## I. INTRODUCTION
Amputation has a profound and long-lasting impact on an individual's economic, psychological, and social status [1, 2]. Complications arising from various peripheral vascular diseases and, or diabetes form the most important causes of amputations [3, 4]. However, traumatic experiences at the extremities and, to a lesser extent, cancer, as well as other causes, also have a role.[5]. Studies have shown that age and gender play a significant role in the pattern of limb loss [6, 7]. Older adults with several chronic conditions are disproportionately affected by limb loss due to peripheral vascular disease, while young men are disproportionately affected by limb loss due to trauma. [8, 9]. Most patients requiring prosthetic restoration and rehabilitation services are older adults with lower limb amputations due to vascular disease[10]. The lifetime risk of amputation in the elderly is $10 - 15\%$, 10-30 times higher than in the general population[11]. Additionally, reports indicate that amputations caused by trauma and cancer may be decreasing, whereas congenital amputations remain stable [12]. Diabetes is responsible for at least $50\%$ of non-traumatic lower-limb amputations worldwide, according to studies [13]. The prevalence of amputations performed has been rising worldwide [14]. In the United States, lower limb loss was estimated to affect 1.6 million people in 2005, with that figure expected to more than double to 3.6 million by 2050 [15]. The studies regarding amputation among countries in Asia have many similarities, as trauma and disease incidence occur in similar patterns [16, 17]. In contrast, the patterns are not the same as those in the United States, Denmark, Finland, or Australia [18], where peripheral vascular disorders, notably arteriosclerosis, are the most common cause of amputations. In these countries, the patterns differ. There has been a paucity of research published about the prevalence of amputees in Saudi Arabia. A 14-year retrospective study published in 1993 for the amputee population in Saudi Arabia was a comprehensive study listing all cases of amputations in a particular rehabilitation center in Riyadh, Saudi Arabia, from 1977 to 1990 [19]. In 2012, Alzahrani, in his study, concluded that around half a million amputations of the lower extremities would likely occur in Saudi Arabia and other Middle East and North African countries, and this number includes only amputations arising out of diabetic complications [20]. Whether so many diabetes-related amputations have occurred in the last decade is difficult to assess, the primary reason being the lack of a national registry of amputations in Saudi Arabia and limited such published reports, which still represents a significant challenge for healthcare policymakers [19, 21]. This study was thus designed to fill up some of these gaps in the literature.
In Saudi Arabia, the number of people with peripheral vascular diseases, diabetes, and people who die in car accidents is also going up [22, 23]. So, it may have also led to a rise in the number of amputations in this country. More data needs to be published to assess better the etiology, characteristics, and risk factors for amputation in this country. This may assist healthcare providers in planning and establishing effective and timely interventions and may also help improve rehabilitation services so that amputee patients can be functionally independent and productive members of their communities. This fact has increased the interest in studying the impact of etiology, characteristics, and clinical status on amputees. Besides, identifying the etiology, the study aimed to identify the characteristics and risk factors for amputation cases in Saudi Arabia.
## II. METHODS
This investigation is a retrospective hospital-based study with 1409 amputee patients' data collected between June 2010 to June 2020. Sultan bin Abdul Aziz Humanitarian City (SBAHC), a tertiary care rehabilitation center, adopted proper evaluation management and quality of life assessment for its clients where we conducted this study. All amputees' medical records were evaluated by medical coders at the Research facility at SBAHC using a pre-designed case report form to determine the pattern of amputations and etiological factors. Inclusion criteria included all patients with amputations who visited outpatient limb loss clinics. The exclusion criteria included the patients whose medical records were incomplete during the study period regardless of the level, site, or type of amputation. Collected data included demographic variables, etiology, site, level, and type of amputations. In addition, the cohort distribution from different provinces, namely Central, Northern, Southern, Eastern, and Western, was collected in addition to patient nationality. This study was approved by the Institutional Review Board of SBAHC.
Out of the selected cohort, 618 patients were required to be admitted because of pre- and postprosthetic rehabilitation. The functional outcomes of the cohort were evaluated based on the functional independent measurement score (FIM Score) at admission and six months after discharge. Clinical evaluation in weight, height, BMI, and systolic/diastolic blood pressure was also collected from the patient's medical files. Progress with rehabilitation, if any, was recorded during the follow-up. The FIM instrument contains 18 items classified into six major scales: self-care, sphincter control, transfer, locomotion, communication, and social cognition [24, 25]. These interviews at admission and discharge were conducted by a team of medical doctors, physical therapists, and nurses on the guidelines laid down by the Center. On each item, the patients rated their level of independence using a 1–7 scale, on which one (1) means assistance was needed, and seven (7) means a person was entirely independent.
Statistical analysis of the data collected from the study was analyzed using SPSS ver. 22 (IBM, Armonk, NY, USA). For continuous normal variables, the data were provided as the mean and standard deviation, whereas for continuous non-normal variables, the data were shown as the median (Q1-Q3). The frequency of each subject was determined based on their distribution according to etiology, age, and level of amputation, and the results were reported as a percentage. A $P$ -value of $< 0.05$ was considered significant. For rehabilitation data, 618 subjects were interviewed before admission and at discharge using a self-reported version of the FIM instrument. Summing up responses to each item gave us a scale score ranging from several items to seven times the number of items, i.e., the total FIM score ranges from 18 to 126. FIM improvement $(\%)$ was calculated by subtracting FIM at admission from FIM at discharge, and this score served as an outcome measure in the study.
