## I. INTRODUCTION
The various orthodontic anomalies can be described by means of a semiology that makes it possible to precisely define the variations from normal of the different signs. The various cases are described according to a plan that successively addresses signs affecting the teeth: dental anomalies, localized malocclusions, alveolar signs, without skeletal
Author α σ ρ ¥: Université Gamal Abdel NASSERde Conakry, Facultés des Scienceset Techniques de la Santé (FSTS), Département d'Odontologie.
Author C: Center dentaire de l'Université Gamal Abdel NASSER de Conakry.
repercussions, signs of sagittal malocclusions (Angle's classification), signs of transverse malocclusions (skeletal or alveolar), signs of skeletal anomalies in the vertical direction, their consequences on the face, dento-maxillary disharmony. Of course, these different categories can be found in the same patient, associating dental anomalies, alveolar anomalies and skeletal anomalies[1]. Numerous types of dental anomalies can be observed in the anterior sectors, and can constitute real aesthetic prejudices for our patients. The descriptive classification is the simplest, and allows us to schematically distinguish various types of anomalies, such as those of shape, structure, number, size, eruption or color. In terms of management, the
The polymorphism of these anomalies, their degree of severity, the time of consultation and the patient's age multiply the therapeutic possibilities [2]. Several studies have been carried out on these anomalies in various countries. Vishnoi et al in 2017 in the city of Udaipur, India reported $28.7\%$ definitive need for orthodontic treatment in schoolchildren aged 7 to 16 [3]. Yassir et al in 2016, in a study of a Lebanese population, found that $31.3\%$ of the sample had a strong need for orthodontic treatment [4].
The aims of this study were to determine the prevalence of orthodontic anomalies of the maxillary incisivo-canine block; to identify the orthodontic anomalies of the maxillary incisivo-canine block encountered, and to describe the type of appliance used to manage these anomalies.
## II. MATERIALS AND METHODS
The maxillofacial surgery and odontostomatology department of the Donka national hospital in Conakry was used as the setting for this study. It was a prospective descriptive study, lasting one year from August 1er2020 to August 31 2021. The study covered all patients in whom one or more orthodontic anomalies of the incisivocanine block were detected and managed during the study period.
Patients seen for one or more orthodontic anomalies of the maxillary incisivocanine block during the study period were included. Patients seen for any other dental pathologies were not included in this study.
The selection criteria were applied to 117 subjects, and patients were sampled exhaustively. The sample size obtained was as follows: $n = 20$
Data were collected manually, using an established survey form. Data entry and analysis were carried out with the help of Word and Excel software from the 2013 office pack. The results were presented in the form of tables and figures, commented and discussed according to recent data in the literature.
Informed consent was obtained from each patient or patient's relatives prior to data collection. Data were collected anonymously. The following evaluation parameters were adopted:
- An exaggerated vestibular orientation of the anterior alveolar processes and the upper or lower incisors is referred to as proalveolism.
- Dento-maxillary disharmony corresponds to a disproportion between the mesio-distal dimensions of the permanent teeth and the perimeter of the corresponding alveolar arches: the continuity of the dental arches at proximal level is no longer ensured. The most obvious sign is crowding or spacing of the dental arches (interdental diastemas).
## III. RESULTS
Table 1: Prevalence of orthodontic anomalies of the maxillary incisivocanine block.
<table><tr><td>Type of fault</td><td>Workforce</td><td>%</td></tr><tr><td>Maxillary proalveolysis</td><td>10</td><td>8,54</td></tr><tr><td>Interdental diastema</td><td>7</td><td>5,98</td></tr><tr><td>Dental crowding</td><td>3</td><td>2,56</td></tr><tr><td>Other dental pathologies</td><td>97</td><td>82,92</td></tr><tr><td>Total</td><td>117</td><td>100</td></tr></table>
Table II: Age distribution of subjects.
<table><tr><td>Age range</td><td>Workforce</td><td>%</td></tr><tr><td>9 - 14</td><td>10</td><td>50</td></tr><tr><td>15 - 20</td><td>6</td><td>30</td></tr><tr><td>21 - 26</td><td>4</td><td>20</td></tr><tr><td>Total</td><td>20</td><td>100,00</td></tr></table>
Table III: Distribution of subjects with orthodontic anomalies of the maxillary incisivocanine block by gender.
