## I. INTRODUCTION
Osteoarthritis (OA) is a localized and chronic joint disease that affects approximately one third of adults, with the prevalence of the disease increasing with advancing age[^1]. The economic impact of knee OA is also a growing problem for healthcare systems. Demographic predictions indicate that people over 65 will make up more than $20\%$ of the population by $2040^{2}$, so knee OA will only become more prevalent.
The knee is the most common site on the lower limb for OA, with the disease affecting the tibiofemoral and patellofemoral joints alone or in combination. The medial tibiofemoral compartment is the most commonly affected (67% medial versus 16% lateral)[^3]. Patients with knee OA often report symptoms of knee pain and difficulty with activities of daily living, such as walking, climbing stairs and household activities[^4]. Ultimately, the pain and disability associated with the disease lead to a loss of functional independence and a profound reduction in quality of life.
Knee OA treatment strategies can be considered as primary prevention (reduction of risk factors to reduce the incidence of the disease); secondary prevention (interventions to delay/prevent progression to serious illness) or; tertiary prevention (treatment of pain and disability) $^{5}$.
Given that there is currently no cure for knee OA and the only established treatment for end-stage OA is joint replacement, slowing the progression of structural disease is essential to help reduce the personal and social burden of knee OA. Traditionally, disease progression has been assessed by measuring joint space loss over time from serial radiographs. There is an increasing use of MRI to measure cartilage volume in the knee as it has proven to be a valid and reproducible technique that is more sensitive to change than x-rays $^6$.
Increased load on the joint is important in the pathogenesis of knee OA. Interventions that alter knee load can reduce symptoms and delay disease progression in patients with knee OA. The knee adduction moment determines the load distribution on the medial and lateral tibial plateaus, with a force in the medial compartment almost 2.5 times greater than the lateral[^7]. This may explain the much higher prevalence of medial OA compared to the lateral tibiofemoral joint.
The magnitude of this adduction moment is partially determined by the mechanical alignment of the knee. In medial knee OA, mechanical alignment becomes varus as the medial joint space narrows. Varus misalignment causes the ground reaction force vector to pass more medially to the center of the knee joint, resulting in a greater knee adduction moment. Cross-sectional studies demonstrate that patients with knee OA have a greater knee adduction moment during walking when compared to healthy controls of the same age[8,9].
Recent research has found that a longer adduction moment is associated with more intense pain in the knee $^{10}$ and greater severity of radiographic disease $^{11}$. The severity of knee misalignment is also significantly associated with the intensity of knee pain and physical function $^{12}$. Longitudinal studies have shown that a minimum increase of one unit at the time of adduction is associated with an increase of up to 6.5 times in the risk of disease progression $^{10,13}$. Likewise, varus misalignment of the knee joint is also correlated with disease progression $^{12,14,15}$. Given the importance of knee adduction timing and joint alignment in relation to symptom severity and disease progression in knee OA, conservative strategies to alter these biomechanical factors constitute a logical rehabilitation approach.
Alternatives to reduce the adductor moment using lateral wedges in the heels for alignment and demonstrated that insoles statically aligned the knee in a more upright position, shifting the calcaneus to a valgus position in relation to the tibia. Studies that such changes would help to reduce the excessive load on the medial articular surface, leading to knee pain mitigation.
Since then, biomechanical studies have evaluated the effects of lateral wedge insoles on knee alignment and medial compartment load. However, despite its biomechanical effects, few randomized clinical trials have evaluated its clinical efficacy $^{16-20,24-26}$.
We classified varus knees as mild varus with mechanical femorotibial angle $\leq 4^{\circ}$ and moderate with mechanical femorotibial angle $>4^{\circ}$.
Treatments with osteotomies $^{27}$, much more for corrections of genu varus than in valgus $^{28}$ with similar results even with moderate varus29.
Our objective is, focusing on knees with mild varus (femorotibial angle $< 4^{\circ}$ ), in addition to intra-articular corrections, perform ligamentopraxia (stretching by stretching by manipulation in valgus) of the medial complex, reducing the compression load on the medial compartment.
