Background: According to WHO, the number of patients with glaucoma in the world ranges from 60.5 to 105 million people, and the number of such patients is also predicted to increase to 80 million. Out of 28 million blind people in the world almost one in five lost their sight due to glaucoma. The aim of this research is to conduct a systematic review of the clinical and economic evidence for the treatment of primary open-angle glaucoma with Tafluprost vs Travoprost.
## I. INTRODUCTION
Glaucoma is one of the leading causes of blindness, it is a chronic disease that visual area is reduced permanently because of optic nerve damage.
According to the World Health Organization, total number of patients with glaucoma in the world ranges from 60.5 to 105 million people, and increasing this number is predicted to 80 million. There is significant an increase the role of glaucoma among primary disability causes, the nosological structure increased up to $20\%$ in the last decade. According to the statistics of WHO, more than 28 million people in the world faced to the blindness, it means almost one in five has lost sight cause of glaucoma.
In majority of patients (about $86\%$ ) suffer from glaucoma for a long time, the disease passes into a more severe stage. In this regard, this disease is not only purely medical issue, but also it is social problems.
The research questions were asked in discussions with healthcare providers, clinical professionals, and other healthcare stakeholders.
The aim of the study was to conduct a systematic review of the clinical and economic evidence for the therapy of primary open-angle glaucoma (POAG) with Tafluprost vsTravoprost.
## II. MATERIALS AND METHODS
A literature search was performed on PubMed interface and used for the MEDLINE database, in addition, the Cochrane Central Register of Controlled Trials, the Cochrane Database of Systematic Reviews, and NICE were used to search for relevant literature. As an input of medical librarians, search strategy was developed by using appropriate keywords and control variables. In order to obtain relevant information on the prevalence of glaucoma and other important evidence, we searched the gray literature on various health websites. The formulation of the PICO concept is very critical because it facilitates the therapeutic question and directly addresses the relevant issues, defining the key concepts that should be the focus of our economic analysis of health care.
The acronym PICO is presented in the following table 1 below:
Table 1: PICO formulation for literature search
<table><tr><td>Acronym</td><td>General definition</td><td>Acceptance of the model</td></tr><tr><td>P</td><td>Population (patients)</td><td>Patients over 40 with open-angle glaucoma</td></tr><tr><td>I</td><td>Intervention (Intervention - an alternative method of treatment (relatively new)</td><td>Tafluprost is a prostaglandin analogue eye drops used to prevent the progression of open-angle glaucoma by lowering intraocular pressure(IOP).</td></tr><tr><td>C</td><td>Comparator (Comparator - traditional treatment)</td><td>Travoprost is a prostaglandin analogue eye drops used to prevent the progression of open-angle glaucoma by lowering IOP.</td></tr><tr><td>O</td><td>Outcome of economic efficiency (The result is profitability)</td><td>Lowering IOP and delaying the progression of glaucoma</td></tr></table>
In order to evaluate clinical outcomes feedback was requested from several associations involved in glaucoma therapy in Tashkent city. We turned to an ophthalmologist, nurses who regularly diagnose glaucoma in patients. The role of the clinical expert was to critique our requests, provide information regarding the patient management algorithm, review the clinical review plan and medical technology assessment.
Economic literature search was conducted to cover studies conducted from inception to the date of the search. PubMed interface was used for the Medline database, and the Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, and NICE were used to search relevant literature. By input from medical librarians, a search strategy was developed with relevant keywords and control variables, with an economic filter set. In order to obtain relevant information on the current prevalence of glaucoma and other important evidence, we conducted a gray literature search on various health websites.
Titles and abstracts of the papers were carefully reviewed, for those studies that should meet the eligibility criteria, we purchased articles with full content and completed further evaluation for eligibility.
### a) Inclusion Criteria
- Full content publications in English;
- Studies have been carried out from the moment of creation to the present day;
- Studies comparing Tafluprost with Travoprost in patients with open-angle glaucoma;
- Profitability analysis;
### b) Exclusion Criteria
- Reviews, polls, edited compositions, notifications, letters, case studies and articles;
- An economic evaluation of laser treatment of open-angle glaucoma and eye drops was carried out;
### c) Outcomes of concern
- Quality-adjusted life years (QALY);
- Expenses;
- Additional costs or additional efficiency;
- Average cost utility ratios and costs from different points of view;
### d) Data Extraction
The data was obtained under the following conditions:
- Source (for example: country, year of publication and title);
- Sample set and comparator;
- Intervention;
- Outcomes (costs, incremental economic effectiveness ratios, side-effects and well-being outcomes);
## III. RESULTS AND DISCUSSIONS
A clinical efficacy literature search identified 434 studies, including those obtained from database searches and additional sources. After removing duplicates and irrelevant studies assessed by title selection, 285 citations remained. Finally, only 2 articles meet the inclusion criteria. To report the studies, we found in systematic reviews, we developed the PRISMA Chart (Preferred Reporting Items for systematic reviews and meta-analyses) (Figure 1).