## III. RESULTS
### a) Demographic characteristics of the Study Subjects
The demographic characteristics of the study subjects are presented in table 1. A total of 1409 patients were recruited, of which $75.6\%$ were male and $24.4\%$ were female. The patients' ages ranged from 1 to 96 years, with the average male age being 45 years and the average female age being 36 years. Out of the total population studied, Saudi nationals constituted $86.9\%$ $(n = 1224)$, and the rest were non-Saudi $(n = 185,13.1\%)$. Most of the studied population $(n = 849,60.3\%)$ was from the Central region of Saudi Arabia, followed by the Western $(n = 235,16.7\%)$, Southern $(n = 160,11.4\%)$, and other regions. Most amputees were affected by vascular and traumatic amputations $(n = 597,42.4\%)$ and $n = 519,36.9\%$ respectively), followed by congenital
$(n = 204,14.4\%)$ and infection/others. The study cohort consists of patients with a duration of amputation of 5 years or less $(n = 566,40.4\%)$, followed by 6-10 years (n=417, 29.7%). Among comorbidities, the most prevalent was diabetes (n=570, 40.5%), followed by hypertension (n=370, 26.3%).
Table 1: Demographic Characteristics of study subjects
<table><tr><td colspan="2">Total</td><td>All (1409)</td><td>Males (1066)</td><td>Females (343)</td><td>P-value</td></tr><tr><td colspan="2">Age Mean (SD)</td><td>43 (21)</td><td>45 (20.8)</td><td>36 (20.0)</td><td><.001</td></tr><tr><td rowspan="2">Nationality N (%)</td><td>Saudi</td><td>1224 (86.8)</td><td>920 (75.1)</td><td>304 (24.9)</td><td><.001</td></tr><tr><td>Non-Saudi</td><td>185 (13.1)</td><td>146 (78.9)</td><td>39 (21.1)</td><td><.001</td></tr><tr><td rowspan="5">Province N (%)</td><td>Central</td><td>849 (60.2)</td><td>650 (76.5)</td><td>199 (23.5)</td><td><.001</td></tr><tr><td>Northern</td><td>59 (4.1)</td><td>37 (62.7)</td><td>22 (37.3)</td><td>.006</td></tr><tr><td>Southern</td><td>160 (11.3)</td><td>126 (78.7)</td><td>34 (21.3)</td><td><.001</td></tr><tr><td>Western</td><td>235 (16.6)</td><td>181 (77.1)</td><td>54 (22.9)</td><td><.001</td></tr><tr><td>Eastern</td><td>106 (7.5)</td><td>72 (67.9)</td><td>34 (32.1)</td><td><.001</td></tr><tr><td rowspan="4">Etiology N (%)</td><td>Trauma</td><td>519 (36.8)</td><td>425 (81.8)</td><td>94 (18.2)</td><td><.001</td></tr><tr><td>Vascular</td><td>597 (42.3)</td><td>479 (80.2)</td><td>118 (19.8)</td><td><.001</td></tr><tr><td>Congenital</td><td>204 (14.4)</td><td>109 (53.4)</td><td>95 (46.6)</td><td>.16</td></tr><tr><td>Infection</td><td>89 (6.3)</td><td>53 (59.5)</td><td>36 (40.5)</td><td>.01</td></tr><tr><td rowspan="5">Duration of amputation N (%)</td><td>≤5</td><td>566 (40.3)</td><td>447 (78.9)</td><td>119 (21.1)</td><td><.001</td></tr><tr><td>6 - 10</td><td>417 (29.6)</td><td>329 (78.8)</td><td>88 (21.2)</td><td><.001</td></tr><tr><td>11-15</td><td>186 (13.2)</td><td>137 (73.6)</td><td>49 (26.4)</td><td><.001</td></tr><tr><td>16 - 20</td><td>84 (5.9)</td><td>55 (65.4)</td><td>29 (34.6)</td><td><.001</td></tr><tr><td>>20</td><td>152 (10.7)</td><td>95 (62.5)</td><td>57 (37.5)</td><td><.001</td></tr><tr><td rowspan="5">Comorbidity N (%)</td><td>Diabetes</td><td>570 (40.4)</td><td>468 (82.1)</td><td>102 (17.9)</td><td><.001</td></tr><tr><td>Hypertension</td><td>370 (26.2)</td><td>301 (81.5)</td><td>69 (18.5)</td><td><.001</td></tr><tr><td>Hyperlipidemia</td><td>74 (5.2)</td><td>63 (85.1)</td><td>11 (14.9)</td><td><.001</td></tr><tr><td>Cardiac</td><td>118 (8.3)</td><td>102 (86.4)</td><td>16 (13.6)</td><td><.001</td></tr><tr><td>Others</td><td>277 (19.6)</td><td>193 (69.6)</td><td>84 (30.4)</td><td><.001</td></tr><tr><td colspan="2">Weight Mean (SD)</td><td>72.5 (32.4)</td><td>72.4 (32.4)</td><td>62.8 (31.7)</td><td><.001</td></tr><tr><td colspan="2">Height Mean (SD)</td><td>158.5 (54.6)</td><td>158.50 (54.6)</td><td>146.5 (48.3)</td><td><.001</td></tr><tr><td colspan="2">BMI Mean (SD)</td><td>30.2 (12.5)</td><td>30.58 (12.5)</td><td>26.9 (12.3)</td><td>.03</td></tr><tr><td colspan="2">Systolic Blood Pressure Mean (SD)</td><td>125.9 (42.5)</td><td>128.9 (42.5)</td><td>120.6 (49.1)</td><td><.001</td></tr><tr><td colspan="2">Diastolic Blood Pressure Mean (SD)</td><td>76.3 (24.8)</td><td>76.3 (24.8)</td><td>74.5 (22.7)</td><td>0.47</td></tr></table>
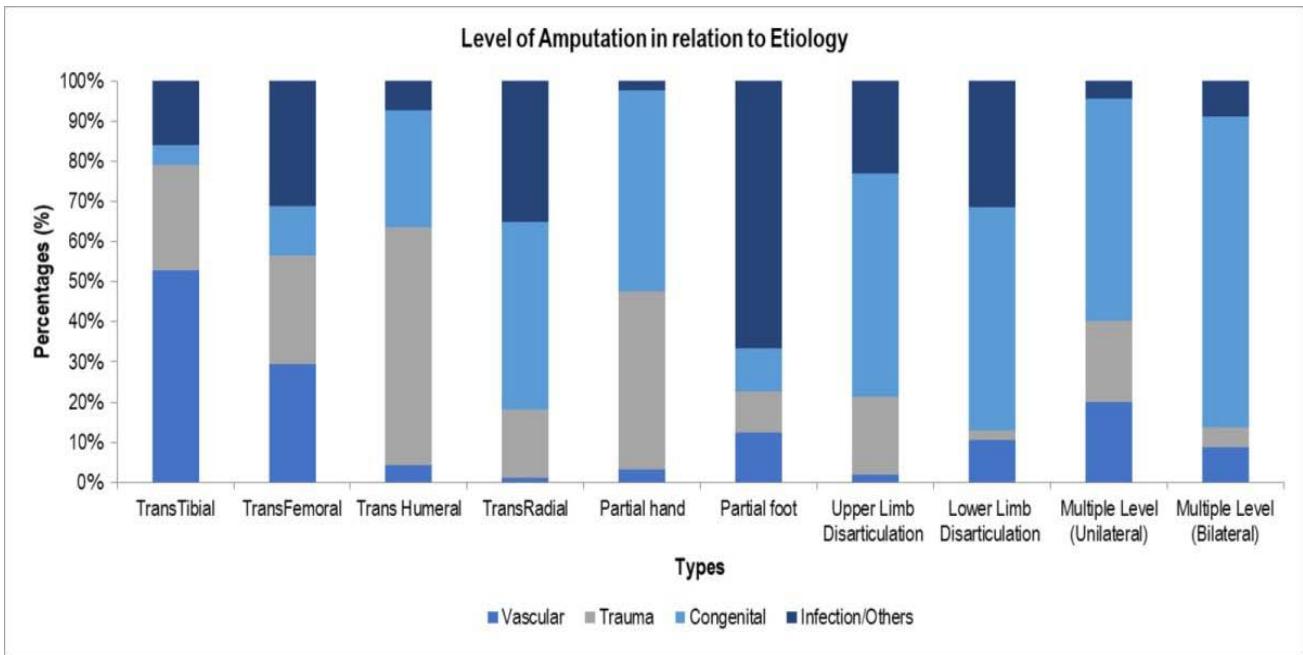
When comparing the level of amputation with etiology, trans-tibial amputations were found to be the highest (135/597, $22.6\%$ ), followed by trans-femoral amputations (84/597, $14.1\%$ ) in the case of patients with vascular diseases. Among trauma patients, trans-femoral amputation was the highest (53/519, $10.9\%$ ), followed by transtibial (50/519, $9.6\%$ ). The amputation level among congenital cases was highest in the case of trans-radial $(2.4\%)$, followed by partial hand $(1.8\%)$ and trans-femoral $(1.6\%)$ (Figure 1).