Evaluated preoperatively and postoperatively by X-Ray with monopodal support and Nuclear Magnetic Resonance, which qualified the femorotibial alignment and intra-articular lesions, as well as a specific and validated clinical questionnaire for the knee.
## II. MATERIAL AND METHODS
16 knees of 13 patients with medial meniscal injuries and femoro-tibial alignment to mild genu varus (femoral-tibial diaphyseal mechanical angle $< 4^{\circ}$ ), (Figure 1 A and 1 B).
 Fig. 1 B: Femorotibial angle Left knee 2o varus
Fig. 1 A: Femorotibial angle of right knee $3.5^{\circ}$ varus
Surgically treated within one year (from 8/13/2020 to 8/13/2021) by the same orthopedist, undergoing in addition to video arthroscopy for resolution of intra-articular lesions, ligamentopraxia of the medial complex (medial collateral ligament and posterior oblique ligament) (Figure 2).
 Fig. 2: Medial side of the knee with the medial collateral ligament and posterior oblique ligament. A redrawn from LaPrade, RF, Engebretsen AH, Ly TV, et al: The anatomy of the medial part of the knee. J Bone Joint Surg Am 89:2000, 2007.)
A valgus maneuver was performed at $20/30^{\circ}$ stabilized by the auxiliary in the thigh after intra-articular saline solution was insufflated in the video arthroscopy (Figure 3A and 3B).
 Fig. 3 A: Thigh stabilization
 Fig. 3 B: Valgus maneuver at $20/30^{\circ}$ of the knee lateralizing the leg with ligamentopraxia (stretching) of the medial complex
The radiographic femoro-tibial mechanical angles were calculated in AP with monopodal support and verified chondral and meniscal lesions in the pre
 Fig. 4 A: Postoperative MRI photograph showing a shortened medial meniscus in the sagittal section (reflecting the meniscoplasty) and edema with stretching of the medial collateral ligament in its proximal third of its superficial and deep leaflets.
and postoperative radiographic study of Nuclear Magnetic Resonance 30-32 (Figure 4A and 4B).
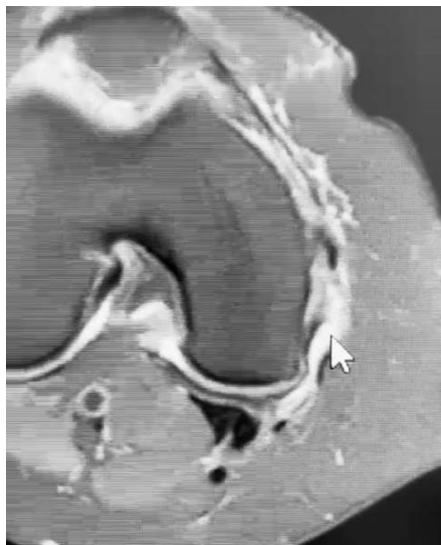 Fig. 4 B: Postoperative MRI photographs showing, in the axial section, in addition to the swelling with stretching of the superficial and deep medial collateral ligament, the oblique posterior ligament.
The Lyscholm $^{33}$ grading was used to assess the pre- and postoperative clinical evolution of the operated knees (Chart 1).