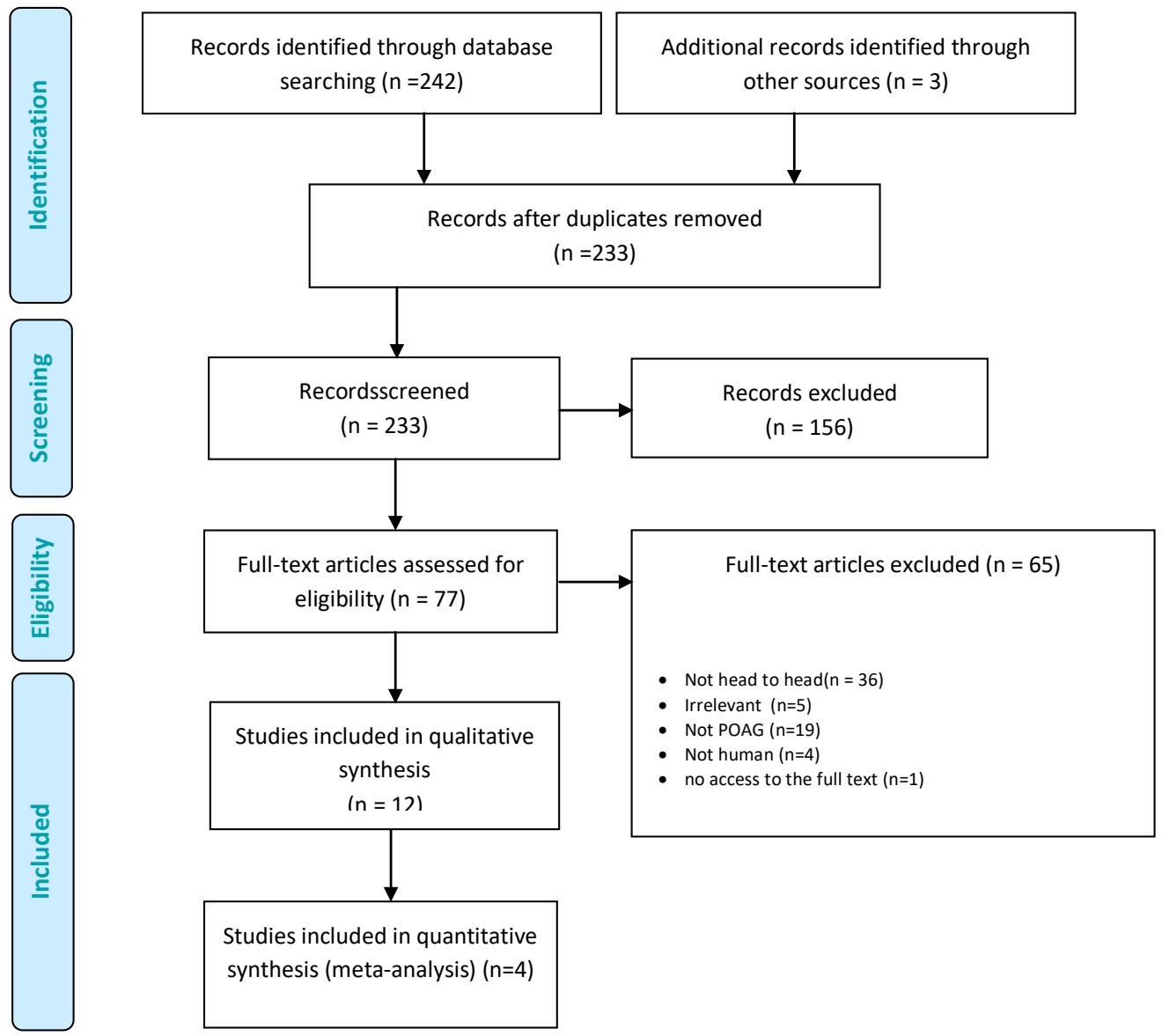 Fig. 1: PRISMA diagram - results of clinical effectiveness
Literature search about economic effectiveness identified 50 studies, including those obtained from database searches and additional sources after dedduplication. After eliminating duplicates and irrelevant studies assessed by title checking 10 citations remained for full-text citation. Finally, after reviewing full-text articles, one study was selected that met the inclusion criteria. Figure 2 is a PRISMA chart for the results of an economic search strategy.