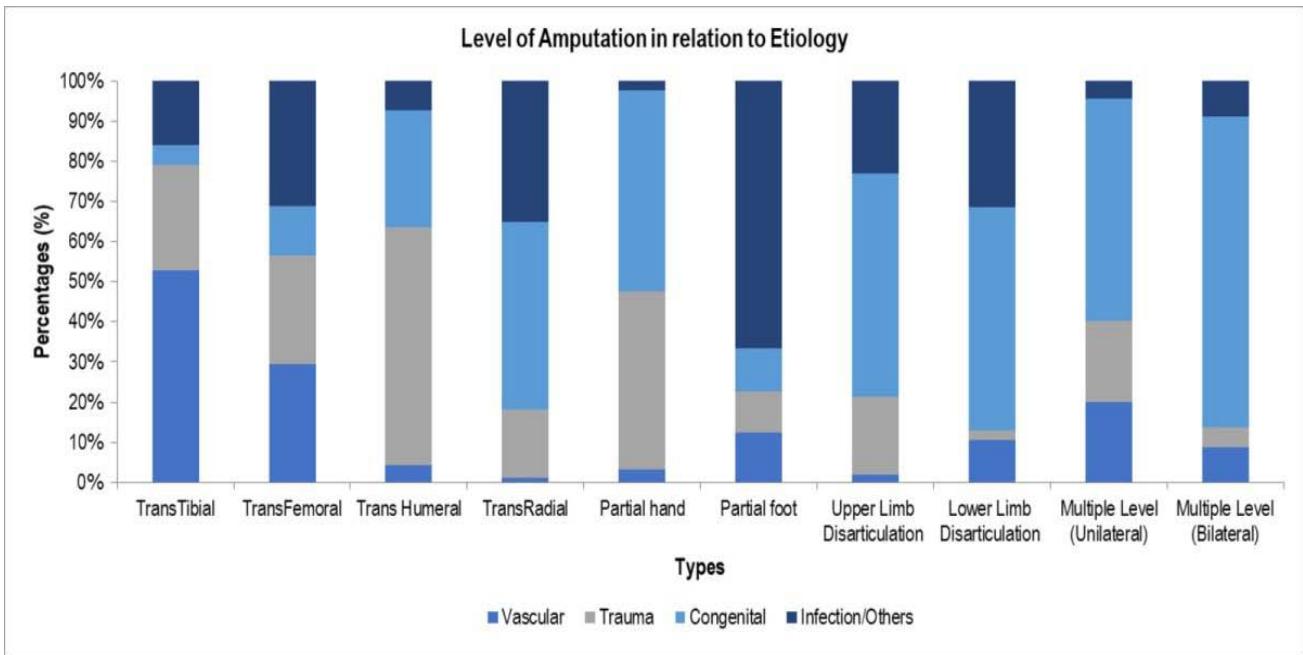 Figure 1: Level of amputation according to etiology.
### b) Etiology
When comparing the etiology of amputation with life span (Figure 2), we found that trauma-related amputation cases were highest in the age group between 21 to 30 years (359/519, $69.2\%$ ) and lowest in people over 70 years of age (36/519, $7\%$ ).
Amputations due to vascular disease were most common in those aged 70 and older (534/597, $89.5\%$ ) and least common in children aged 0-10 (23/597, $3.9\%$ ). Congenital amputation was, as expected, most frequent in the age group 0-10 years (162/204, $79.4\%$ ) and was least in the age group 51-60 years (1/204, $0.5\%$ ).
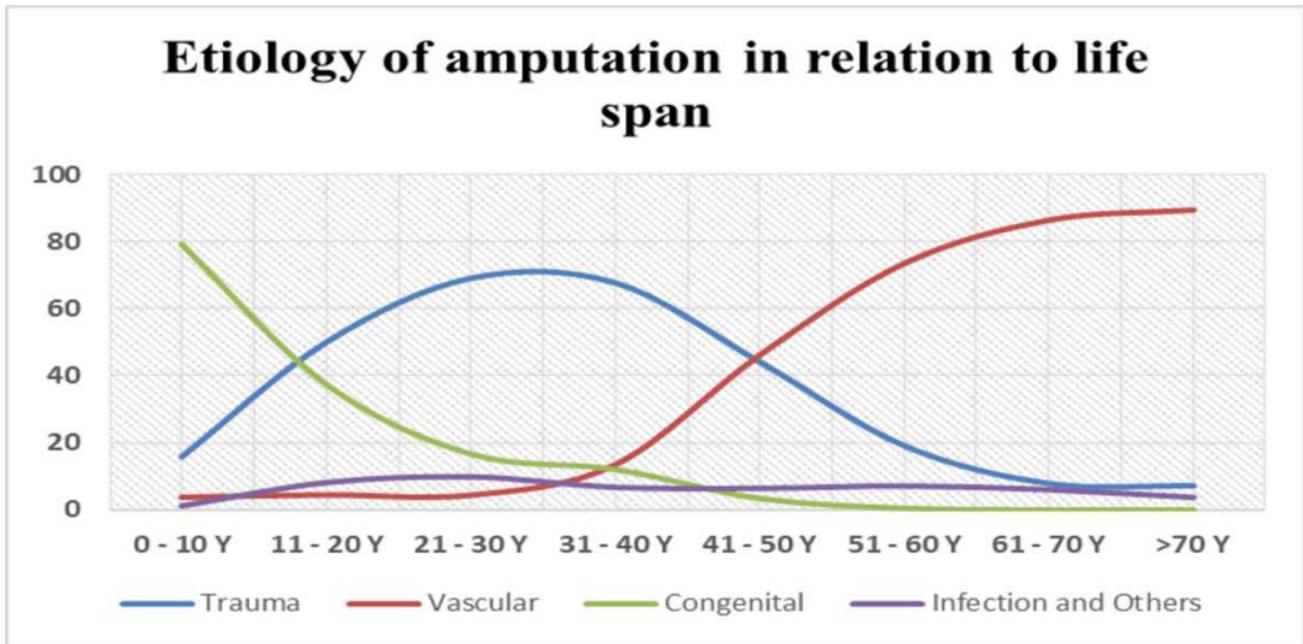 Figure 2: Etiology of amputation according to life span.
