Background-The menopausal progress is a complicated period in a lady’s life, reflecting ovarian maturing and hormonal changes, notwithstanding friendly and metabolic changes. These changes, thusly, impact the signs and issues normal to this period. Indications which are impacted by the hormonal variances happening during the menopausal progress incorporate vasomotor manifestations and vaginal dryness; others are bosom delicacy, rest issues and prefeminine dysphoria. Hormonal treatment has been demonstrated to be first-line treatment for a significant number of these manifestations. Different sorts of pharmacotherapies might be useful, including specific serotonergic take-up inhibitors for vasomotor side effects. Trademark indications of the menopausal change incorporate unusual uterine bleeding, best made do with hormonal pharmacotherapy; lessening bone mineral thickness, which might warrant analytic intercession, and may profit from dietary and way of life adjustments; and expanded weight list and deteriorating lipid profile, which additionally may profit from dietary and way of life alterations.
## I. BACKGROUND
The menopausal progress is a complicated period in a lady's life, reflecting ovarian maturing and hormonal changes, notwithstanding friendly and metabolic changes. These changes, thusly, impact the signs and issues normal to this period. Indications which are impacted by the hormonal variances happening during the menopausal progress incorporate vasomotor manifestations and vaginal dryness; others are bosom delicacy, rest issues and pre-feminine dysphoria. Hormonal treatment has been demonstrated to be first-line treatment for a significant number of these manifestations. Different sorts of pharmacotherapies might be useful, including specific serotonergic take-up inhibitors for vasomotor side effects. Trademark indications of the menopausal change incorporate unusual uterine bleeding, best made do with hormonal pharmacotherapy; lessening bone mineral thickness, which might warrant analytic intercession, and may profit from dietary and way of life adjustments; and expanded weight list and deteriorating lipid profile, which additionally may profit from dietary and way of life alterations.
## II. NEED AND SIGNIFICANCE
The hormonal milieu of the menopausal progress encourages annoying vasomotor manifestations, state of mind interruption, brief intellectual brokenness, genitourinary side effects, and other sickness measures that decrease the personal satisfaction of influenced ladies. The endocrine tumult of the menopause progress likewise uncovered racial and financial differences in the beginning, seriousness, and recurrence of indications. Hormonal treatment (HT) can be powerful for perimenopausal indications yet its utilization has been hindered by worries about wellbeing hazards saw in postmenopausal HT clients who are more established than 60 and additionally ladies who have been postmenopausal for more than 10 years.
The menopause progress is a problematic cycle that can keep going for longer than 10 years and causes issues in a greater part of ladies. Clinicians should perceive early signs and symptoms of the progress and be ready to offer treatment to alleviate these manifestations.
## III. OBJECTIVES
1. To find out the management strategies adopted by women in menopausal transition.
2. To find out the association between management strategies adopted by women in menopausal transition with marital status, education, occupation and menopausal transition stage.
3. To find out the adjusted effects of variables on the management strategies adopted by women in menopausal transition.
4. Find out the Correlation of knowledge on menopausal transition, health challenges of menopausal transition, health related quality of life and management strategies adopted.
## IV. METHODOLOGY
Non experimental approach with a cross sectional survey design was adopted. 420 women of 40-55 years from Randomly Selected seven wards of (wards 3, 5,14,18,20,21,24) a selected panchayath of Kunnamangalam block of Kozhikode district, Kerala were included using a cluster sampling technique. After getting IEC permission from Govt. college of Nursing, data were collected using a semi structured interview schedule having three part. Section A with socio personal variable, Section B to assess the reproductive, marital and clinical data. Section C to assess the Knowledge on menopausal transition. This section consists of 24 items, which are categorized as 8 items on the meaning and causes of menopausal transition,7 items under signs and symptoms and problems associated with menopausal transition and 9 items under diet, exercise and management strategies adopted.
The collected data were analyzed using both descriptive and inferential statistics using SPSS soft ware 18 version.
