Necrotizing Sialometaplasia (NS) is a benign, self-limiting rare inflammatory condition that involves the salivary glands tissues and simulates a malignant process. The etiology of this lesion is still not fully understood. The aim of this study was observe and evaluate the profile of this condition and its association with smoking. This integrative review followed six methodological stages and evaluated only case reports published from 1973 to 2022. It was analyzed 134 cases which 25% of them were associated with smoking. Others clinical features were also observed and described. Although the NS is a rare condition, it is necessary to know and understand, so as not to confuse this lesion with a malignant neoplasm and apply inappropriate treatments that may impair the patient’s quality of life.
## I. INTRODUCTION
Necrotizing Sialometaplasia (NS) was first described in 1973 by Abrams, Melrose and Howell[^1]. It is characterized as a rare inflammatory process that involves the salivary glands and that in many cases represents a challenge for diagnosis, since it simulates a malignant process<sup>2,3</sup>.
In general, the lesion initially appears as a nodule that later evolves into a central ulcer and resolves spontaneously in an average period of 8 to 10 weeks $^{3-5}$. In about $75\%$ of cases, NS develops on the palate $^{5}$. The cause is commonly linked to local ischemia that generates necrosis of the salivary glands, although the etiological process has not fully understood yet $^{4,6}$.
SN is a rare lesion, cited in only $0.03\%$ of biopsies of oral lesions, although this value can be uncertain, since it is poorly recognized and often confused with other lesions[3,5]. NS occurs mostly in male patients, especially in the fourth decade of life[5]. In addition, local trauma, drug abuse and smoking are factors that may be related to the appearing of $\mathsf{SN^4}$.
In this sense, it is understood that tobacco use continues to be a public health problem worldwide, since about $23\%$ of adults in the world smoke tobacco and its derivatives[^7]. The main pharmacologically active substance in tobacco smoke is nicotine, a sympathomimetic drug. In addition, many other potentially harmful substances are released during tobacco combustion, including carbon monoxide (CO), a compound known for its ability to impede the transport of oxygen through the bloodstream.
Therefore, it is relevant to investigate and understand the etiology of NS, since this lesion is misdiagnosed both clinically and microscopically, often being confused with malignant neoplasms, generating inappropriate and aggressive treatments $^{2,5}$.
Thus, this study aimed to observe and evaluate the profile of NS over the years, gathering clinical information about this condition from cases published in the literature, emphasizing cases associated with smoking.
## II. MATERIAL AND METHODS
This integrative literature review was developed from 6 methodological stages\[^10\](figure 1) and is configured as an exploratory, retrospective review of an analytical nature.
Integrative Review
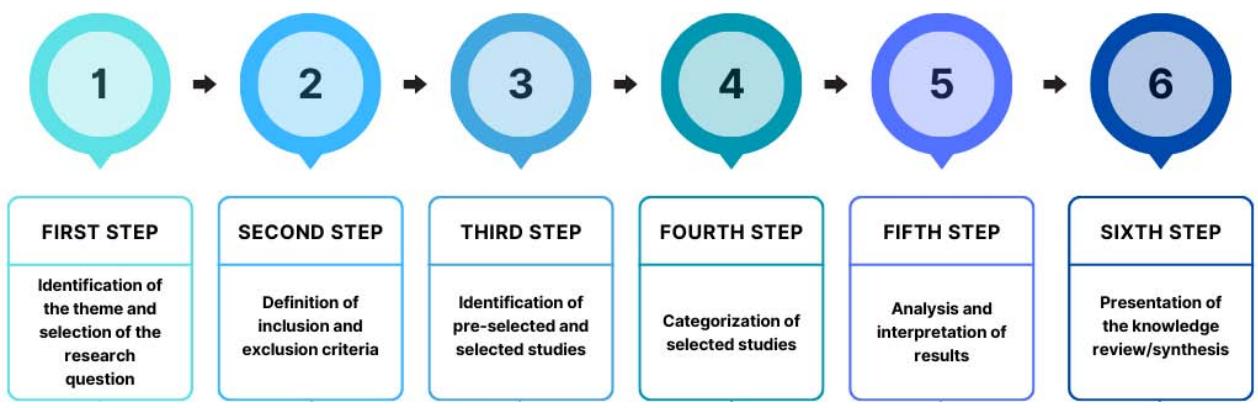 Fig. 1: Stages of the integrative review adapted from Botelho et al. (2011)
The first stage consisted of preparing the guiding question, which determined which studies would be included, the means adopted for identification and the information collected from each of the selected studies. The guiding question used was "what is the relationship between smoking and necrotizing sialometaplasia?"
