilaterally. A space-closing archwire with L-shaped loops positioned between teeth 2 and 3 was fabricated, and space closure was activated at approximately 1.5 mm per month over a two-month period, resulting in complete space closure. Thereafter, both arches were placed on 0.017×0.025 stainless steel archwires with full-arch elastomeric chains. Intermaxillary elastics were continued to assist in midline correction and to achieve optimal intercuspation.




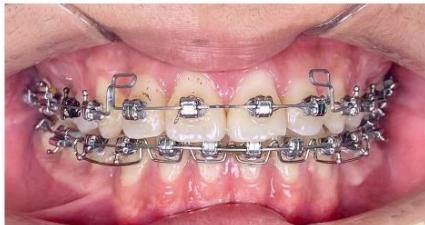



 Figure 9: Re-leveling and alignment phase following anterior space closure of the four incisors
The patient was retained for three months prior to appliance removal. The total treatment duration was 33 months.
## IX. TREATMENT RESULTS
After appliance removal, bilateral Class I canine and first molar relationships were achieved, with stable intercuspation. The maxillary and mandibular dental midlines were coincident, and both overjet and overbite were approximately $2\mathrm{mm}$. The dental arches in both jaws were well aligned, leveled, and exhibited a standardized arch form.
With respect to soft tissue outcomes, facial esthetics improved markedly, transitioning from a convex facial profile with lip protrusion relative to the E-line to a more harmonious facial profile with an E-line position approaching physiological norms. Mentalis muscle strain was reduced, facial esthetics were significantly enhanced, and the patient expressed satisfaction with the treatment outcome.
Notably, the mandibular incisor roots did not perforate the labial cortical plate and did not exhibit a clinically significant increase in negative torque, despite the prolonged space closure phase. This finding is of particular clinical relevance given the unfavorable biological limitations present at the beginning of treatment.




 Figure 10: Post-treatment intraoral photographs







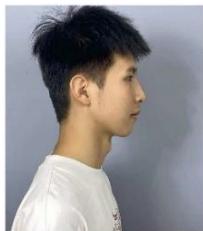 Figure 11: Comparison of incisor root position before and after treatment
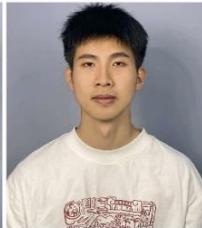
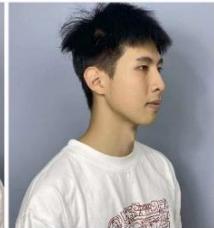
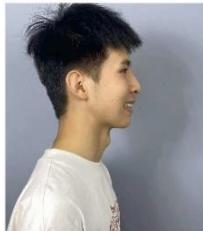
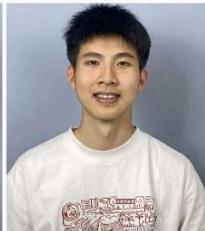
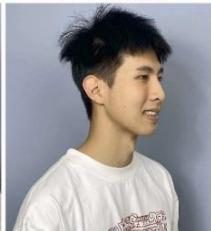 Figure 12: Post-treatment extraoral photographs
## X. PRE- AND POST-TREATMENT CEPHALOMETRIC CHANGES
Post-treatment cephalometric analysis according to the Ricketts system demonstrated marked improvements in incisor inclination and protrusion. Maxillary incisor inclination was reduced to $28.6^{\circ}$, with protrusion decreased to $7.4 \, \text{mm}$, while mandibular incisor inclination was reduced to $22^{\circ}$, with protrusion decreased to $3.4 \, \text{mm}$. Superimposed pre- and posttreatment tracings showed posterior repositioning and improved axial inclination of the incisors in both arches. The posterior teeth exhibited a slight mesial movement, consistent with the moderate anchorage strategy employed.
Notably, in the mandibular arch, the incisor roots were more favorably oriented within the cancellous bone compared with the pre-treatment condition, reflecting the effectiveness of active torque control during space closure.