## V. RESULTS
### a) Socio personal characteristics of the participants
The present study showed nearly one fifth of the population belongs to the age group less than or equal to 44 (25.7%), nearly one third in the age group of 45-49 years (35.5%) and the remaining one third belonged to the age group of greater than 50 years (38.8%). As far as religion is concerned nearly three forth (74.8%) were Hindus, 20.7% were Islam and 4.3% were Christians and 0.2% were others. Out of the total sample more than half were home makers (68.8%) and 4.8% were private employees. only 7.6% were doing private employment and the rest 18.8% were working in the Govt. sector. Educational status showed 20% with non formal education, 30.2% with primary education, 17.6% completed secondary, 18.3% had higher secondary education and 8% were degree holders and 7.9% had post graduation. Regarding income, more than half had an income below Rs 5000/. Out of the subjects, 11% had an income of Rs >200001. Nearly cent percent are having a nuclear family (96.2%), only 2.4% had joint family and 1.4% had separated family. Nearly half of the sample had more than three members in the family (48.3%), 0.7% is having a single member in the family. Nearly hundred percent are following a mixed dietary pattern (97.9%) and only 2.1% are vegetarians.75.7% were following a sedentary life style and 24.3% doing hard work.
### b) Menstrual, marital and clinical history
The mean age of attainment of menarche was 14.12 years, with a SD of 1.21 and nearly $90\%$ attained menarche between 11 and 15 years. But $11\%$ attained after the age of 16.Out of the total sample, $38.1\%$ attained menopause. Out of the rest $38.6\%$ had irregular menstruation and the rest with regular menstruation. Out of the sample with irregular menstruation, $23.8\%$ had cycle duration less than 25 days and $13.6\%$ had a longer cycle, ie, within 35-65 days and $1.2\%$ had other type of irregularity. Women with menstruation $36.7\%$ had a flow less than 5 days, $18.6\%$ with 5-7 days of flow and
6.7% had $>7$ days flow. Out of the samples $92.9\%$ were married, $1.2\%$ were single, $4.5\%$ widows and $1.4\%$ living separated. Regarding age at marriage more than half married after 20 years $(55.2\%)$, $13.3\%$ got married before 18 years and $1.2\%$ were not married. The average age of attainment of menopause was 47.83 years. As far as other illnesses are concerned, $47.4\%$ had the history of illnesses. Diabetes mellitus, Thyroid disorders and hypertension were seen more in this study group. Out of the sample with history of illness, $5.7\%$ had Diabetes mellitus and $12.4\%$ had Hypertension. $6.7\%$ with thyroid disorders and $6\%$ with rheumatoid arthritis and $4.5\%$ had the history of allergy. DM and hypertension were seen along with almost all other illness in this group.
### c) Peri-menopausal status of the participants
Among the participants one fifth belonged to pre menopausal $(23.3\%)$, $38.6\%$ menopausal and $38.1\%$ post menopausal stage as per STRAW criteria. Out of the post menopausal group $35.5\%$ had natural menopause and $2.6\%$ had surgical menopause (attained menopause after hysterectomy). The mean age of menopause was found to be 47.83 years. As far as number of pregnancy are concerned, more than $50\%$ had less than two $(57.1\%)$, and $6\%$ never became pregnant and not having children. Out of the sample, $10.7\%$ of the women have One child, $50\%$ with two children and $31.9\%$ having more than two children. Regarding history of abortion $30.7\%$ had and the rest don't.
### d) Health seeking behavior of peri menopausal women
Nearly one third (22.1%) of the sample underwent ca cervix screening and the rest do not. Regarding mammogram $5.5\%$ only underwent mammographic screening. More than three fourth (65%) of the sample used oral contraceptive pill in their life for different reasons. Nearly ninety percent completed their last child birth before 35 years, More than forty percent breast fed their baby for one year and $35.71\%$ breast fed for more than 2 years.