The second stage consisted of a broad and diversified search in electronic databases. In this sense, the database used was from the National Library of Medicine, USA in its PubMed interface (www.pubmed.com.br), Latin American and Caribbean Literature in Health Sciences (LILACS) (lilacs.bvsalud.org), and Science Direct (sciencedirect.com), using the MeSH term "Necroziting Sialometaplasia".
The results were filtered in order to obtain only case reports published since the first time the disease was described (1973) until 2022; there were no time limits or language limits. All citations were entered into the Mendeley Reference Manager.
The third stage served to extract data from the selected articles, for which a table was built showing information about each article, namely: article title, research objective, target population and main idea of the article.
In the fourth stage, a critical analysis of the included articles was carried out, based on their complete reading. Then, data extraction was performed, which took place through an online spreadsheet, where research information, clinical characteristics and additional information were compiled as shown in table 1.
Table 1: Data extraction
<table><tr><td rowspan="3">Research information</td><td>Author</td></tr><tr><td>Publication date</td></tr><tr><td>Country where the studies were published</td></tr><tr><td rowspan="6">Clinical features</td><td>Age</td></tr><tr><td>Gender</td></tr><tr><td>Location</td></tr><tr><td>Clinical presentation</td></tr><tr><td>Evolution</td></tr><tr><td>Associated conditions</td></tr><tr><td rowspan="3">Additional information</td><td>Histological interpretation</td></tr><tr><td>Treatment and prognosis</td></tr><tr><td>Additional observations</td></tr></table>
Source:Authors
The fifth phase was developed from the discussion of the results, considering the interpretation and analysis of the articles, comparing the data evidenced in the analysis of the articles to the theoretical framework. At that moment, emphasis was placed on observing how many patients had smoking as an associated condition, in addition to identifying possible gaps in knowledge.
In the sixth and last phase, the final part of the research was developed, which is characterized by the analysis of the data and the preparation of the article, as well as the visual resources contained therein.
## III. RESULTS
From the data search carried out, following the strategy mentioned above, 352 studies were found. However, after reading the abstracts, only 80 studies[^1]
6,11-84 were selected to be read in full, since the other studies had research bias and/or were duplicated.
The included studies were published from 1973, when NS was first described, until the year 2022. During this period, the years with the highest number of published studies were 2004, 2009, 2016 and 2020. Most recurrent place of publication was the United States (21), followed by Brazil (8), Japan (6), among others (figure 2).
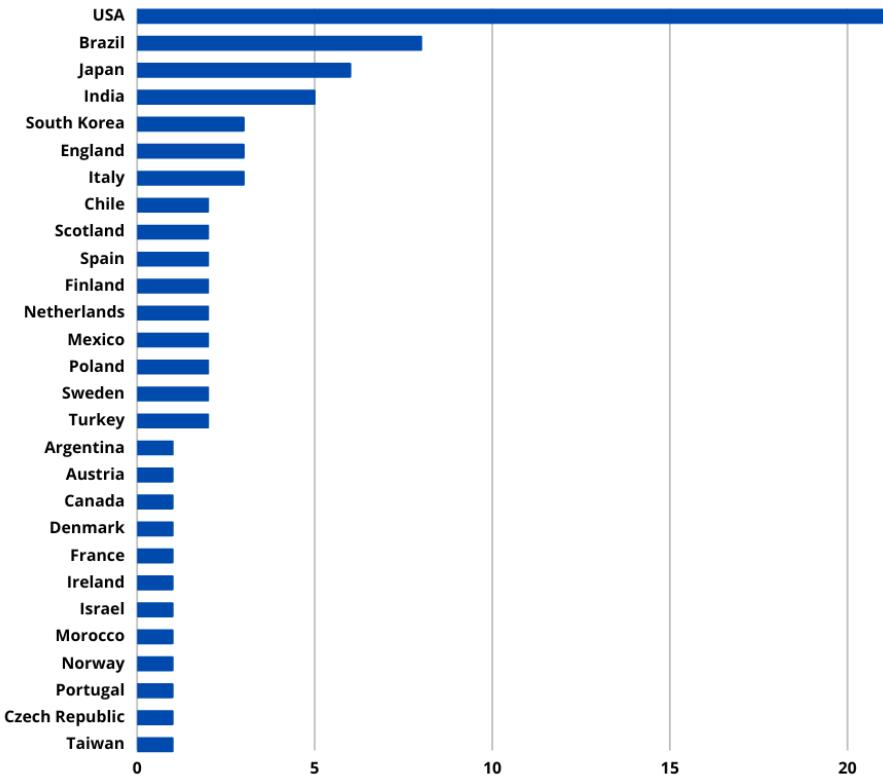 Fig. 2: Country where the studies were published
From the 80 included studies, it was possible to extract 134 cases. From this total, 78 cases $(58.2\%)$ were male patients and only 56 $(41.8\%)$ were female patients, which suggests a higher prevalence of the condition in men. Another relevant data was the general average age of the individuals, which was 43 years old, with the average age for men being 46 years old and for women being 38 years old.