Table 1: Lyscholm scale score Limping (5 points) Never = 5 Mild or periodically = 3 Strong and continuous ☑0 Support (15 points) No support ☑0 Walking stick or crutches ☑2 Impossible ☑0 Restrainting (15 points) No restraining or restraining feeling ☑15 Has the feeling, but no restraining ☑10 Occasional restraining ☑6 Frequent ☑2 Joint restrained at examination ☑0 Instability (25 points) Never misses a step ☑25 Seldom, during athletic activities or other strong-effort exercises ☑20 Frequently during athletic activities or other strong-effort exercises (or unable to participate) ☑15 Occasionally in daily activities ☑10 Frequently in daily activities ☑5 At each step ☑0 Pain (25 points) No pain ☐ 25 Intermittent or mild during strong-effort exercises ☑ 20 Marked during strong-effort exercises ☑ 15 Marked during or after walking more than 2 Km ☑ 10 Marked during or after walking less than 2 Km ☑ 5 Continuous ☑ 0 Swelling (10 points) No swelling ☑ 10 Upon strong-effort exercises ☑ 6 Upon usual exercises ☑ 2 Continuous ☑5 Climbing stairs (10 points) No problem ☑ 10 Slightly damaged ☑6 One step at a time ☑ 2 Impossible ☑ 0 Squeezing (5 points) No problem ☑ 5 Slightly damaged ☑ 4 Not exceeding 60 degrees ☑ 2 Impossible ☑ 0 Total score: Score table: Excellent: 95 = 130; Good: 84 = 94; Fair: 65 = 83; Poor: < 64
<table><tr><td>Limping (5 points)<br>Never = 5<br>Mild or periodically = 3<br>Strong and continuous ☑0<br>Support (15 points)<br>No support ☑0<br>Walking stick or crutches ☑2<br>Impossible ☑0<br>Restrainting (15 points)<br>No restraining or restraining feeling ☑15<br>Has the feeling, but no restraining ☑10<br>Occasional restraining ☑6<br>Frequent ☑2<br>Joint restrained at examination ☑0<br>Instability (25 points)<br>Never misses a step ☑25<br>Seldom, during athletic activities or other strong-effort exercises ☑20<br>Frequently during athletic activities or other strong-effort exercises (or unable to participate) ☑15<br>Occasionally in daily activities ☑10<br>Frequently in daily activities ☑5<br>At each step ☑0<br><br>Pain (25 points)<br>No pain ☐ 25<br>Intermittent or mild during strong-effort exercises ☑ 20<br>Marked during strong-effort exercises ☑ 15<br>Marked during or after walking more than 2 Km ☑ 10<br>Marked during or after walking less than 2 Km ☑ 5<br>Continuous ☑ 0<br>Swelling (10 points)<br>No swelling ☑ 10<br>Upon strong-effort exercises ☑ 6<br>Upon usual exercises ☑ 2<br>Continuous ☑5<br>Climbing stairs (10 points)<br>No problem ☑ 10<br>Slightly damaged ☑6<br>One step at a time ☑ 2<br>Impossible ☑ 0<br>Squeezing (5 points)<br>No problem ☑ 5<br>Slightly damaged ☑ 4<br>Not exceeding 60 degrees ☑ 2<br>Impossible ☑ 0<br>Total score:<br><br>Score table: Excellent: 95 = 130; Good: 84 = 94; Fair: 65 = 83; Poor: < 64</td></tr></table>
## III. RESULTS
The procedures were performed in 12 patients (8 females and 4 males) in 16 knees (10 right knees and 6 left) bilateral ones were two females and two males (Table 1).
The femorotibial mechanical angle ranged from $3^{\circ}$ of Valgus to $4^{\circ}$ of Varus (weighted average of $0.41^{\circ}$ of Varus).
The internal lesions involved grade III medial meniscus $^{30,31}$ and grade I to IV medial chondral lining $^{32}$.