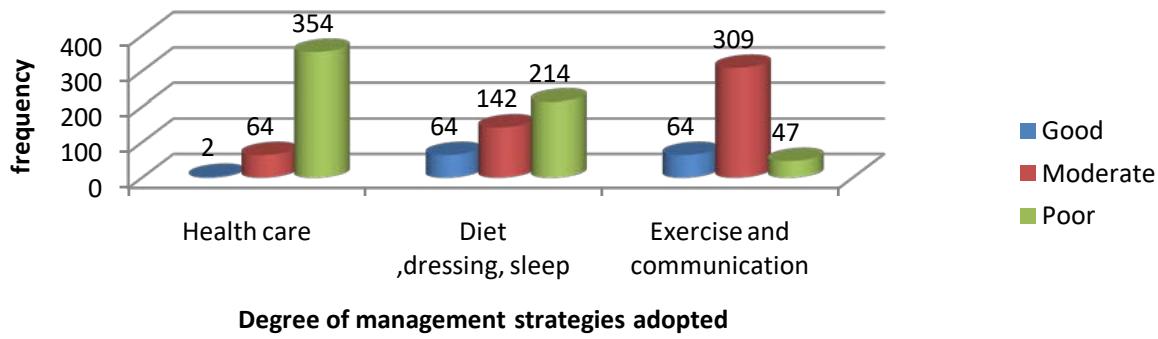
Graph 1: Distribution of participants based on degree of management strategies adopted.
The management strategies were classified and assessed under health care, Diet, Dressing and sleep, exercise and communication. Based on the total score in the various domains, the total management strategies were classified as good, moderate and poor. Out of the total sample, $26.9\%$ has got good, $56.42\%$ has got moderate and $14.28\%$ has got poor adoption of management strategies based on total score. The management under health care was seen poor than healthy life style and exercise and communication among these samples. $73.6\%$ of the sample has adopted a moderate practice of exercise and communication as a management strategy to deal with the particular stage of menopausal transition they belonged.
Table 1: Distribution of participants based on level of management strategies adopted. (n=420)
<table><tr><td colspan="2"></td><td colspan="2">Total management strategies adopted</td></tr><tr><td colspan="2"></td><td>f</td><td>%</td></tr><tr><td rowspan="4"></td><td>Poor</td><td>60</td><td>14.28</td></tr><tr><td>Moderate</td><td>237</td><td>56.42</td></tr><tr><td>Good</td><td>113</td><td>26.9</td></tr><tr><td>Very good</td><td>10</td><td>2.4</td></tr></table>
The data from the above table and graph is the division of the aggregate score of the total management strategy score of the participants. This data tell us nearly $15\%$ of the women of menopausal transition age were having a poor total management score and only $2.4\%$ had a very good score. It is good to say that the women of this study, who are mostly house wives, were using moderate level of management strategies to get acquainted with the inevitable stage of their life, the menopausal transition. Nearly thirty percent had $(26.9\%)$ good management.
Table 2: Descriptive association between management strategies adopted by women in menopausal transition and marital status. (n=420)
<table><tr><td>Marital status</td><td>N</td><td>Mean</td><td>Std. Deviation</td><td>df</td><td>F</td><td>P</td></tr><tr><td>Single</td><td>5</td><td>5.60</td><td>2.30</td><td rowspan="4">3 416</td><td rowspan="4">10.741</td><td rowspan="4">.000***</td></tr><tr><td>Married</td><td>390</td><td>10.14</td><td>4.52</td></tr><tr><td>Widow</td><td>19</td><td>5.95</td><td>2.22</td></tr><tr><td>Living separate</td><td>6</td><td>16.00</td><td>4.73</td></tr></table>
The descriptive analysis between management strategy adopted by women of different menopausal transition group with their marital status showed statistically significant difference between women who were single and who were living separate as determined by One Way Anova (F $(3,416) = 10.741$, $p=.000$ ). A Tukey HSD post hoc test revealed that the management strategy score was statistically significantly lower among women who are single with others like married and living separate. Women who were widow also had a less mean score compared to other groups. Marriage and family support really improves the health seeking of women.
