Physician Leader as a Change or Burnout Agent in Physician Group Practices: Leadership Approach from a Mindfulness, Selflessness, and Compassion (MSC) Outlook
## I. INTRODUCTION
The evolution of physicians' role as independent caregivers and leaders in effective teams, has reshaped the opportunity pathways for those seeking new platforms to exert leadership influences and professional satisfaction in healthcare settings that experience unparalleled changes (Shanafelt et al., 2017; Wolper, 2013). However, the notion of engagement is crucial to leadership development for physicians seeking mobility within organizations with high-stress levels or planning to join group practices because of one key factor expressed as burnout (Romani & Ashkar, 2014; Verweij et al., 2016). Burnout, defined by Verweij et al. (2016) is a "syndrome of emotional exhaustion, depersonalization, and a diminished sense of personal accomplishment (p. e99). Shanafelt et al. (2017) equate burnout to cynicism and diminished effectiveness. Hougaard and Carter (2018) added that seeking a leadership position requires selflessness and courage with constant introspection of behavior, strategies to excel, and leading people by engaging them to succeed. For Hougaard and Carter (2018) it requires an ego-free mentality, humility, "a realistic perspective on individual worth, a sense of self and a healthy self-confidence" (pp.72-73).
It is noteworthy to consider a physician leader as a change agent when there are key principles of new roles learning, new skills development, and acquisition that the physician has not acquired during medical training that can yield to a position of power and are critical to the success of institutional and group practices (Wolper, 2013). Wasylkiw et al. (2015, as cited in Jamieson, 2021) defined, in this context, leadership as a relational process relying on trust, empathy, and inspiring others. Physicians must become learners of change in organizations to survive and grasp the tenets of a VUCA environment [volatile, uncertain, complex, and ambiguous](Kinsinger & Walch, 2012). Hougaard and Carter (2018) see a sensible dimension of leadership prioritizing human values, meaning, and connection for optimal change within organizations. Do the expressed considerations suggest that it is not asinine to ask what are the driving factors causing physician leadership challenges and burnout in group practices?
To better answer this question, it is reasonable to dig into the literature search about physicians as change and burnout agents in group practice settings, lifestyle interventions, and burnout strategies. Additionally, this article presents an MSC outlook to balance the root causes of physician burnout and highlight the changing dynamics of efficient leadership. A short critique of the proposed solution will follow.
## II. LITERATURE REVIEW
### a) Physician as a Change Agent in Group Practices
Medical group practices in the United States started in the early 1930s when the American Medical Association recognized approximately three hundred medical practice groups that evolved to become the dispensary, academic medical center, industrial medical program, and private clinic (Wolper, 2013, p, 12). The noticeable rapid growth paved the way for the creation of the Medical Group Management Association (MGMA), which morphed into the health maintenance organization (HMO), accountable care organizations (ACO), and employers' preferred provider organizations (PPOs). With the passage of the Patient Protection and
Accountable Care Act (PPACA) of 2010, the healthcare organizations grew to create the integrated health delivery systems (IDS), multispecialty group practices (MSGPS), physician-hospital organizations (PHOs), independent practice associations (IPAs), and the virtual physician organizations (VPOs) (Wolper, 2013).
Within this healthcare network, physician leadership in medical group practices grew until hospitals started to acquire physician groups in different markets to properly align hospitals with physician group practices. The rationale was due to the concept of managed care under former President Clinton's quality healthcare reform allowing hospitals and physicians to assume risks, increase bed placements with admissions, and capitalize on revenue streams, but the cost was exaggerated (IMO, 2001, as cited in Wolper, 1013).
The physician is a change agent because of his or her ability to survive internal and external challenges, meet strategic priorities, recruit, and retain quality physicians for the group practice. Nonetheless, because of the competition, it is a challenge to retain them. Kotter (1996, 1990, as cited in Wolper, 2013) explained that allowing physicians to depart from their traditional roles required comprehensive management skills to control large organizational structures and changes in the group practice. Physicians who planned the best approaches to implement and lead changes grasped important challenges and excelled. Wolper (2013, pp. 90-93) articulated the following internal leadership challenges that the physician, as a change agent should tackle:
- Price control efficiency to reduce rising costs and boost revenues.