<table><tr><td>Type</td><td>Workforce</td><td>%</td></tr><tr><td>Female</td><td>10</td><td>50</td></tr><tr><td>Male</td><td>10</td><td>50</td></tr><tr><td>Total</td><td>20</td><td>100</td></tr></table>
Table IV: Distribution of subjects according to clinical signs.
<table><tr><td>Clinical and paraclinical findings</td><td>Workforce</td><td>%</td></tr><tr><td>Labial occlusion</td><td>15</td><td>75</td></tr><tr><td>Lipin occlusion</td><td>5</td><td>25</td></tr><tr><td>Dental ectopy*</td><td>5</td><td>25</td></tr><tr><td>Exaggerated maxillary overhang</td><td>9</td><td>45</td></tr><tr><td>Insufficient maxillary overhang</td><td>6</td><td>30</td></tr><tr><td>Normal maxillary overhang</td><td>5</td><td>25</td></tr><tr><td>Hemi symmetrical arches</td><td>16</td><td>80</td></tr><tr><td>A symmetrical arch hemi</td><td>4</td><td>20</td></tr><tr><td>Incisal overlap</td><td></td><td></td></tr><tr><td>2-3 mm</td><td>5</td><td>25</td></tr><tr><td>'3mm</td><td>11</td><td>55</td></tr><tr><td>'1mm</td><td>4</td><td>20</td></tr></table>
Table V: Distribution of subjects according to the type of appliance used to manage orthodontic anomalies of the maxillary incisivocanine block
<table><tr><td>Device type</td><td>Workforce</td><td>Percentage(%)</td></tr><tr><td>Hawleyplate</td><td>2</td><td>10,00</td></tr><tr><td>Fixed devices (Brackets or multi-attachment)</td><td>14</td><td>70,00</td></tr><tr><td>Orthodontic extractions+ Fixed appliances</td><td>4</td><td>20,00</td></tr><tr><td>Total</td><td>20</td><td>100</td></tr></table>
 Patient SB14- year-old patient with an anterior reverse occlusion (11,12; 22) of the maxilla prior to orthodontic treatment
 During orthodontic treatment with a Hawley plate with palatal springs and elevation of the first molars
 After orthodontic treatment Figure 1: Treatment of an anterior reverse bite.
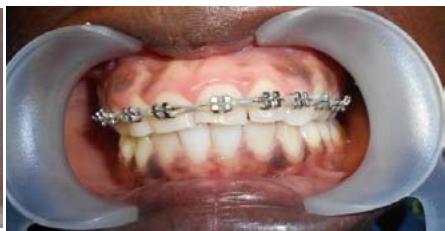
 Patient DS22 years old with anterior crowding of the maxilla prior to orthodontic treatment
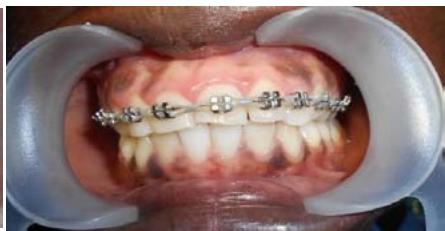 During orthodontic treatment with multi-attachment fixed appliances
 After orthodontic treatment Figure 2: Orthodontic treatment of anterior crowding.
## IV. DISCUSSION
The study revealed a prevalence of orthodontic anomalies of the maxillary incisivocanine block of $17.08\%$. This result is comparable to that of Uslu et al in Turkey in 2009, who reported a $16.1\%$ frequency of orthodontic anomalies of the maxillary incisivocanine block [5]. According to Liausas et al, adolescent age is a predictive factor for orthodontic anomalies [6]. In this series, the average age of patients was 17.60 years, with extremes of 9-26 years. These results differ from those of Liausas et al in Lithuania in 2019 and Baron et al in France in 2018, who found mean ages of 12 and 15.23 respectively [6,7]. The young age of the patients would be due to the fact that this period corresponds to that of adolescence when, very often, an awareness of self-appearance is significant.
In the present study, the gender distribution of patients was characterized by equitability of both sexes. This result differs from those of Blige et al in Turkey in 2017, who obtained a gender distribution of $44.8\%$ boys and $55.2\%$ girls [8].
The majority of patients with orthodontic anomalies in the study were schoolchildren at $65\%$. These results corroborate those of Liausas et al in Lithuania in 2019 who reported that, $42.60\%$ were schoolchildren [6]. This could explain the young average age obtained in the series.