Table 3: Descriptive association between management strategies of women in menopausal transition and occupation. (n=420)
<table><tr><td>Occupation</td><td>N</td><td>Mean</td><td>Std. Deviation</td><td>df</td><td>F</td><td>P</td></tr><tr><td>House wife</td><td>289</td><td>9.52</td><td>4.16</td><td rowspan="4">3</td><td rowspan="4">3.205</td><td rowspan="4">.000***</td></tr><tr><td>Private employee/coolie</td><td>20</td><td>10.95</td><td>5.59</td></tr><tr><td>Temporary</td><td>32</td><td>11.16</td><td>5.18</td></tr><tr><td>Govt. job</td><td>79</td><td>10.95</td><td>5.29</td></tr></table>
The descriptive analysis between management strategy adopted by women of different menopausal transition group with their occupation showed statistically significant difference between women who were home makers and who were engaged with other jobs like private employment, temporary work/coolie and with government jobs as determined by One Way Anova(F(3,416)=3.205, p=.000). A Tukey HSD post hoc test revealed that the management strategy score was statistically significantly lower among women who are home makers than with others like doing private employment, temporary work or Government jobs. Women engaged in temporary work showed a high statistically significant mean score than women with private/coolie work or government job. The findings may be due to the individual differences.
Table 4: Descriptive association between management strategy adopted by women in menopausal transition and education
<table><tr><td>Education</td><td>N</td><td>Mean</td><td>Std. Deviation</td><td>df</td><td>F</td><td>P</td></tr><tr><td>Non formal education</td><td>84</td><td>9.90</td><td>3.89</td><td rowspan="5">5 414</td><td rowspan="5">17.832</td><td rowspan="5">.000***</td></tr><tr><td>Primary</td><td>127</td><td>8.42</td><td>4.05</td></tr><tr><td>Secondary</td><td>74</td><td>10.66</td><td>4.82</td></tr><tr><td>Higher secondary</td><td>77</td><td>8.77</td><td>3.78</td></tr><tr><td>Degree and above</td><td>58</td><td>14.20</td><td>4.55</td></tr></table>
The descriptive analysis between management strategy adopted by women of different menopausal transition group with their education level showed, a statistically significant difference between women who were primary educated and who were underwent higher education as determined by One Way Anova $(F(5,414) = 17.832, p =.000)$. A Tukey HSD post hoc test revealed that the management strategy score was statistically significantly lower among women who are having higher secondary education, non formal education, primary, secondary than with degree and above. The findings may be due to the individual characteristics of the sample.
Table 5: Descriptive association between management strategy adopted by women and menopausal transition stage
<table><tr><td>Menopausal transition stage</td><td>N</td><td>Mean</td><td>Std. Deviation</td><td>df</td><td>F</td><td>p</td></tr><tr><td>Pre menopausal</td><td>98</td><td>11.73</td><td>4.71</td><td>2</td><td rowspan="3">14.959</td><td rowspan="3">.000***</td></tr><tr><td>Menopausal</td><td>162</td><td>10.22</td><td>4.09</td><td rowspan="2">417</td></tr><tr><td>Post menopausal</td><td>160</td><td>8.66</td><td>4.60</td></tr></table>
The descriptive analysis between management strategy adopted by women of different menopausal transition group showed statistically significant difference between women who are post menopausal than who are pre menopausal as determined by One Way Anova $(F(2,417) = 14.959, p =.000)$. A levenes post hoc test revealed that the management strategy score was statistically significantly lower among women who are post menopausal than pre menopausal. The women of menopausal group also had a lower statistically significant mean score compared to the premenopausal group. Adoption of management strategy depends on the need, availability, and individual knowledge.