- Planned direction to meet current setting with clear strategic goals.
- Honesty and effectiveness are due to the physician's apparent trustworthiness and clinical success.
- Exhibit appropriate behavior as an essential leadership trait to utilize physicians as colleagues of the clinical teams.
Cochran et al. (2014) looking at physician leadership postulated that physicians must be accountable for changes occurring in the healthcare systems, as well as in their private or group practices. To this end, they must acquire the necessary skills to manage larger or group practices and avoid isolation. Cochran et al. (2014) referred to an "expanded paradigm of physician leadership" (p.19). The development of physicians as change agents in group practices also presupposes the ability to generate a vision and enthusse physicians to change because of engagement, and a clear comprehension of why issues must change, Cochran et al. (2014) contended.
Furthermore, since hospitals constantly buy physician group practices, they create an employer-employee framework, with the physician as an employee, and a way to prepare for revision in payment reforms holding the provider accountable for services. According to Cochran et al. (2014), there is an enormous need for physician leadership and engagement in hospital systems, and hospitals reason how to create better physician leaders. By doing so, the emphasis is to foster a group of physicians as change leaders, not solely employees. Cocharan et al. (2014) further expressed the industry's opinion about leadership development as a key component of health systems performance but reported that integrated group practices should prioritize leadership before contemplating a merger agreement. Hospitals are not willing to absorb the cost of leadership development.
### b) Physician as Burnout Agent in Group Practices
One of the ideas behind the creation of physician group practices to minimize stress endured in hospital settings was to foster sustainability in healthcare through efficient allocation of services with an evidenced-based approach valuing patients at the center of the system (Harris et al., 2017; Wolper, 2013). Today, the currents of changes push physicians in group practices and in hospital settings to share greater accountability. These changes became real stressors to physicians dealing with demanding stakeholders: purchasers, policymakers, and patients holding them accountable more than ever before (Cochran et al., 2014). A physician is expected to assume a great leadership role in patient care. There are also constraints in the payment systems: providing market-competitive compensations to physicians within the group, from insurers and hospitals acquiring physician practices, which engender tremendous stress, anxiety, and distress leading to burnout (Cochran et al., 2014; Wolpert, 2013). The American Medical Association (Berg, 2021) reported that physician burnout impacts all specialties and practice locations, and drivers are feeding this trend. The American Medical Association reported that in a 2020 Medscape online survey with more than 20,000 physicians who responded from 20 specialties, the overall physician burnout rate was down to $42\%$ compared to five years from $46\%$ (Berg, 2021). "The highest percentage of physician burnout occurred across these specialties (p.1)"
Urology: $54\%$
Neurology $50\%$
Nephrology $49\%$
Diabetes and endocrinology: $46\%$
Family medicine: $46\%$
Radiology: $46\%$
To date, the best research found was a controlled mixed-methods pilot study by Verweij et al.
(2016) about a mindfulness-based stress reduction (MBSR) for 50 general practitioners with longstanding experience in primary care and private practice at two Dutch hospitals. Using the quantitative realm, the research revealed that during pre-post ratings, the between-group differences at baseline, the MBSR group reported significantly more depersonalization and less work engagement. At the end of the training, controlled for baseline scores, the MBSR group experienced a decrease in depersonalization than the control group (p.101). The trainers consisted of a general practitioner (GP) with private medical practice, a consultant psychiatrist, a psychotherapist, and a psychologist. Looking at the same mindfulness parameters, Hofert et al. (2020) conducted a pilot study at a community hospital that provided mindfulness-based stress reduction (MBSR) to determine if MBSR leads to burnout reduction and improved patient care as identified by clinicians. The findings indicated that MBSR decreased burnout and apparent stress. Romani & Ashkar (2014) stated that the burnout rate is more pronounced among practicing physicians.