### c) Improvement in FIM scores
Admission and discharge FIM score data were presented in Table 2. There is a significant difference $(P=.005)$ between admission and discharge scores in self-care, transfer, and locomotion (all $P$ -values $<.001$ ). Also, the overall FIM score improved 6 months postdischarge as compared to the admission $(P <.001)$. FIM showed a maximum improvement in the case of locomotion (score of 6.4 at admission to 10.8 at discharge out of a total of 14, an increase of $33.6\%$, $P <.001$ ), followed by transfer and self-care. An improvement of $15.1\%$ was also found in the total FIM score, which increased from 89.8 to 107.5 out of the maximum score of 126.
Table 2: Patient's functional status according to Functional Independence Measurement (FIM) Score value from admission to discharge
<table><tr><td>FIM Scale Mean (SD)</td><td>Admission</td><td>Discharge</td><td>P-value</td><td>Max Score</td><td>Admission (% score)</td><td>Discharge (% score)</td><td>Improvement (%)</td></tr><tr><td>Self-care</td><td>29.6 (0.5)</td><td>36.6 (0.3)</td><td><.001</td><td>42</td><td>71.4</td><td>87.8</td><td>16.4</td></tr><tr><td>Sphincter- Control</td><td>12.5(0.2)</td><td>12.5 (0.2)</td><td>.34</td><td>14</td><td>88.0</td><td>91.8</td><td>3.8</td></tr><tr><td>Transfer</td><td>11.0 (0.4)</td><td>17.3 (0.2)</td><td><.001</td><td>21</td><td>52.6</td><td>83.2</td><td>30.6</td></tr><tr><td>Locomotion</td><td>6.4 (0.3)</td><td>10.8 (0.2)</td><td><.001</td><td>14</td><td>45.9</td><td>79.5</td><td>33.6</td></tr><tr><td>Communication</td><td>13.6 (0.1)</td><td>13.7 (0.1)</td><td>.19</td><td>14</td><td>97.6</td><td>98.8</td><td>1.2</td></tr><tr><td>Social-Cognition</td><td>20.3 (0.1)</td><td>20.4 (0.1)</td><td>.29</td><td>21</td><td>97.0</td><td>97.9</td><td>0.9</td></tr><tr><td>Total FIM</td><td>89.8 (1.2)</td><td>107.5 (1.1)</td><td><.001</td><td>126</td><td>74.4</td><td>89.5</td><td>15.1</td></tr></table>
## IV. DISCUSSION
This study aimed to present our experiences with major limb amputations in Saudi Arabia and compare the results to those of similar studies conducted in other regions of the world. The purpose of this comparison was to highlight the differences in the pattern and indications for amputations and suggest relevant preventive interventions. In addition, this study aimed to present our experiences with major limb amputations in Saudi Arabia.. As expected, most of amputees in this study were males with vascular diseases, followed by trauma being the leading cause of amputation. In causes related to vascular diseases, diabetes was the major culprit, while trans-tibial and trans-femoral amputations being the leading amputations related to trauma. Younger adults in the age-group of 21-30 years formed the most prevalent group when it comes to trauma-related amputations, while vascular-related amputations were highest in older adults of age 70 and above. This study also reported the improvement in FIM scores following a rehabilitation period in the SBAHC facility.
Numerous factors, including levels of technology, access to medical and surgical care, and living conditions, may account for differences in the prevalence of amputees not only between countries but also within them. This research reveals a picture of the geographic and pathological distribution of amputations across Saudi Arabia's five most populous provinces. SBAHC rehabilitation center, located in Riyadh, the capital of Saudi Arabia, is easily accessible to receive patients from all major provinces of the Kingdom. This study was carried out in order to provide a clearer picture of the physical and pathological distribution of amputations.
This study's male predominance among amputees is consistent with the findings of other researchers [26, 27] who, irrespective of race and geographical dispersion, have reached similar conclusions. This could be linked to male having more severe peripheral artery disease, higher smoking rates, and a greater propensity for road traffic accidents. On the other hand, estrogen and its influence on reducing vascular pathology may account for the lower frequency of amputations due to vascular disease [14]. The fact that diabetic patients have a 15-fold increased risk of lower limb amputation, along with the rising incidence of diabetes and vascular disease-related increases in lower limb amputation, underscores the significance of early detection, medical education, patient compliance, and reasonable glycemic control in this population. Diabetic neuropathy, which can cause loss of feeling, aberrant gait, and deformity, raises the risk of foot pathology, which raises the risk of lower limb amputation when combined with vascular abnormalities [28]. In addition, the presence of chronic foot ulcers invites infection, especially deep wound, and osteomyelitis infections that may end in amputation[29, 30]. In a study from South Africa and India, infection and ulcers were the most common causes of amputation in diabetic individuals. At the same time, ischemia was the most common cause in nondiabetic people, which was not the case in our studied cohort. This could be related to the better care provided to this cohort since medical care is free and provided by secondary and tertiary care centers [31, 32].