Table 6: Adjusted effects of variables on the management strategies adopted by women in menopausal transition. $(n = 420)$
<table><tr><td>Variable</td><td>Beta Co-efficient</td><td>t</td><td>Sig.</td></tr><tr><td>Income</td><td>.74</td><td>4.8</td><td>.000***</td></tr><tr><td>Dietary pattern</td><td>-.25</td><td>-.34</td><td>.734</td></tr><tr><td>Life style</td><td>.42</td><td>.822</td><td>.412</td></tr><tr><td>Number of pregnancy</td><td>.67</td><td>1.78</td><td>.076</td></tr><tr><td>Menstrual status</td><td>-.77</td><td>-2.96</td><td>.003**</td></tr><tr><td>Breast feeding duration of last child</td><td>-1.50</td><td>-3.34</td><td>.001**</td></tr></table>
From the above table, a linear regression established that income, menstrual status, breast feeding duration of last child could statistically significantly associated with the health challenges of menopausal transition. $P <.001$, Adjusted R square $12.3\%$ of the explained variability in the health challenges. Dietary pattern, life style and number of pregnancy were not statistically significantly associated with the management strategies adopted during menopausal transition among women in menopausal transition.
Table 7: Correlation analysis of knowledge on menopausal transition, health challenges of menopausal transition, health related quality of life and management strategies adopted. (n=420)
<table><tr><td rowspan="2">Knowledge on MT</td><td>Knowledge on MT</td><td>Health challenges</td><td>HRQOL</td><td>Management strategies</td></tr><tr><td>1</td><td></td><td></td><td></td></tr><tr><td rowspan="2">Health challenges</td><td>.275**</td><td>1</td><td></td><td></td></tr><tr><td>.000</td><td></td><td></td><td></td></tr><tr><td rowspan="2">HRQOL</td><td>.286**</td><td>.628**</td><td>1</td><td></td></tr><tr><td>.000</td><td>.000</td><td></td><td></td></tr><tr><td rowspan="2">Management strategies</td><td>.288**</td><td>.301**</td><td>.311**</td><td>1</td></tr><tr><td>.000</td><td>.000</td><td>.000</td><td></td></tr></table>
## VI. DISCUSSION
Menopause in human is an in evitable and age related phenomenon, having associated with general health problems and problems specific to menopausal change too. So the principle of caring should consider the both. Drugs should be used with utmost care. Health care of aging women should approach with knowledge, optimism and compassion. Steps should be taken to provide effective and safe treatment for the most distressing menopausal symptoms of woman by taking in to consideration the good and bad effects of treatment.
Studies report that HRT to be used with most care, considering the general bone mineral density loss in both genders after 50 years, more among the female. A sensible approach, nutrition, exercise and ERT have found effective in MT symptom management. Helping woman to have a careful selection of HRT for the rest of her life is essential at a very early age of recognition of the first menopausal transition related symptom. Studies recognized the good effect of ERT in preserving and enhancing the cognitive function in post menopausal women. Exercise, stress reduction, and dietary changes may improve the QOL as they age.
Studies emphasized the greater advantage of a self help group for menopausal women at their community level to share their thoughts and up to date information, clarify their doubts and to empower them to take decisions too. These groups will have a therapeutic impact in the life of woman. Many herbal and homeopathic products with limited clinical trials were found to be effective in managing menopause related health issues, if taken as per direction. HRT use was more seen among smokers, with surgical menopause, with better socio economic status, higher education, and living in urban area. Single, divorced and widowed used HRT more than married. The more symptomatic women who were regularly consulting were the regular use of HRT. HRT has got a very positive role on the psychological well being among the post menopausal women. Studies in the USA revealed many women during MT, seek health care variably. VMS were considered as the most common symptom reported by all races/ ethnicities. HRT, complementary and alternative medicine were used variably by these participants. Studies reported the beneficial effects of HRT, once started immediately after the menopause, but adverse effects also were reported. Studies reported the positive effects of exercise, yoga on menopausal symptoms. Studies also highlighted the importance of having greater awareness while handling the menopausal population from different ethnicities. Non leisure time physical activity seemed to be associated with a favourable sleep quality. Domestic guide lines on urinary incontinence and problems are found to be of great help among this group. Symptom management model to be practiced among this population to alleviate anxiety and to enhance the menopausal experience of women. Health and life style of the middle aged women need to be taken care of well. One Japanese study highlighted the effect of a ten minute stretching just before sleep in reducing the menopausal symptoms of Japanese women. Acupuncture showed good effect on VMS. Group education also found beneficial among this group. Soy isoflavones found to be good for managing the somatic and mental symptoms among the peri and post menopausal ladies.