Ectopic maxillary canines were the most common dental position anomalies, accounting for $25\%$. These results are similar to those of Nasreen et al in Pakistan in 2021, who found $30.6\%$ of subjects with ectopic maxillary canines [9].
Patients with interdental diastemas in the present series were the most represented at $75\%$. This result is contrary to that of Farid et al in a study carried out in 2012 in Morocco, who found a frequency of dental crowding/overlap of $50\%$ [10]. This predominance of interdental diastemas could be explained by the diversity of risk factors linked to the appearance of interdental diastemas. In the study, the distribution of patients according to overhang showed that maxillary overhang predominated, with a value of $45\%$. These results were superior to those obtained by Ouedraogo et al, who obtained $22.8\%$ of exaggerated maxillary overhang[11]. This predominance may be explained by the high frequency of maxillary interdental diastemas in the study.
During the study period, incisaloverlap(>3mm) was the most represented (incisaloverlap>3mm $(55\%)$ ). This result is superior to that of Faridetal, who reported $23.6\%$ of 4mm incisal overlap [10]. These results may be linked to the predominance of exaggerated maxillary overhang in this series. Maxillary proalveolism was the most frequently diagnosed condition, at $8.54\%$, followed by maxillary interdental diastema at $5.98\%$. This could be linked to heredity or to various deforming habits, notably digital suctioning, which most often act on the maxilla, depending on the technique used.
Orthodontic treatment of patients mainly involved the use of fixed appliances (Brackets or multi-attachment) followed by Hawley plates, preceded by tooth extractions, particularly in cases where temporary teeth remained.
## V. CONCLUSION
At the end of the study, a low prevalence of orthodontic anomalies of the maxillary incisivocanine block was observed. The most common subjects were schoolchildren, with both sexes equally represented. Proalveolism and maxillary interdental diastemas were the predominant manifestations of orthodontic anomalies of the incisivocanine block in the majority of subjects. Early diagnosis and appropriate therapeutic management of orthodontic anomalies of the maxillary incisivo-canine block provide better results, and their treatment is often multidisciplinary.
Generating HTML Viewer...
References
11 Cites in Article
F Bassigny (2012). Major signs and associated signs of orthodontic anomalies.
Amir Chafaie (2016). Esthetic management of anterior dental anomalies: A clinical case.
Pradeep Vishnoi,Tarulatha Shyagali,Deepak Bhayya (2017). Prevalence of Need of Orthodontic Treatment in 7–16-Year-Old School Children in Udaipur City, India.
T Yassir,B Joseph,H Nuha,Ames Ahmed (2016). Association between normative need for orthodontic treatment and autopercu need in a¸ Lebanese population.
Ozge Uslu,M Akcam,Sehrazat Evirgen,Ilker Cebeci (2009). Prevalence of dental anomalies in various malocclusions.
Hatice Olkun,Gulsilay Sayar (2019). Impact of Orthodontic Treatment Complexity on Oral Health-Related Quality of Life in Turkish Patients: A Prospective Clinical Study.
C Baron,M Houchmand-Cuny,B Enkel,S Lopez-Cazaux (2018). Prevalence of dental anomalies in French orthodontic patients: A retrospective study.
N Bilge,S Yeşiltepe,K Törenek Ağırman,F Çağlayan,O Bilge (2018). Investigation of prevalence of dental anomalies by using digital panoramic radiographs.
N Nasreeni,A Imtiaz,R Sadia,P Hana,K Taskeen,A Tahira (2021). Frequency and association of maxillary ectopic canine with incisor root resorption and dental agenesis.
B Farid,S Mourad,H Mouna,Laila Zouhair,A Farid,E (2012). Prevalence of malocclusions and orthodontic treatment need in 8-to 12-year-old schoolchildren in Casablanca, Morocco.
Y Ouédraogo,Y Lamien,A Sawadogo,Cnt Ouédraogo,K Touré,A Sangaré (2020). Prevalence of dental malocclusions and need for orthodontic treatment among students inthe city of Boromo.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
FADIGA Mohamed Sid-dick. 2026. \u201cPrevalence and Treatment of Maxillary Incisivo-Canine Block Anomalies at the Donka National Hospital in Conakry\u201d. Global Journal of Medical Research - J: Dentistry & Otolaryngology GJMR-J Volume 23 (GJMR Volume 23 Issue J3).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.