Analyzing the clinical aspect of each case presented in the articles, it was possible to notice that the lesion is predominantly in the form of an ulcer (91 cases) and is also recurrent in the form of a swelling (29 cases), as illustrated in figure 3.
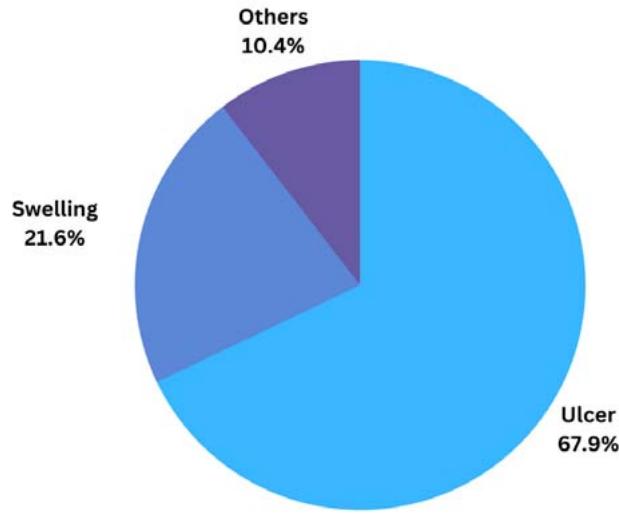 Fig. 3: Clinical presentation of the lesion in the cases studied
The most recurrent location of the lesion was on the hard palate (59% of cases), mostly unilateral, especially on the left side (figure 4A). Other regions, such as the junction of the hard and soft palate, the parotid glands, and others, were also affected by NS, as shown in figure 4B.
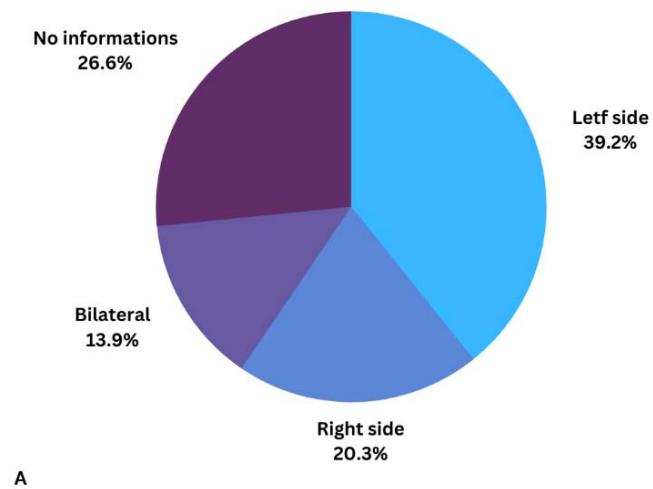
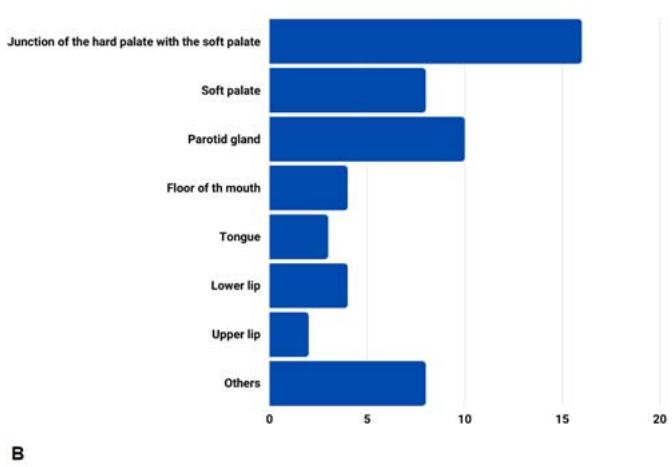 Fig. 4: A) Distribution of the occurrence of lesions on the hard palate in the cases studied; B) Other locations of the lesion in the cases studied.