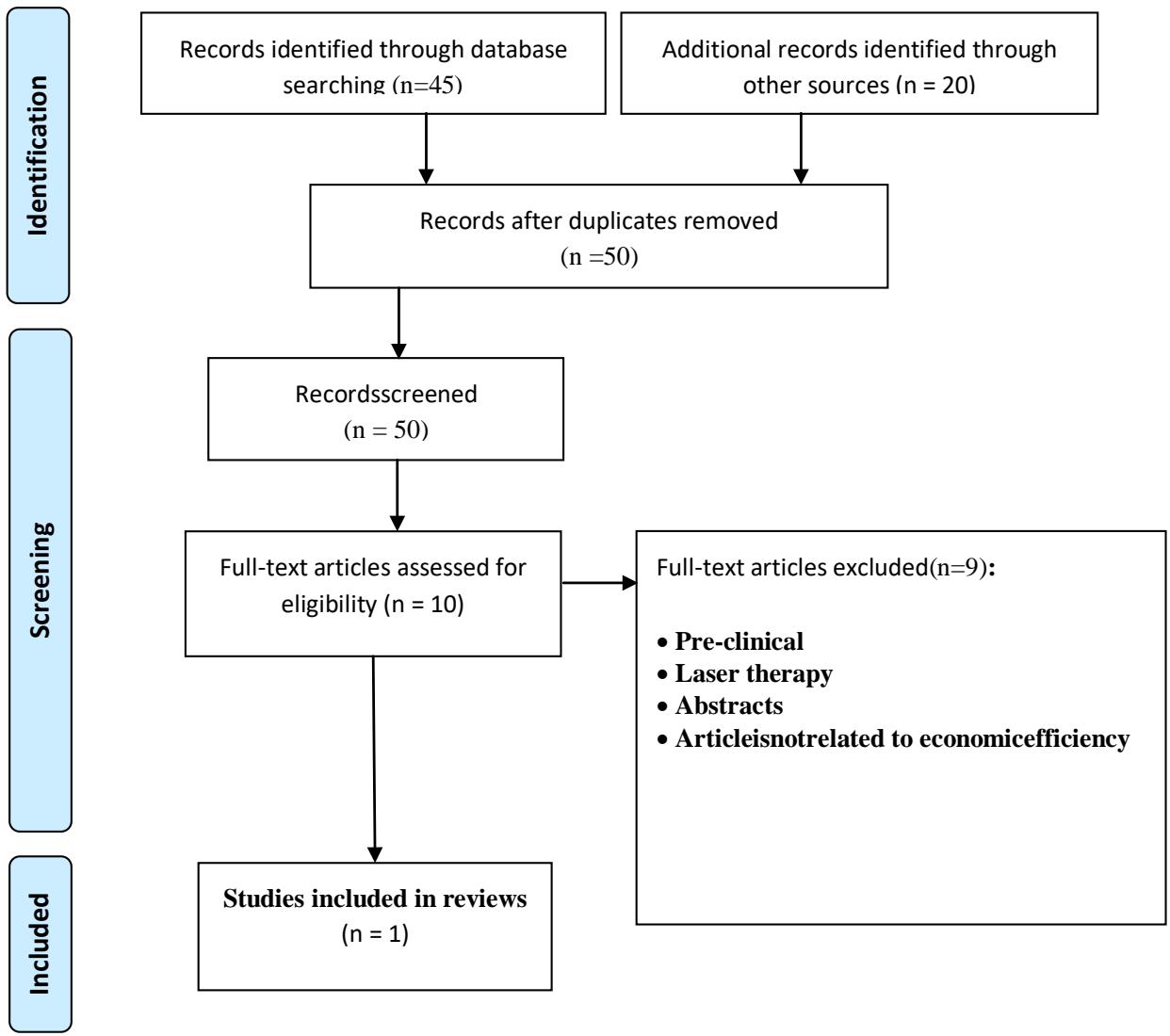 Fig. 2: PRISMA chart - economic search results
Two single arm cohort studies were selected because they met the inclusion criteria. The first study examined IOP adjustment and visual area imperfection movement over a 3-year period while adjusting Travoprost eye drops monotherapy in patients with POAG [2]. A second cohort study examined the effects of Tafluprost eye drops on IOP changes, visual area progression, safety, and side effects in patients with POAG [3].
We were unable to find studies examining mortality due to glaucoma. In addition, there is no any research conducted to investigate patients with advanced and end-stage glaucoma treated with our interventions.