 Figure 13: Post-Treatment Lateral Cephalometric and Panoramic Radiographs
Post-treatment Cephalometric Analysis (Ricketts)
<table><tr><td colspan="3">Cranial Base</td></tr><tr><td>Measurement</td><td>Normal</td><td>Patient</td></tr><tr><td>FH-NBa (°)</td><td>27.0</td><td>30.0</td></tr><tr><td>CC-N (mm)</td><td>64.0</td><td>55.8</td></tr><tr><td>Po-Ptv (mm)</td><td>43.5</td><td>35.9</td></tr><tr><td colspan="3">Facial Typology</td></tr><tr><td>Measurement</td><td>Normal</td><td>Patient</td></tr><tr><td>NBa-XiPm (°)</td><td>60.0</td><td>67.8</td></tr><tr><td>Facial taper Npg-GoMe (°)</td><td>68.0</td><td>59.6</td></tr><tr><td colspan="3">Mandibular Growth Direction</td></tr><tr><td>Measurement</td><td>Normal</td><td>Patient</td></tr><tr><td>Facial axis NBa-PtGn (°)</td><td>90.0</td><td>79.6</td></tr><tr><td>LFH ANS-Xi-Pm (°)</td><td>46.0</td><td>46.4</td></tr><tr><td colspan="3">Mandibular Shape</td></tr><tr><td>Measurement</td><td>Normal</td><td>Patient</td></tr><tr><td>Mandibular arc DC-Xi-Pm (°)</td><td>27.2</td><td>35.5</td></tr><tr><td>FMA (°)</td><td>21.5</td><td>35.9</td></tr><tr><td>Xi-Pm (mm)</td><td>77.4</td><td>65.0</td></tr><tr><td>CF-Go (mm)</td><td>64.0</td><td>65.0</td></tr><tr><td colspan="3">Skeletal Relations</td></tr><tr><td>Measurement</td><td>Normal</td><td>Patient</td></tr><tr><td>Facial convexity A-Npg (mm)</td><td>0.0</td><td>3.2</td></tr><tr><td>Upper facial height N-CF-A (°)</td><td>62.5</td><td>57.4</td></tr><tr><td>Maxillary depth FH-NA (°)</td><td>90.0</td><td>87.5</td></tr><tr><td>Facial depth FH-NPg (°)</td><td>91.7</td><td>84.5</td></tr><tr><td colspan="3">Dental Relations</td></tr><tr><td>Measurement</td><td>Normal</td><td>Patient</td></tr><tr><td>Upper 6 to PTV (mm)</td><td>21.0</td><td>18.1</td></tr><tr><td>U1-APg (mm)</td><td>6.5</td><td>7.4</td></tr><tr><td>Upper incisor inclination (°)</td><td>30.0</td><td>28.6</td></tr><tr><td>Interincisal angle (°)</td><td>126.0</td><td>128.9</td></tr><tr><td>Occ-L1 (mm)</td><td>1.2</td><td>-1.6</td></tr><tr><td>Lower incisor inclination (°)</td><td>22.0</td><td>22.5</td></tr><tr><td>L1-APg (mm)</td><td>1.0</td><td>3.4</td></tr><tr><td>Facial axis closure (°)</td><td>92.0</td><td>96.1</td></tr></table>
 Figure 14: Post-treatment Ricketts Cephalometric Analysis Figure 15: Superimposition on Ba-N at CC after treatment
## XI. DISCUSSION
This clinical case was challenging for three main reasons: the patient exhibited a high-angle growth pattern associated with an increased risk of anterior tooth extrusion and clockwise mandibular rotation; severe bimaxillary incisor protrusion required extensive and prolonged retraction; and the mandibular incisor roots were positioned close to the labial cortical plate, which significantly limited the biological envelope available for tooth movement [3-5,10-12].
The application of retraction forces below the center of resistance during space closure generates rotational moments that increase negative torque of the incisors, thereby elevating the risk of root displacement toward the labial cortical bone in the absence of active torque control [6,7].
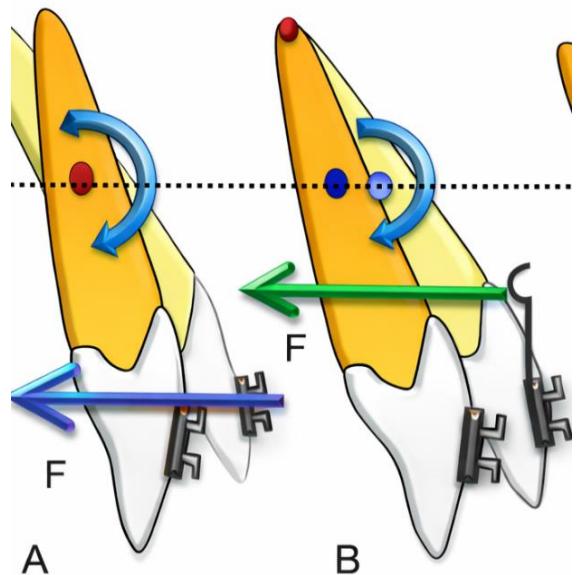 Figure 16: Negative torque moments and tooth extrusion occurring during space closure with force application below the center of resistance
 Figure 17: The ART torque spring generates active positive torque to control incisor root position In this case, an ART torque spring was employed as an auxiliary torque spring to generate additional positive torque moments, based on biomechanical principles of moment control and root movement as described by Burstone, and in accordance with studies on the biological response of periodontal tissues to light and continuous torque forces [9,22,23].
In addition, segmented mechanics using a single-loop on a TMA archwire and retraction arches designed according to the Bioprogressive philosophy allowed three-dimensional control of incisor movement by combining posterior retraction forces, intrusive forces, and strong positive torque. This approach is particularly suitable for high-angle patients, in whom vertical control plays a decisive role in occlusal stability and soft tissue esthetics [19-21].
## XII. RETENTION
After treatment, a Hawley retainer was delivered for the maxillary arch, and a fixed lingual retainer was bonded to the eight mandibular incisors. The Hawley retainer was prescribed for full-time wear (except during eating and oral hygiene) during the first year, followed by nighttime wear in subsequent years. All four third molars were scheduled for extraction after completion of orthodontic treatment.
## XIII. CONCLUSION
Extraction of the four first premolars in a high-angle patient with severe bimaxillary incisor protrusion and mandibular incisor roots positioned close to the labial cortical plate represents a significant biomechanical and biological challenge. In this case, the combination of continuous archwire mechanics with active torque control using an ART torque spring and segmented mechanics based on the Ricketts-Bioprogressive philosophy allowed effective reduction of incisor protrusion, improvement of soft tissue esthetics, maintenance of a Class I occlusal relationship, and, most importantly, preservation of biological safety in the mandibular incisor region throughout the prolonged space closure process.
Generating HTML Viewer...
Open Access
Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0)
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
×
This Page is Under Development
We are currently updating this article page for a better experience.
Thank you for connecting with us. We will respond to you shortly.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Extraction Treatment of Severe Bimaxillary Incisor Protrusion in a High-Angle Class II Patient: Three-Dimensional Torque Control using ART and Ricketts Bioprogressive Mechanics