The condition associated with the appearance of the most recurrent lesion, presented in the articles, was smoking (25%), isolated or associated with some other condition, mainly alcoholism (figure 5A). Furthermore, other adjacent conditions were also reported in the studies, such as oral malignant neoplasms, especially adenoid cystic carcinoma, in addition to trauma, use of prostheses and others (Figure 5B).
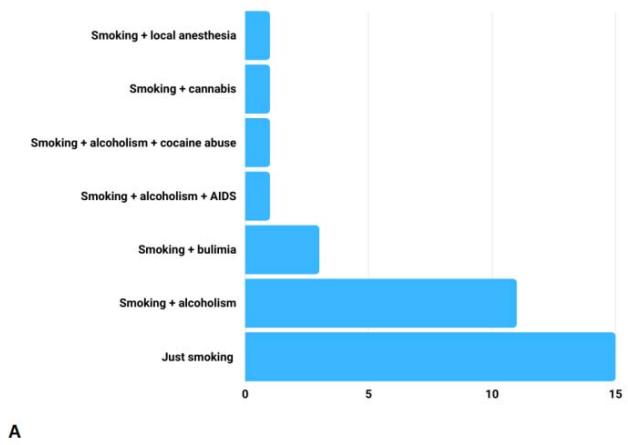
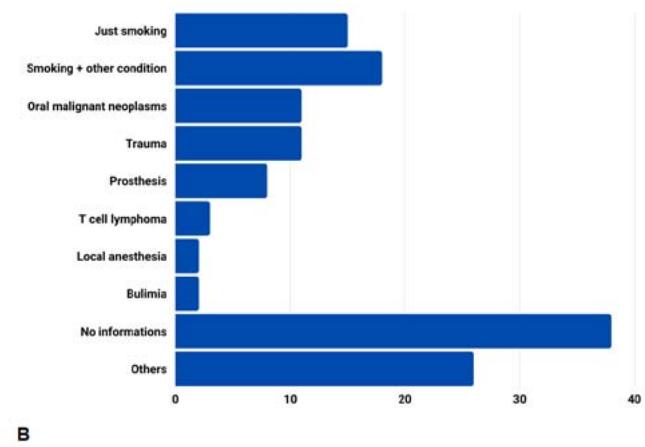 Fig. 5: A) Cases associated with smoking; B) Cases associated with other conditions.
The vast majority of cases were correctly diagnosed through biopsy. In only 10 cases there was confusion in the interpretation of the diagnosis. In 8 of them, the lesion was misdiagnosed as squamous cell carcinoma; in 1 case, as mucoepidermoid carcinoma and another one, as both. Surgical treatment was performed in 7 of the 10 inadequately diagnosed cases.
About $65\%$ of the cases own resolved spontaneously, without the need for intervention. There was surgical treatment in $21\%$ of cases and pharmacological intervention in $3\%$ of cases, as shown in figure 6.
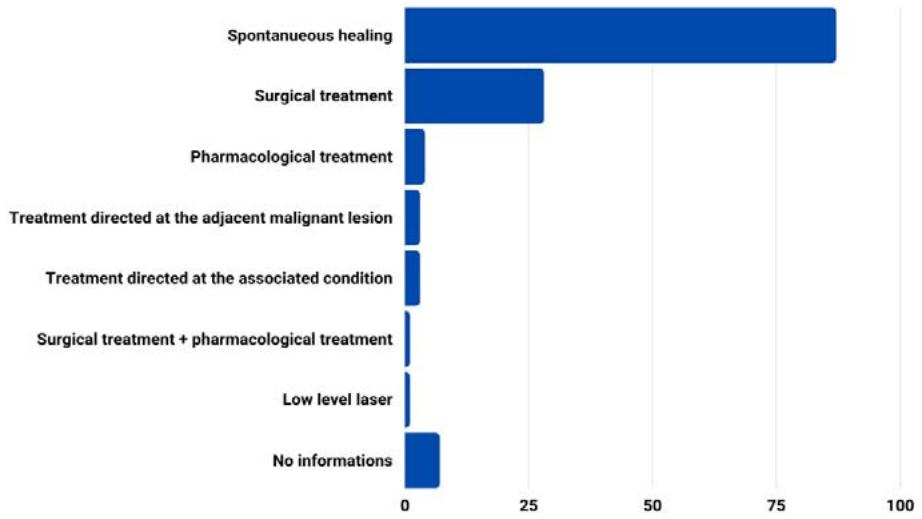 Fig. 6: Resolution of clinical cases.