Table 2: Research, patients and intervention features
<table><tr><td>Authors, year</td><td>Country</td><td>Purpose of the study</td><td>Randomized groups</td><td>Basic mean deviation(MD)</td><td>Patients(men /women)</td><td>Average age Years (SD)</td><td>Result</td></tr><tr><td>Inoue, Iwasa, Wakakura and Tomita, 2012</td><td>Japan</td><td>To study the efficiency of long-term Travoprost monotherapy without (BAC) on IOP and visual area efficiency.</td><td>Mean IOP at switch on 16.8±2.6 mmHg.</td><td>-5.4±4.7dB</td><td>76:33/43</td><td>54.8±13.9</td><td>Decreased intraocular pressure (IOP)</td></tr><tr><td>Inoue, Tanaka and Tomita, 2013</td><td>Japan</td><td>Calculate the effect of Tafluprost treatment for 3 years on visual area and intraocular pressure.</td><td>Initial IOP 15.7±2.2 mmHg.</td><td>-6.75±5.5dB</td><td>55:32/23</td><td>56.1±11.2</td><td>Decreased intraocular pressure (IOP)</td></tr></table>
Table 3: Decrease in IOP and progression of the visual area
<table><tr><td>Author s, year</td><td>Level of IOP reduction</td><td>Progression field of view</td></tr><tr><td rowspan="2">Inoue, Iwasa, Wakakura and Tomita (2012)</td><td>When treated with Travoprost</td><td rowspan="2">2.8%–13.9%</td></tr><tr><td>14.1±2.4 mmHg (Before treatment: 16.8±2.6 mmHg)</td></tr><tr><td rowspan="2">Inoue, Tanaka and Tomita (2013)</td><td>When treated with Tafluprost</td><td rowspan="2">10.3%–13.8%</td></tr><tr><td>12.8±2.8 mmHg Art. (before therapy: 15.7±2.2 mmHg)</td></tr></table>
Overall, both Travoprost and Tafluprost were found to be effective interventions for lowering intraocular pressure in patients with POAG. Innouetal. (2012) in their randomized control trial showed the effectiveness of Travoprosteye drops in reducing IOP, which in the long term was $16.1 - 36.6\%$ while the reduction in IOP by $21.9\pm 14.0\%$ with the introduction of Tafluprost in patients with POAG. There have been no reports of visual area impairment due to long-term use of Tafluprost and Travoprost eye drops. Significant differences in average and standard deviation of the model were not observed before and after treatment with follow-up 3 years in both analyzed studies. It can be seen that when comparing the efficacy of the two interventions, Travoprost had a slightly higher efficacy in lowering IOP than Tafluprost among patients with POAG [2, 3].
A systematic review identified one study evaluating the economic effectiveness of Travoprost and Tafluprost in the treatment of pre-intervention open-angle glaucoma in previously untreated 65-year-old patients. Intraocular pressure, visual area characteristics, and patient value of drugs are derived from published retrospective clinical reviews and randomized control trials with a follow-up period of 20 years. Average wholesale prices were taken to calculate drug price data for both social and direct eye care costs. As recommended by the Health and Medicine Cost Efficiency Panel, all costs and benefits assessed by the patient were discounted annually at a rate of $3\%$.
Table 4: Economic indicators of Tafluprost and Travoprost
<table><tr><td rowspan="2">Author, year</td><td rowspan="2">Study type</td><td rowspan="2">Population</td><td rowspan="2">Intervention/ Control (Comparator)</td><td colspan="3">Results</td><td rowspan="2">Research period</td></tr><tr><td>health outcomes</td><td>Expenses</td><td>Economic Efficiency</td></tr><tr><td rowspan="2">Brown 2019</td><td rowspan="2">Cost-utility analysis</td><td rowspan="2">Patients over 40 years of age</td><td>Tafluprost</td><td>1.99 QALY (17.9%)</td><td>$1,925 cost/year</td><td rowspan="2">ICER is missing</td><td rowspan="2">3 months a</td></tr><tr><td>Travoprost</td><td>1.92 QALY (17.2%)</td><td>$944 cost/year</td></tr></table>
QALY- Quality Adjusted Life Years (Additional Years of Quality Life)
The results showed that each anti-intervention drug has demonstrated clinical and economic effectiveness. Travoprost scored 1.92 QALYs (15% improvement in quality of life) over a 20-year period, and Tafluprost scored a slightly higher score of 1.99 QALYs (14.2% improvement in quality of life). The median ophthalmic costs for Tafluprost and Travoprost were 38,607 USD and 23,569 USD respectively. The authors concluded that Tafluprost is clinically effective for the treatment of patients with open-angle glaucoma, but is not cost effective compared to Travoprost. Moreover, sensitivity analyzes were also performed with upper and lower IOP limits at $95\%$ confidence intervals. Tafluprost remained with the best QALY scores among other interventions.