In the studied cohort, trauma is the second observed cause of amputation, which is similar to what has been found in developed countries, contrary to what has been found in developing countries, where trauma is the first cause of amputation [33]. These variations in amputation patterns reflect differences in comorbidities. This is the finding of the current study, which could provide a scientific reason for the increased incidence when compared with Traumatrauma. Previous research has shown that the risk of amputation increases with the number of comorbidities that a patient has. SBAHC, being a tertiary care center, receives most of its patients within five years of amputation, reflecting the efficiency of this hospital in providing services for such patients. Although trauma was ranked second in this study, it was the most common reason for amputation in young adults in their productive and active age group.
In this study, the relationship between etiology and amputation level demonstrates the significant variations between amputation and surgical decisions by medical staff. Most of our amputations were in the lower limbs, with transtibial amputation the most common, regardless of the etiology[34]. This data supports previous findings that lower limbs are wounded more frequently than upper extremities, and diabetic gangrene is more common in the lower extremities than in any other part of the body. Transfemoral amputation is more prevalent than transtibial amputation, according to the findings of other studies. This could be a reflection of the severity of the infection in the lower limb that necessitates transfemoral amputation, or it could be a surgical attitude.[35, 36]. When comparing Trauma to the degree of amputation, the transfemoral and transtibial amputation rates were nearly the same, at $9.6\%$ and $10.9\%$, respectively. That could be the effect of a wide age range in this cohort. According to research published in 1993, Trauma was the leading cause of lower limb amputation in Saudi Arabia $(52.9\%)$. The most common location of amputation was the trans-tibia, followed by the transfemoral, trans-radial, partial hand, and trans-humeral[37, 38]. Since that time, there have been no reports of amputations in this country that have been found in the PubMed database. This could be explained by the rising prevalence of comorbidities, particularly diabetes, as well as the increased enforcement of laws requiring people to wear safety belts [39]. In the population that we researched, we found that the etiology varied throughout the various age groups. According to the findings of our research, the most common age range for trauma-related amputations was between the ages of 20 and 40 years. This is consistent with a WHO report indicating that road traffic accidents are among the top causes of death in those aged 15 to 29 years old [40]. The first few months after receiving a license are extremely hazardous, and the report indicates that road traffic accidents are among the top causes of death in this age group. When taking into account the effect that age has on amputations and how it relates to the etiology of the condition, vascular disease is the most common cause of amputations. This was seen in people in their 30s and 40s, and it was the same as what other developed and developing countries found.[41].
Consequently, vascular disease-related amputation was most common in older people aged over 60 years. Furthermore, older people are more likely to have more than one ailment that may result in amputation due to vascular etiology [42]. Congenital limb deficiency, on the other hand, accounted for $79.4\%$ of lower limb deficiency in children under the age of 10 years in this study, compared to $67\%$ in the Krebs and Fishman study [43], $32\%$ in the Yigiter et al. study [44], and $73.3\%$ in the Boonstra et al. study[45]. This could be at the expense of trauma-related limb loss based on strengthening children's car safety rules. In addition to data from tertiary centers receiving patients from all over the Kingdom, these demographic parameters of children with limb deficits showed a high degree of consistency throughout the literature.
There was a significant difference between FIM scores at admission and discharge and a total FIM gain during hospitalization. On follow-up visits, we saw a considerable improvement in the total FIM score and its motor and transfer subscales. The average total FIM scores for admission and discharge were 89.811.2 and 107.51.1, respectively. A FIM score of greater than 108 indicates home independence [46]. On six-month follow-up visits, individuals in this study achieved this independence degree. This improvement was most noticeable in the self-care, transfer, and locomotion categories. The results showed an improvement in self-care, transfer, and locomotion in the FIM scores between admission and discharge, comparable with the findings of the Hall et al. study [47] and others [48, 49]. According to the findings of the study, improvements in the motor domain were significantly higher than those in the cognitive domain; however, the cognitive score was not the focus of this particular investigation. This study's strength comes from being conducted in the largest tertiary rehabilitation center in the country, which was able to represent amputees nationwide and covers all age spectrums. The second strength is that amputees in this institution are subject to a multidisciplinary approach that would give a better clinical, physical and, mental assessment, as shown in this study. Finally, although this study was limited to be a retrospective study and receiving patients after five years, that would not provide data related to immediate amputation outcomes.
In conclusion, vascular pathology caused by chronic illnesses is the key risk factor for amputation in Saudi Arabia, necessitating primary and secondary preventive efforts. A multidisciplinary approach, an in-depth understanding of the functional impacts of amputation, and a comprehensive and detailed examination of the patients and their surroundings should serve as the cornerstone for post-amputation rehabilitation programs.
### ACKNOWLEDGMENTS
The authors are grateful to the Research and Scientific Center at SBAHC for the assistance in conducting this study.
Conflicts of interest
None declared.
Generating HTML Viewer...
References
49 Cites in Article
Daniel Jupiter,Jakob Thorud,Clifford Buckley,Naohiro Shibuya (2016). The impact of foot ulceration and amputation on mortality in diabetic patients. I: From ulceration to death, a systematic review.