Therefore, it was possible to notice that 1 out of 4 cases of NS were associated with smoking. Furthermore, of this total (33 cases), 31 cases $(94\%)$ presented as ulcerated lesions. In addition, as in the general analysis, the most recurrent location of the lesion was the hard palate $(70\%)$, but other regions such as the junction of the hard palate with the soft palate and the lower lip were also recurrent.
The average age of smokers was 43 years old, which is the same mean of the total number of patients analyzed. The patients were also mostly men (63%). Additionally, 22 cases resolved spontaneously, while 10 underwent surgical treatment and the rest were not reported. Finally, 5 cases were misdiagnosed at some point before the correct diagnosis was closed and all of them were treated surgically.
## IV. DISCUSSION
NS is an uncommon, benign, self-limiting, necrotizing inflammatory lesion that affects salivary gland tissues[^6]. It presents an etiology that is still not fully understood, although it is already accepted that the development of the lesion occurs from a local ischemia, as previously discussed. This local ischemia generates, consequently, an infarction that generates tissue necrosis, followed by repair and metaplasia[^11].
Several associated conditions are suggested as risk factors for the development of NS, including local trauma, local anesthesia, intubation trauma, chemical irritation caused by recurrent vomiting, as in cases of bulimia, in addition to tobacco use $^{12}$.
It is suggested by authors that physical, chemical or biological injuries to blood vessels are capable of producing ischemic changes, causing local infarction and the development of $\mathsf{SN}^{13}$. In this sense, the literature understands that tobacco use can cause local ischemia due to the vasoconstrictor effect of the substance[^14].
Histologically, NS is characterized by acinar necrosis at the beginning of the lesion, followed by an association of squamous metaplasia of the salivary ducts. In this context, although necrosis occurs, the lobular architecture of the affected glands is still preserved. Briefly, the histopathological criteria for diagnosing this condition are coagulative necrosis of the acini in initial lesions and squamous metaplasia and reactive fibrosis in more advanced lesions; Besides histologically benign nuclear morphology; pseudoepitheliomatous hyperplasia of the lining epithelium; mucus release; intact lobular architecture[^15].
The results of this study demonstrate a predominance of the lesion in men, as already recognized in the literature $^{16}$. In addition, the occurrence of this condition was mainly concentrated between the $4^{\text{th}}$ and $6^{\text{th}}$ decade of life. However, it was possible to observe rare cases which NS manifested itself in young patients, aged less than 20 years, the most atypical case being that of a 2-year-old child $^{17}$.
The importance of understanding this lesion is related to the fact that it is remarkably similar to a malignant process, clinically and histologically[^18]. Because of this, inadequate diagnoses can happen, leading professionals to opt for inappropriate or unnecessary treatments[^19].
NS was misdiagnosed as a malignant lesion in some cases analyzed by this study, and surgical intervention was required in almost all of them. Thus, it is possible to see how a wrong diagnosis leads to an inadequate approach capable of further impairing the quality of life of a patient who is already conditioned to NS symptoms.
NS is an injury capable of causing a lot of pain to the affected patient $^{20}$. According to the analyzed cases, the most predominant clinical presentation was in the form of an ulcer, although many cases without the presence of ulceration were also associated with pain. In addition, in many cases, the lesion started as a swelling and later evolved into an ulcer.
Furthermore, the most recurrent location of the lesion among the analyzed cases was the hard palate and, in many cases, the patient reported difficulties in eating due to the pain and sensitivity of the affected area. On the other hand, there were also reports of lesions in other regions, including those outside the oral cavity, such as the maxillary sinus[21].
Another case that draws attention is the one reported by Jeong et al. (2015) $^{22}$, which there was a recurrence of the lesion after 5 months of healing of the first lesion, something even rarer to happen and rarely reported. In the first clinical condition presented by the 36-year-old patient, a smoker, NS occurred in the form of an ulcer on the left side of the hard palate. After 5 months, when the symptoms reappeared, the lesion showed the same clinical presentation, but on the opposite side of the hard palate.
Among smokers, the most frequent region was the hard palate, as well as in cases in general. However, smokers had other regions affected by NS such as lower lip, mouth floor, parotid gland, and buccal mucosa.