A study by Brown et al. (2019) showed that even though Travoprost is cheaper than Tafluprost, Tafluprost saves more social costs due to greater IOP lowering effect and more years of good vision. The main limitation of the study conducted by Brown is the lack of calculation of comparative economic efficiency (Incremental Cost Effectiveness Ratio, ICER) [4].
So, according to Brown et al. (2019), there is no calculation of the ICER indicator. In this regard, we calculated the ICER indicator and obtained:
$$
\begin{array}{l} \operatorname{ICER} = \operatorname{Cost} (1) - \operatorname{Cost} (2) / \operatorname{E f} (1) - \operatorname{E f} (2) = 1 9 2 5 - 9 4 4 / 1.9 9 - 1.9 2 \\= 1 4 0 1 4 \text{cost / QALY} \\\end{array}
$$
## IV. CONCLUSIONS
1. A review of clinical studies showed that the use of drugs from the group of prostaglandin analogues has a pronounced clinical efficacy. Travoprost has the most significant antihypertensive effect, Tafluprost show slightly less or approximately the same hypotensive activity.
2. Side effects from prescribing drugs - prostaglandin analogues do not have a significant impact on the quality of life of patients and their attitude to treatment. Tafluprost has the least side effects compared to Travoprost. The results of the review show that there is no significant statistical difference in the cost and effectiveness of treating POAG with both drugs.
3. A review of the economic literature on the treatment of primary open-angle glaucoma showed a paucity of economic evidence supporting the efficacy of treating POAG with Tafluprost compared with Travoprost.
Generating HTML Viewer...
References
15 Cites in Article
S Jalalov,Ch,D Jalalova,Kh,D Khoch (2012). The role of systematic review and meta-analysis in the evaluation of technologies in health care.
Iwasa Inoue,Tomita (2013). Effects of Tafluprost treatment for 3 years in patients with normal-tension glaucoma.
Kenji Inoue,Goji Tomita,Masato Wakakura,Mieko Masumoto (2012). Effects of BAK-free travoprost treatment for 3 years in patients with normal tension glaucoma.
G Brown,M Brown (2019). Patient Preference-Based Comparative Effectiveness and Cost-Utility Analysis of the Prostamides for Open-Angle Glaucoma.
Nice (2017). Glaucoma: Diagnosis and management.
S Jalalov,Ch,D Jalalova,Kh,D Khoch (2014). Conceptualization of a model for medical technology assessment.
S Dzhalalov,D Dzhalalova,M Krahn,J Hoch (2020). Incremental vs. average cost-effectiveness ratio: which one is preferable in health technology assessment?.
David Rein (2006). The Economic Burden of Major Adult Visual Disorders in the United States.
P Lichter (2001). Interim clinical outcomes in the collaborative initial glaucoma treatment study comparing initial treatment randomized to medications or surgery.
Anders Heijl (2002). Reduction of Intraocular Pressure and Glaucoma Progression.
Nice (2009). A new guideline to improve the diagnosis and management of chronic open angle glaucoma and ocular hypertension in the UK will be available from April 22.
Bryan Lee,Steven Kymes,Robert Nease,Walton Sumner,Carla Siegfried,Mae Gordon (2008). The Impact of Anchor Point on Utilities for 5 Common Ophthalmic Diseases.
Ricardo Paletta Guedes,Vanessa Paletta Guedes,Sirley Freitas,Alfredo Chaoubah (2015). Does the type of treatment have an influence on utility values in a glaucoma population?.
Vivek Adwe,Khurshed Bharucha,Atul Hegade,Rahul Deshpande,Madan Deshpande,Vk Kalyani (2016). Evaluation of skills transfer in short-term phacoemulsification surgery training program by International Council of Ophthalmology -Ophthalmology Surgical Competency Assessment Rubrics (ICO-OSCAR) and assessment of efficacy of ICO-OSCAR for objective evaluation of skills transfer.
A Liberati,D Altman,J Tetzlaff,C Mulrow,P Gotzsche,J Ioannidis,M Clarke,P Devereaux,J Kleijnen,D Moher (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Surayyo Z. Yuldasheva. 2026. \u201cSystematic Review of Clinical and Economic Evidence for Primary Open- Angle Glaucoma Therapy with Tafluprost vs Travoprost\u201d. Global Journal of Medical Research - F: Diseases GJMR-F Volume 22 (GJMR Volume 22 Issue F3).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