<table><tr><td>pat</td><td>ag</td><td>gen</td><td>site</td><td>f/tà</td><td>mri pré</td><td>lysholm pré</td><td>lysholm pós</td></tr><tr><td>mtbr</td><td>55</td><td>fem</td><td>rig</td><td>vr 2°</td><td>m iii ciii</td><td>25</td><td>93</td></tr><tr><td>mtbr</td><td>55</td><td>fem</td><td>lef</td><td>vr 2°</td><td>m iii cii</td><td>25</td><td>93</td></tr><tr><td>jwc</td><td>86</td><td>mal</td><td>rig</td><td>vl 3°</td><td>miii ciii</td><td>18</td><td>87</td></tr><tr><td>jwc</td><td>86</td><td>mal</td><td>lef</td><td>vl 2°</td><td>miii ciii</td><td>18</td><td>87</td></tr><tr><td>rcc</td><td>64</td><td>mal</td><td>lef</td><td>vr 4°</td><td>miii civ</td><td>42</td><td>99</td></tr><tr><td>moa</td><td>71</td><td>fem</td><td>tig</td><td>vr 0</td><td>miii civ</td><td>19</td><td>94</td></tr><tr><td>rvmc</td><td>65</td><td>fem</td><td>rig</td><td>vl2°</td><td>m iii ciii</td><td>17</td><td>99</td></tr><tr><td>oow</td><td>76</td><td>mal</td><td>rig</td><td>0°</td><td>m iii cii</td><td>57</td><td>95</td></tr><tr><td>oow</td><td>76</td><td>mal</td><td>lef</td><td>vr 1°</td><td>m iii cii</td><td>57</td><td>93</td></tr><tr><td>dp</td><td>58</td><td>mal</td><td>lef</td><td>vr 2°</td><td>m iii ciii</td><td>25</td><td>99</td></tr><tr><td>ats</td><td>57</td><td>fem</td><td>rig</td><td>vr 1°</td><td>m iii cii</td><td>34</td><td>92</td></tr><tr><td>nca</td><td>68</td><td>fem</td><td>rig</td><td>vl 2°</td><td>m iii ciii</td><td>57</td><td>89</td></tr><tr><td>rci</td><td>63</td><td>fem</td><td>rig</td><td>vl 1°</td><td>m iii ciii</td><td>40</td><td>95</td></tr><tr><td>cmg</td><td>66</td><td>fem</td><td>rig</td><td>vr3,5°</td><td>miii civ</td><td>47</td><td>98</td></tr><tr><td>msb</td><td>72</td><td>fem</td><td>rig</td><td>0°</td><td>miii cii</td><td>12</td><td>98</td></tr><tr><td>msb</td><td>72</td><td>fem</td><td>lef</td><td>vr 1°</td><td>miii civ</td><td>12</td><td>98</td></tr></table>
<table><tr><td>pat</td><td>ag</td><td>gen</td><td>site</td><td>f/tà</td><td>mri pré</td><td>lysholm pré</td><td>lysholm pós</td></tr><tr><td>mtbr</td><td>55</td><td>fem</td><td>rig</td><td>vr 2°</td><td>m iii ciii</td><td>25</td><td>93</td></tr><tr><td>mtbr</td><td>55</td><td>fem</td><td>lef</td><td>vr 2°</td><td>m iii cii</td><td>25</td><td>93</td></tr><tr><td>jwc</td><td>86</td><td>mal</td><td>rig</td><td>vl 3°</td><td>miii ciii</td><td>18</td><td>87</td></tr><tr><td>jwc</td><td>86</td><td>mal</td><td>lef</td><td>vl 2°</td><td>miii ciii</td><td>18</td><td>87</td></tr><tr><td>rcc</td><td>64</td><td>mal</td><td>lef</td><td>vr 4°</td><td>miii civ</td><td>42</td><td>99</td></tr><tr><td>moa</td><td>71</td><td>fem</td><td>tig</td><td>vr 0</td><td>miii civ</td><td>19</td><td>94</td></tr><tr><td>rvmc</td><td>65</td><td>fem</td><td>rig</td><td>vl2°</td><td>m iii ciii</td><td>17</td><td>99</td></tr><tr><td>oow</td><td>76</td><td>mal</td><td>rig</td><td>0°</td><td>m iii cii</td><td>57</td><td>95</td></tr><tr><td>oow</td><td>76</td><td>mal</td><td>lef</td><td>vr 1°</td><td>m iii cii</td><td>57</td><td>93</td></tr><tr><td>dp</td><td>58</td><td>mal</td><td>lef</td><td>vr 2°</td><td>m iii ciii</td><td>25</td><td>99</td></tr><tr><td>ats</td><td>57</td><td>fem</td><td>rig</td><td>vr 1°</td><td>m iii cii</td><td>34</td><td>92</td></tr><tr><td>nca</td><td>68</td><td>fem</td><td>rig</td><td>vl 2°</td><td>m iii ciii</td><td>57</td><td>89</td></tr><tr><td>rci</td><td>63</td><td>fem</td><td>rig</td><td>vl 1°</td><td>m iii ciii</td><td>40</td><td>95</td></tr><tr><td>cmg</td><td>66</td><td>fem</td><td>rig</td><td>vr3,5°</td><td>miii civ</td><td>47</td><td>98</td></tr><tr><td>msb</td><td>72</td><td>fem</td><td>rig</td><td>0°</td><td>miii cii</td><td>12</td><td>98</td></tr><tr><td>msb</td><td>72</td><td>fem</td><td>lef</td><td>vr 1°</td><td>miii civ</td><td>12</td><td>98</td></tr></table>