The associated condition most observed among the patients in the cases studied was smoking, as already mentioned, demonstrating a possible association between this substance and the NS etiology. However, the etiology remains misunderstood and the fact that the lesion is rare, few records are made in the literature. In addition to the rarity of the lesion, there are also cases in which the lesion is confused, mainly by squamous cell carcinoma and mucoepidermoid carcinoma, which may also be a factor that hinders the dissemination of more cases in the literature.
## V. CONCLUSION
Necrotizing Sialometaplasia is an injury that, although rare, is important to be recognized in order to avoid diagnostic confusion, as well as inappropriate treatments that may harm the quality of life of the patient affected by this condition. Although the etiology is still unclear, the results of the present study demonstrated a truly relevant quantitative relationship between the occurrence of the lesion and smoking, suggesting this condition as one of the main risk factors for the appearance of Necrotizing Sialometaplasia.
Generating HTML Viewer...
References
84 Cites in Article
A Abrams,R Melrose,F Howell (1973). Necrotizing sialometaplasia. A disease simulating malignancy.
M Leite,E Freitas,S De,A De Vasconcelos Ii,T Pinheiro (2020). Low-Level Laser Therapy Approach of Bilateral Necrotizing Sialometaplasia of the Hard and Soft Palates.
Elle Nuttall,Daniel Wehrmann (2022). Bilateral Asynchronous Necrotizing Sialometaplasia of the Buccal Mucosa: A Case Report and Literature Review.
Júlia Néri,Viviane Silva,Luciana Ramalho,Laís De Castro,Jean Santos (2020). Necrotizing sialometaplasia: a case report of a non-ulcerated histopathological presentation.
Rajae El Gaouzi,Lamiae Hallab,Bouchra Taleb (2022). A diagnostic error of a necrotizing sialometaplasia: Case report.
J Hernández-Flores,E Santos-Jaimes,L Gaitán-Cepeda (2021). Necrotizing sialometaplasia of the tonsillar pillar. An unusual case.
M Perez-Warnisher,M De Miguel,Luis Seijo (2019). Tobacco Use Worldwide: Legislative Efforts to Curb Consumption.
H Porchet,N Benowitz,L Sheiner,J Copeland (1987). Apparent tolerance to the acute effect of nicotine results in part from distribution kinetics..
Alyrene Dorey,Pieter Scheerlinck,Hoanvu Nguyen,Timothy Albertson (2020). Acute and Chronic Carbon Monoxide Toxicity from Tobacco Smoking.
Louise Botelho,Cristiano Cunha,Marcelo Macedo (2011). O MÉTODO DA REVISÃO INTEGRATIVA NOS ESTUDOS ORGANIZACIONAIS.
T Tsuji,Y Nishide,H Nakano,K Kida,K Satoh (2014). Imaging findings of necrotizing sialometaplasia of the parotid gland: case report and literature review.
Alessandro Gatti,Emanuele Broccardo,Giuseppe Poglio,Arnaldo Benech (2016). Necrotizing Sialometaplasia of the Hard Palate in a Patient Treated with Topical Nonsteroidal Anti-Inflammatory Drug.
F Femopase,S Hernández,H Gendelman,M Criscuolo,López De,S Blanc (2004). Sialometaplasia necrotizante: Presentación de cinco casos clínicos.
L Kumar,A Muthukrishnan,S Gopalakrishnan (2016). Necrotising sialometaplasia at multiple sites: A therapeutic challenge to oral physicians.
A Bascones-Martínez,M Muñoz-Corcuera,R Cerero-Lapiedra,J Bascones-Ilundáin,G Esparza-Gómez (2011). Case report of necrotizing sialometaplasia.
Sowmya Krishna,Ramnarayan Bk (2011). Necrotizing sialometaplasia of palate: a case report.
L Ylikontiola,M Siponen,T Salo,G Sándor (2007). Sialometaplasia of the soft palate in a 2year-old girl.
D Farina,E Gavazzi,C Avigo,A Borghesi,R Maroldi (2008). MRI findings of necrotizing sialometaplasia.
P Keogh,E O'regan,M Toner,S Flint (2004). Necrotizing sialometaplasia: An unusual bilateral presentation associated with antecedent anaesthesia and lack of response to intralesional steroids. Case report and review of the literature.
Edgard Riquelme-M,Rodrigo Badilla-M (2018). Sialometaplasia Necrotizante: Revisión de la Literatura a Propósito de un Caso.