Caitlyn Loucas,Sarah Brand,Sima Bedoya,Anna Muriel,Lori Wiener (2017). Preparing youth with cancer for amputation: A systematic review.
Khalid Al-Rubeaan,Amira Youssef,Shazia Subhani,Najlaa Ahmad,Ahmad Al-Sharqawi,Heba Ibrahim (2013). A Web-Based Interactive Diabetes Registry for Health Care Management and Planning in Saudi Arabia.
B Green,M Anderson,J Ralston,S Catz,P Fishman,A Cook (2011). Patient ability and willingness to participate in a web-based intervention to improve hypertension control.
Kathryn Ziegler-Graham,Ellen Mackenzie,Patti Ephraim,Thomas Travison,Ron Brookmeyer (2008). Estimating the Prevalence of Limb Loss in the United States: 2005 to 2050.
Elin Børøsund,Milada Cvancarova,Mirjam Ekstedt,Shirley Moore,Cornelia Ruland (2013). How User Characteristics Affect Use Patterns in Web-Based Illness Management Support for Patients with Breast and Prostate Cancer.
Tammy Chang,Vineet Chopra,Catherine Zhang,Susan Woolford (2013). The Role of Social Media in Online Weight Management: Systematic Review.
G Pooja,L Sangeeta (2013). Prevalence and aetiology of amputation in Kolkata, India: A retrospective analysis.
Hashaam Akhtar,Sundas Khalid,Fazal Rahman,Muhammad Umar,Sabahat Ali,Maham Afridi,Faheem Hassan,Yousef Saleh Khader,Nasim Akhtar,Muhammad Khan,Aamer Ikram (2021). Presenting Characteristics, Comorbidities, and Outcomes Among Patients With COVID-19 Hospitalized in Pakistan: Retrospective Observational Study.
Sanne Klaphake,Kevin De Leur,Paul Mulder,Gwan Ho,Hans De Groot,Eelco Veen,Hence Verhagen,Lijckle Van Der Laan (2017). Mortality after major amputation in elderly patients with critical limb ischemia.
P Moxey,P Gogalniceanu,R Hinchliffe,I Loftus,K Jones,M Thompson (2011). Lower extremity amputations-a review of global variability in incidence.
Patti Ephraim,Timothy Dillingham,Mathilde Sector,Liliana Pezzin,Ellen Mackenzie (2003). Epidemiology of limb loss and congenital limb deficiency: A review of the literature.
Anton Johannesson,Gert-Uno Larsson,Nerrolyn Ramstrand,Aleksandra Turkiewicz,Ann-Britt Wiréhn,Isam Atroshi (2009). Incidence of Lower-Limb Amputation in the Diabetic and Nondiabetic General Population.
Junmei Jonasson,Weimin Ye,Pär Sparén,Jan Apelqvist,Olof Nyrén,Kerstin Brismar (2008). Risks of Nontraumatic Lower-Extremity Amputations in Patients with Type 1 Diabetes.
Naseer Ahmad,G Thomas,Paramjit Gill,Francesco Torella (2016). The prevalence of major lower limb amputation in the diabetic and non-diabetic population of England 2003–2013.
Nicholas Stone,Ajay Shah,Brian Chin,Victoria Mckinnon,Matthew Mcrae (2021). Comparing digital replantation versus revision amputation patient reported outcomes for traumatic digital amputations of the hand: A systematic review and <scp>meta‐analysis</scp>.
Zulfiqarali Abbas (2015). Reducing diabetic limb amputations in developing countries.
M Nativel,L Potier,L Alexandre,L Baillet-Blanco,E Ducasse,G Velho (2018). Lower extremity arterial disease in patients with diabetes: a contemporary narrative review.
H Al-Turaiki,L Al-Falahi (1993). Amputee population in the Kingdom of Saudi Arabia.
Hasan Alzahrani (2012). Diabetes-Related Lower Extremities Amputations in Saudi Arabia: The Magnitude of the Problem.
Fayez Alshehri,Salwa Ahmed,Sami Ullah,Haitham Ghazal,Shah Nawaz,Ahmed Alzahrani (2022). The Patterns of Acquired Upper and Lower Extremity Amputation at a Tertiary Centre in Saudi Arabia.
Alwin Robert,A,Al Dawish,M (2019). Microvascular complications among patients with diabetes: An emerging health problem in Saudi Arabia.
Abdulaziz Al Dawish,M,Alwin Robert,A Braham,R,Abdallah Al Hayek,A,Al Saeed,A,Ahmed Ahmed,R (2016). Diabetes mellitus in Saudi Arabia: a review of the recent literature.
Kari Bottemiller,Patti Bieber,Jeffrey Basford,Marcelline Harris (2006). FIM Scores, FIM Efficiency, and Discharge Disposition Following Inpatient Stroke Rehabilitation.
Hiroaki Sakurai,Toru Tsujimura,Yoshito Sugiura,Yousuke Kimura,Tetsuro Kawamura,Tetsuo Okanisi,Yoshikiyo Kanada (2011). Determinants of Return to Home After Stroke: An Analysis Based on FIM Scores.