## IV. DISCUSSION
The prevalence of knee OA has increased significantly in recent decades and continues to increase, and age, previous knee injuries, obesity (increased body mass index (BMI), joint misalignment and instability resulting in increased mechanical stress are all strong factors. risk for developing knee OA $^{34-38}$
Physical inactivity is also another important contributor to the increased prevalence of OA, causing greater susceptibility to knee injuries due to less stable and weaker joints $^{39}$. However, weakness of the knee extensor muscles appears to be a weak risk factor, compared to previous knee injuries $^{40}$.
Men are less likely to develop OA than women, making sex one of the risk factors associated with developing OA40. Narrower femurs, thinner patellas, larger quadriceps angles and differences in the size of the tibial condyles make women's knee anatomy different from men's, leading to different kinematics, which influence females to be more likely to develop OA, leading to a higher prevalence of OA in women41,42.
In this study, we selected patients with meniscal injuries associated with knees with varus less than $4^{\circ}$, grade III meniscal injuries and varied chondral injuries.
In our sample, we had an average age of 68.13 years (55 to 86 years) being more prevalent in females, $66.67\%$ of operated knees, which is in agreement with the literature[43].
The gradation of the tibial femur anatomical angle was $0.41^{\circ}$ of varus (ranging from $3^{\circ}$ of valgus to $4^{\circ}$ of varus). Respecting the 4th of varus to be considered light varus. Literature agrees that from Moderate Varism (greater than $4^{\circ}$ ) the indications for osteotomies and arthroplasties would be of better therapeutic indication.
Meniscal injuries were all grade III, those without chondral or chondral injuries were type I $2\%$, type II $35.5\%$, type III $37.5\%$ and type IV $25\%$.
All treated by the same surgeon, with meniscoplasty of the medial meniscus being performed by resection only of the injured area, respecting the maximum amount of intact tissue, chondroplasty by toilet or microfractures when necessary.
Preoperative Lysholm Scorres had a Weighted Average of 31.56 (13 to 57) and all qualified on the score as poor. In the evaluation by the same Score in the Postoperative period, the knees had a Weighted Average of 94.31 (87 to 99) 9 knees had a score as good and 6 as excellent.
Very positive results were obtained for the patients followed.
The purpose of this article serves as a presentation of this technique of ligamentopraxia of the medial collateral complex.
Specific videoarthroscopic meniscoplasty and chondroplasty are always performed for patients with femoro-tibial misalignment with varus to moderate.
## V. CONCLUSION
In knees with moderate varus, the technique aims to improve the medial femoro-tibial conflict through the ligamentopraxia of the medial complex (medial collateral ligament and posterior oblique ligament).
Associated with the specific treatment of meniscal and chondral injuries, it improved the pre-topostoperative score from 31.56 to 94.31 points.
As the technique is unprecedented, its efficacy and replicability must be observed with further studies.
Generating HTML Viewer...
References
44 Cites in Article
David Felson,Allan Naimark,Jennifer Anderson,Lewis Kazis,William Castelli,Robert Meenan (1987). The prevalence of knee osteoarthritis in the elderly. the framingham osteoarthritis study.
D Hamerman (1995). Clinical implications of osteoarthritis and ageing..
J Ledingham,M Regan,A Jones,M Doherty (1993). Radiographic patterns and associations of osteoarthritis of the knee in patients referred to hospital..