Hugo Dominguez-Malagon,Adalberto Mosqueda-Taylor,Ana Cano-Valdez (2009). Necrotizing sialometaplasia of the palate associated with angiocentric T-cell lymphoma.
Chan-Woo Jeong,Taegyun Youn,Hyun Kim,Kwang-Ho Park,Jong-Ki Huh (2015). Contralateral recurrence of necrotizing sialometaplasia of the hard palate after five months: a case report.
Charles Dunlap,Bruce Barker (1974). Necrotizing sialometaplasia.
Mario Arguelles,Juan Viloria,Manuel Talens,Thomas Mccrory (1976). Necrotizing sialometaplasia.
H Philipsen,J Petersen,B-H Simonsen (1976). Necrotizing sialometaplasia of the palate.
S Forney,J Foley,W Sugg,G Oatis (1977). Necrotizing sialometaplasia of the mandible.
J Hovinga,H De Jager (1977). A patient with necrotizing sialometaplasia.
James Murphy,John Giunta,Irving Meyer,Kenneth Robinson (1977). Necrotizing sialometaplasia.
R Nilsen,C Bernhoft,O Gilhuus-Moe (1978). Necrotizing sialometaplasia.
Ronald Spark,Donn Duncan (1978). Necrotizing Sialometaplasia.
Ranes Chakravorty,Tatsuo Yoneyama,Cyrus Makooi (1979). Necrotizing sialometaplasia of palate.
Robert Dunley,John Jacoway (1979). Necrotizing sialometaplasia.
Alfredo Matilla,Teresa Flores,Francisco Nogales,Hugo Galera (1979). Necrotizing sialometaplasia affecting the minor labial glands.
A Gad,Helena Willén,R Willén,S Thorstensson,L Ekman (1980). Necrotizing sialometaplasia of the lip simulating squamous cell carcinoma.
Leslie Rye,Noah Calhoun,Robert Redman (1980). Necrotizing sialometaplasia in a patient with Buerger's disease and Raynaud's phenomenon.
H Birkholz,G Minton,Y Yuen (1979). Necrotizing sialometaplasia: Review of the literature and report of nonulcerative case.
Mark Granich,Ben Pilch (1981). Necrotizing sialometaplasia in the setting of acute and chronic sinusitis.
Helena Willén,Roger Willén,Leif Ekman (1981). NECROTIZING SIALOMETAPLASIA OF THE BUCCA.
J Van Der Wal,I Van Der Waal (1990). Necrotizing sialometaplasia: report of 12 new cases.
L Aragón,A Medeiros,M Sant'ana Filho (1991). Sialometaplasia necrotizante: apresentação de caso clínico.
Louis Mandel,Ayfer Kaynar,Sharon Dechiara (1991). Necrotizing sialometaplasia in a patient with sickle-cell anemia.
Toshiharu Matsumoto,Noriyuki Kuwabara,Hidetoshi Shiotsu,Yoshiro Fukuda,Akira Yanai,Ginichiro Ichikawa (1991). Necrotizing Sialometaplasia in the Mouth Floor Secondary to Reconstructive Surgery for Tongue Carcinoma.
N Goldman,W Schroeder (1994). Necrotizing Sialometaplasia.
Doron Aframian,Isaac Milhem,Gina Kirsh,Alice Markitziu (1995). Necrotizing Sialometaplasia after Silastic Ring Vertical Gastroplasty: Case Report and Review of Literature.
G Bell,R Loukota (1996). Necrotizing sialometaplasia coincident with ipsi lateral infarcted antral polyps.
Terence Imbery,Paul Edwards (1996). NECROTIZING SIALOMETAPLASIA: LITERATURE REVIEW AND CASE REPORTS.
Harald Schöning,Rüdiger Emshoff,Alfons Kreczy (1998). Necrotizing sialometaplasia in two patients with bulimia and chronic vomiting.
Özgür Aydin,Taner Yilmaz,Feyza Özer,Sarp Saraç,Cenk Sökmensüer (2002). Necrotizing sialometaplasia of parotid gland: a possible vasculitic cause.
S Sarioğlu,U Pabuççuoğlu,C Ecevit,K Ceryan,S Paksoy,E Ada (2004). Sialometaplasia arising in the ectopic salivary gland ductal inclusions of multiple intraparotid lymph nodes.
C Scully,J Eveson (2004). Sialosis and necrotising sialometaplasia in bulimia; a case report.