G Carmona,P Hoffmeyer,F Herrmann,J Vaucher,O Tschopp,A Lacraz (2005). Major lower limb amputations in the elderly observed over ten years: the role of diabetes and peripheral arterial disease.
T Lim,A Finlayson,J Thorpe,K Sieunarine,B Mwipatayi,A Brady (2006). Outcomes of a contemporary amputation series.
Df (2018). The diabetic foot: Pathophysiology, evaluation, and treatment.
Laura Giurato,Marco Meloni,Valentina Izzo,Luigi Uccioli (2017). Osteomyelitis in diabetic foot: A comprehensive overview.
Chris Boodoo,Julie Perry,Paul Hunter,Dragos Duta,Samuel Newhook,General Leung,Karen Cross (2017). Views of Patients on Using mHealth to Monitor and Prevent Diabetic Foot Ulcers: Qualitative Study.
Graeme Dunbar,Derek Hellenberg,Naomi Levitt (2015). Diabetes mellitus and non-traumatic lower extremity amputations in four public sector hospitals in Cape Town, South Africa, during 2009 and 2010.
A Almohammadi,M Alnashri,Rat Harun,S Alsamiri,M Alkhatieb (2022). Pattern and type of amputation and mortality rate associated with diabetic foot in Jeddah, Saudi Arabia: A retrospective Cohort Study.
A Sarvestani,A Azam (2013). Amputation: a ten-year survey.
S Essoh,I Bamba,V Bi Dje,A Traore,Y Lambin (2007). Limb amputations in adults in an Ivorian Teaching Hospital.
A Kidmas,C Nwadiaro,G Igun (2004). Lower limb amputation in Jos, Nigeria.
V Driver,M Fabbi,L Lavery,G Gibbons (2010). The costs of diabetic foot: the economic case for the limb salvage team.
Tesfamichael Mariam,Abebaw Alemayehu,Eleni Tesfaye,Worku Mequannt,Kiber Temesgen,Fisseha Yetwale,Miteku Limenih (2017). Prevalence of Diabetic Foot Ulcer and Associated Factors among Adult Diabetic Patients Who Attend the Diabetic Follow-Up Clinic at the University of Gondar Referral Hospital, North West Ethiopia, 2016: Institutional-Based Cross-Sectional Study.
A Rahimi,M Masoumi,M Soroush,Mousavi (2009). Orthopedic complications in bilateral lower limb amputation.
Al-Wathinani Am Schwebel,D Al-Nasser,A Alrugaib,A Al-Suwaidan,H,Al-Rowais Ss (2021). The prevalence of risky driving habits in Riyadh, Saudi Arabia.
Susan Monaro,Sandra West,Janice Gullick (2017). Patient outcomes following lower leg major amputations for peripheral arterial disease: A series review.
A Abbas,A Musa (2007). Changing pattern fro extremity amputations in University of Maiduguri Teaching Hospital, Nigeria.
L Fried,L Ferrucci,J Darer,J Williamson,G Anderson (2004). Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care.
Michael Krebs,Robert Halvorsen,Irving Fishman,Norma Santos-Mendoza (1984). Prevention of Urinary Tract Infection during Intermittent Catheterization.
K Yiiĝiiter,Ö Ülger,G Şener,S Akdoğan,F Erbahçecî,K Bayar (2005). Demography and Function of Children with Limb Loss.
A Boonstra,L Rijnders,J Groothoff,W Eisma (2000). Children with congenital deficiencies or acquired amputations of the lower limbs: functional aspects.
Mts Larbi,Al Mangour,W,Saba,Al Naqeb,D Faisal,Z Omar,S (2021). Ischemic and Nonischemic Stroke in Young Adults-A Look at Risk Factors and Outcome in a Developing Country.
K Hall,M Cohen,J Wright,M Call,P Werner (1999). Characteristics of the Functional Independence Measure in traumatic spinal cord injury.
Masahiko Mukaino,Tsuyoshi Tatemoto,Nobuhiro Kumazawa,Shigeo Tanabe,Masaki Katoh,Eiichi Saitoh,Yohei Otaka (2020). An Affordable, User-friendly Telerehabilitation System Assembled Using Existing Technologies for Individuals Isolated With COVID-19: Development and Feasibility Study.
Pete Grevelding,Henry Hrdlicka,Steve Holland,Lorraine Cullen,Amanda Meyer,Catherine Connors,Darielle Cooper,Allison Greco (2022). Patient Outcomes and Lessons Learned From Treating Patients With Severe COVID-19 at a Long-term Acute Care Hospital: Single-Center Retrospective Study.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Enas M. Shahine. 2026. \u201cEtiology and Characteristics of Amputations in Saudi Arabia: A Retrospective Study from a Tertiary Rehabilitation Center\u201d. Global Journal of Medical Research - K: Interdisciplinary GJMR-K Volume 23 (GJMR Volume 23 Issue K1).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Subject: Global Journal of Medical Research - K: Interdisciplinary
Authors:
Enas M. Shahine, Mohamed T. Silarbi, Abdullah Alzeer, Mostafa Bukhamseen, Khalid Mohammed Alzaraa, Iram Saba, Sultan Bin Abdulaziz (PhD/Dr. count: 0)
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.