## VII. CONCLUSION
Need for empowering the women to actively participate in the management of MT symptoms including self care strategies provide a sense of worth and well being to them. This will have positive role in the general improvement of menopausal symptoms and overall health.
Generating HTML Viewer...
References
20 Cites in Article
Antonia Lyons,Christine Griffin (2003). Managing menopause: a qualitative analysis of self-help literature for women at midlife.
Lenarindner (2017). Reducing menopausal symptoms for women during the menopause transition using group education in a primary health care setting-a randomized controlled trial.
Maya Lambiase,Rebecca Thurston (2013). Physical activity and sleep among midlife women with vasomotor symptoms.
Laura Lampio,Päivi Polo-Kantola,Olli Polo,Tommi Kauko,Jenni Aittokallio,Tarja Saaresranta (2014). Sleep in midlife women.
Lilystojanovska (2014). To exercise, or, not to exercise, during menopause and beyond.
Lisa Gallicchio,Susan Miller,Judith Kiefer,Teresa Greene,Howard Zacur,Jodi Flaws (2015). Risk factors for hot flashes among women undergoing the menopausal transition.
Hui-Koon Lim,Sandra Mackey (2012). The Menopause Transition Experiences of Chinese Singaporean Women.
; Loesjaspers (2015). Health in middle-aged and elderly women: A conceptual framework for healthy menopause.
Lydia Brown,Christina Bryant,Valerie Brown,Bei Bei,Fiona Judd (2015). Investigating how menopausal factors and self-compassion shape well-being: An exploratory path analysis.
Lorraine Dennerstein,John Randolph,John Taffe,Emma Dudley,Henry Burger (2002). Hormones, mood, sexuality, and the menopausal transition.
Lorraine Dennerstein,A (2003). The Menopause and Sexual Functioning: A Review of the Population-Based Studies.
Alastair Maclennan (2009). Hormone replacement therapy: a 2008 perspective.
Pauline Maki,Lauren Drogos,Leah Rubin,Suzanne Banuvar,Lee Shulman,Stacie Geller (2008). Objective hot flashes are negatively related to verbal memory performance in midlife women.
Lorraine Dennerstein,; (2000). A prospective population-based study of menopausal symptoms.
Mary Lumsden,Ann (2016). Menopausal symptoms in Bangladeshi women in midlife.
L Gao,T Zheng,W Xue,Y Wang,Y Deng,H Zuo,A Sun (2017). Efficacy and safety evaluation of <i>Cimicifuga foetida</i> extract in menopausal women.
Plácido Llaneza,María García-Portilla,David Llaneza-Suárez,Begoña Armott,Faustino Pérez-López (2012). Depressive disorders and the menopause transition.
Lotta Lindh-Åstrand,; (2007). Women's conception of the menopausal transition -a qualitative study.
Rui-Xia Li,Min Ma,Xi-Rong Xiao,Yan Xu,Xiu-Ying Chen,Bin Li (2016). Perimenopausal syndrome and mood disorders in perimenopause.
Lilian Thompson,Beatrice Boucher,Zhen Liu,Michelle Cotterchio,Nancy Kreiger (2006). Phytoestrogen Content of Foods Consumed in Canada, Including Isoflavones, Lignans, and Coumestan.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Dr. Vijayasree K V. 2026. \u201cManagement Strategies Adopted by Women in Menopausal Transition in a Selected Panchayath of Kozhikode District, Kerala, India\u201d. Global Journal of Medical Research - E: Gynecology & Obstetrics GJMR-E Volume 22 (GJMR Volume 22 Issue E1).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