Pavel Komíanek,Petr Blasch (2006). Necrotizing Sialometaplasia: A Potential Diagnostic Pitfall.
Lynn Solomon,Mihai Merzianu,Maureen Sullivan,Nestor Rigual (2007). Necrotizing sialometaplasia associated with bulimia: case report and literature review.
I Niedzielska,T Janic,J Markowski (2009). Bilateral localization of necrotizing sialometaplasia: a case report.
Dong Lee,Hye Ahn,Eun Koh,Young Rho,Hyung Chu (2009). Necrotizing Sialometaplasia Accompanied by Adenoid Cystic Carcinoma on the Soft Palate.
Alessandra Silva,Carolina Silva,Cristiane Furuse,Rodrigo Souza,Mauro Da Costa,Vera De Araújo (2010). Necrotizing sialometaplasia in a patient who is HIV positive: a case report.
Takako Yoshioka,Mizue Harada,Yoshihisa Umekita,Shuhei Taguchi,Michiyo Higashi,Daisuke Nakamura,Shinsuke Suzuki,Akihide Tanimoto (2010). Necrotizing sialometaplasia of the parotid gland associated with angiocentric T‐cell lymphoma: A case report and review of the Literature.
M Alves,D Kitakawa,Y Carvalho,L Cabral,J Almeida (2011). Necrotizing sialometaplasia as a cause of a non-ulcerated nodule in the hard palate: a case report.
T Bernardo,D Tente,P Oliveira,D Helena,D Ribeiro,S Gerós,A Silva (2012). Benign or malignant? Case report.
N Garcia,D Oliveira,S Faustino,A Azevedo (2012). Necrotizing Sialometaplasia of Palate: A Case Report.
A Suomalainen,J Törnwall,J Hagström (2012). CT findings of necrotizing sialometaplasia.
Maria Devine,Stephanie Sammut,Brendan Conn,Victor Lopes (2014). Necrotising sialometaplasia in the floor of mouth.
Tomoaki Imai,Masahiro Michizawa (2013). Necrotizing Sialometaplasia in a Patient With an Eating Disorder: Palatal Ulcer Accompanied by Dental Erosion Due to Binge-Purging.
Young-Ha Kim,Young Joo,Jeong-Hoon Oh (2013). A case of necrotizing sialometaplasia involving bilateral parotid glands.
Łukasz Gilowski,Rafał Wiench,Anna Polakiewicz-Gilowska,Katarzyna Dwornicka (2014). Necrotizing sialometaplasia of the palatal mucosa in patient with history of anorexia: Review and case report.
Nakul Uppal,Mohan Baliga (2014). Necrotizing sialometaplasia: A rare lesion that mimics oral cancer clinically and histopathologically.
O Gutiérrez,J Erazo,L Lagos,J Pozo (2017). Sialometaplasia necrotizante: reporte de un caso y revisión de la literatura.
P Haen,L Ben Slama,P Goudot,T Schouman (2017). Necrotizing sialometaplasia of the parotid gland associated with facial nerve paralysis.
Kazuhiro Yagihara,Junichi Ishii,Miki Katsurano,Eri Tsuchida,Takeshi Okamura,Ayataka Ishikawa (2018). A case of necrotizing sialometaplasia clinically mimicking a malignant tumor of the palate.
Khrystyna Zhurakivska,Eugenio Maiorano,Riccardo Nocini,Michele Mignogna,Gianfranco Favia,Giuseppe Troiano,Claudia Arena,Vito Caponio,Lorenzo Lo Muzio (2019). Necrotizing sialometaplasia can hide the presence of salivary gland tumors: A case series.
Saulo Chateaubriand,Elaine De Amorim Carvalho,Amanda Leite,Augusto Da Silva Leonel,José Prado,Danyel Da Cruz Perez (2021). Necrotizing sialometaplasia: A diagnostic challenge.
Patrícia Fernandes,Erika Pedroso,Alan Santos-Silva,Pablo Vargas,Márcio Lopes (2021). Non-ulcerated necrotizing sialometaplasia may mimic a salivary gland tumor.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Lucas Gabriel Silva Ferreira. 2026. \u201cAssociation between Necrotizing Sialometaplasia and Smoking: An Integrative Review\u201d. Global Journal of Medical Research - K: Interdisciplinary GJMR-K Volume 23 (GJMR Volume 23 Issue K2).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