A Guccione,D Felson,J Anderson,J Anthony,Y Zhang,Pwf Wilson,M Kelly-Hayes,P Wolf,B Kreger,W Kannel (1994). The effects of specific medical conditions on the functional limitations of elders in the Framingham study.
Paul Dieppe,Kenneth Brandt (2003). What is important in treating osteoarthritis? Whom should we treat and how should we treat them?.
Felix Eckstein,Michael Schnier,Michael Haubner,J??rgen Priebsch,Christian Glaser,Karl-Hans Englmeier,Maximilian Reiser (1998). Accuracy of Cartilage Volume and Thickness Measurements With Magnetic Resonance Imaging.
O Schipplein,T Andriacchi (1991). Interaction between active and passive knee stabilizers during level walking.
A Baliunas,D Hurwitz,A Ryals,A Karrar,J Case,J Block,T Andriacchi (2002). Increased knee joint loads during walking are present in subjects with knee osteoarthritis.
D Hurwitz,A Ryals,J Case,J Block,T Andriacchi (2002). The knee adduction moment during gait in subjects with knee osteoarthritis is more closely correlated with static alignment than radiographic disease severity, toe out angle and pain.
T Miyazaki,M Wada,H Kawahara,M Sato,H Baba,S Shimada (2002). Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis.
L Sharma,D Hurwitz,E Thonar,J Sum,M Lenz,D Dunlop,T Schnitzer,G Kirwanmellis,T Andriacchi (1998). Knee Adduction Moment, Serum Hyaluronan Level, and Disease Severity in Medial Tibiofemoral Osteoarthritis.
Leena Sharma,J Song,D Felson,Sbs Cahue,Ems Shamiyeh,D Dunlop (2001). The Role of Knee Alignment in Disease Progression and Functional Decline in Knee Osteoarthritis.
L Sharma,D Dunlop,T Andriacchi,K Hayes,J Song,S Cahue,A Ryals,A Chang,D Hurwitz (2003). The adduction moment and knee osteoarthritis (OA): a longitudinal study.
Rui Cerejo,Dorothy Dunlop,September Cahue,David Channin,Jing Song,Leena Sharma (2002). The influence of alignment on risk of knee osteoarthritis progression according to baseline stage of disease.
F Cicuttini,A Wluka,J Hankin,Y Wang (2004). Longitudinal study of the relationship between knee angle and tibiofemoral cartilage volume in subjects with knee osteoarthritis.
Tetsuto Sasaki,Kazunori Yasuda (1987). Clinical Evaluation of the Treatment of Osteoarthritic Knees Using a Newly Designed Wedged Insole.
Kazunori Yasuda,Tetsuto Sasaki (1987). The Mechanics of Treatment of the Osteoarthritic Knee with a Wedged Insole.
K Ogata,M Yasunaga,H Nomiyama (1997). The effect of wedged insoles on the thrust of osteoarthritic knees.
S Crenshaw,F Pollo,E Calton (2000). Effects of lateralwedged insoles on kinetics at the knee.
D Kerrigan,Jennifer Lelas,Joyce Goggins,Greg Merriman,Robert Kaplan,David Felson (2002). Effectiveness of a lateral-wedge insole on knee varus torque in patients with knee osteoarthritis.
Robert Butler,Stephanie Marchesi,Todd Royer,Irene Davis (2007). The effect of a subject‐specific amount of lateral wedge on knee mechanics in patients with medial knee osteoarthritis.
J Giffin,William Stanish,Scott Mackinnon,Donald Macleod (1995). Application of a Lateral Heel Wedge as a Nonsurgical Treatment for Varum Gonarthrosis.
J Maillefert,C Hudry,G Baron,P Kieffert,P Bourgeois,D Lechevalier,A Coutaux,M Dougados (2001). Laterally elevated wedged insoles in the treatment of medial knee osteoarthritis: a prospective randomized controlled study.
T Pham,J-F Maillefert,C Hudry,P Kieffert,P Bourgeois,D Lechevalier,M Dougados (2003). Laterally elevated wedged insoles in the treatment of medial knee osteoarthritis.
Kristin Baker,Joyce Goggins,Hui Xie,Karen Szumowski,Michael Lavalley,David Hunter,David Felson (2007). A randomized crossover trial of a wedged insole for treatment of knee osteoarthritis.
Kim Bennell,Kelly-Ann Bowles,Craig Payne,Flavia Cicuttini,Richard Osborne,Anthony Harris,Rana Hinman (2007). Effects of laterally wedged insoles on symptoms and disease progression in medial knee osteoarthritis: a protocol for a randomised, double-blind, placebo controlled trial.
Haining Peng,Aichun Ou,Xiaohong Huang,Chen Wang,Lei Wang,Tengbo Yu,Yingze Zhang,Yi Zhang (2021). Osteotomy Around the Knee: The Surgical Treatment of Osteoarthritis.
Gunter Spahn,Jürgen Fritz,Dirk Albrecht,Peter Angele,Stefan Fickert,Matthias Aurich,Gunther Hofmann,Phillip Niemeyer (2017). Koinzidenz und Therapie von Beinachsdeviationen bei degenerativen Knorpelschäden des Kniegelenks. Ergebnisse aus dem Deutschen KnorpelRegister DGOU.
Young Na,Beom Lee,Do Hwang,Eun Choi,Jae Sim (2018). Can osteoarthritic patients with mild varus deformity be indicated for high tibial osteotomy?.
Jae Ang,Sim (2018). Unknown Title.
J Crues,J Mink,T Levy,M Lotysch,D Stoller (1987). Meniscal tears of the knee: accuracy of MR imaging..
D Stoller,C Martin,J Crues,L Kaplan,J Mink (1987). Meniscal tears: pathologic correlation with MR imaging..
M Rodrigues (2010). CamanhoGL Avaliação da cartilagem do joelho pela ressonância magnética.
Maria Peccin,Rozana Ciconelli,Moisés Cohen (2006). Questionário específico para sintomas do joelho "Lysholm Knee Scoring Scale": tradução e validação para a língua portuguesa.
Sung-Do Cho,Yoon-Seok Youm,Jong-Hyun Kim,Hye-Yong Cho,Kwang-Ho Kim (2016). Patterns and Influencing Factors of Medial Meniscus Tears in Varus Knee Osteoarthritis.
Uyen-Sa D. T. Nguyen,Yuqing Zhang,Yanyan Zhu,Jingbo Niu,Bin Zhang,David Felson (2011). Increasing Prevalence of Knee Pain and Symptomatic Knee Osteoarthritis: Survey and Cohort Data.
Shane Anderson,A Loeser,R (2010). Why is osteoarthritis an age-related disease? Best.
D Felson (2013). Osteoarthritis as a disease of mechanics.
Ernest Vina,C Kwoh (2018). Epidemiology of osteoarthritis: literature update.
Francis Berenbaum,Ian Wallace,Daniel Lieberman,David Felson (2018). Modern-day environmental factors in the pathogenesis of osteoarthritis.
David Hunter,Sita Bierma-Zeinstra (2019). Osteoarthritis.
Sharon Hame,Reginald Alexander (2013). Knee osteoarthritis in women.
Huibin Long,Xinying Zeng,Qiang Liu,Haidong Wang,Theo Vos,Yunfei Hou,Chutong Lin,Yudian Qiu,Kai Wang,Dan Xing,Yuqing Zhang,Maigeng Zhou,Jianhao Lin (2020). Burden of osteoarthritis in China, 1990–2017: findings from the Global Burden of Disease Study 2017.
Yuqing Zhang,Joanne Jordan (2010). Epidemiology of Osteoarthritis.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Dr. Marco Antonio Schueda Dr. Marco Antonio Schueda. 2026. \u201cLigamentopraxia of the Medial Complex in Knees with Medial Conflict\u201d. Global Journal of Medical Research - H: Orthopedic & Musculoskeletal System GJMR-H Volume 23 (GJMR Volume 23 Issue H1).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.