### c) Maslach Burnout Inventory (MBI)
The Maslach Burnout Inventory consists of a 22-item questionnaire considered the standard document to assess burnout (Tawfik et al., 2018, p.3). Physicians with a high score of depersonalization (DP) or emotional exhaustion (EE) subscale of the MBI had at least one indication of professional burnout. Consistent with the cross-sectional study of 6,695 currently practicing responding physicians in the U.S., Tawfik et al. (2018) pursued to describe burnout, fatigue and depressive symptoms, patient safety, and physician wellbeing, to medical errors (p.2). The study conclusion was physician burnout, fatigue, and work safety measures were independently associated with medical errors and unit safety. Burnout and poor well-being were determined as having negative effects on healthcare professionals and patients.
### d) Lifestyle Interventions for General Practice Physicians
While the literature on burnout in physician practice is scant, one can argue that physicians exhibiting this syndrome from work-related stress: emotional exhaustion, depersonalization, withdrawal, and feelings of ineffectiveness (WHO, 2019, as cited in Wolper, 2013) may put their patients at risk and expose them to inadequate wellbeing or support (Hofmeyer et al., 2020). Derman et al. (2008) reported, in a study generated from a 2003 world survey in South Africa, that a healthy lifestyle intervention or modification is required from general practice physicians for their patients. Taking into consideration the burnout notion of physicians' poor wellbeing, such an approach would not be attainable in the U.S.
### e) Mindfulness- Selflessness-Compassion (MSC)
As proposed by Hougaard and Carter (2018), the MSC framework emphasized the need for healthcare leaders to embrace mindfulness, selflessness, and compassion, as essential practices to enhance their organization's mission and values in a changing world. The framework is captured in figure 1.0 below from Hougaard and Carter's (2018) book: The mind of the leader: How to lead yourself, your people, and your organization for extraordinary results. What is paramount is a leader's ability to embrace leadership skills needed to focus on awareness, about what he or she, and the organization are doing, and where they are going. The benefits of mindfulness, selflessness, and compassion can be assessed within an organizational context, Hougaard and Carter (2018) posited. The mindfulness leadership model consists of three essential qualities:
1) The mindfulness leader exhibits a focused quality, which is the ability to concentrate on a particular task with deliberate ease. A focused strategy leads to awareness.
2) The selflessness leader finds ways to get out of his or her comfort zone to reach and empower people. Selflessness promotes humility, and self-confidence by keeping the ego at bay to see others doing their best.
3) The compassionate leader embraces compassion defined as holding positive intentions towards others, being of service to them, and being able to understand their perspective. It encourages strength and courage and fosters good decision-making for the good of the organization (Hougaard & Carter, 2018).
These enunciated pillars (Hougaard & Carter, 2018, pp.12-19) rely on three matrices:
- (a) A mindfulness matrix showing focus versus distraction. In the first spectrum, the leader is focused and aware, able to bypass distraction since there is a task to accomplish. Mindfulness implies awareness.
- (b) In the selflessness matrix, the selflessness leader exhibits a selfless attitude with confidence. In the lower spectrum, lacking such confidence leads to egoism and strong narcissist traits.
- (c) In the compassion spectrum the combination of compassion with wisdom creates a benevolent attitude. A lack of wisdom and compassion leads to ignorance and indifference. The leader exhibits incompetence.
Putting together, the model proposed by Hougaard and Carter (2018) and Conversano et al.'s (2020) arguments against burnout and compassion fatigue, which associate compassion fatigue with burnout are paramount and needed. One can argue that attentional ability, defined as focus sustained attention: a key indicator encompassing awareness in mindfulness, which is paying attention to the present moment, is a prerequisite. The practice of mindfulness and MSC supports the mindfulness and compassion-related qualities that physicians need to exert after embracing mindfulness. It is advanced that compassion-based interventions lead to improvement in
self-compassion for self may lead to compassion towards others. One can further add that it clarifies both the compassion and selflessness matrices presented by Hougaard and Carter (2018). Using the MSC strategy with mindfulness-based stress reduction (MBSR) training is a viable option when dealing with physician burnout in group practices.
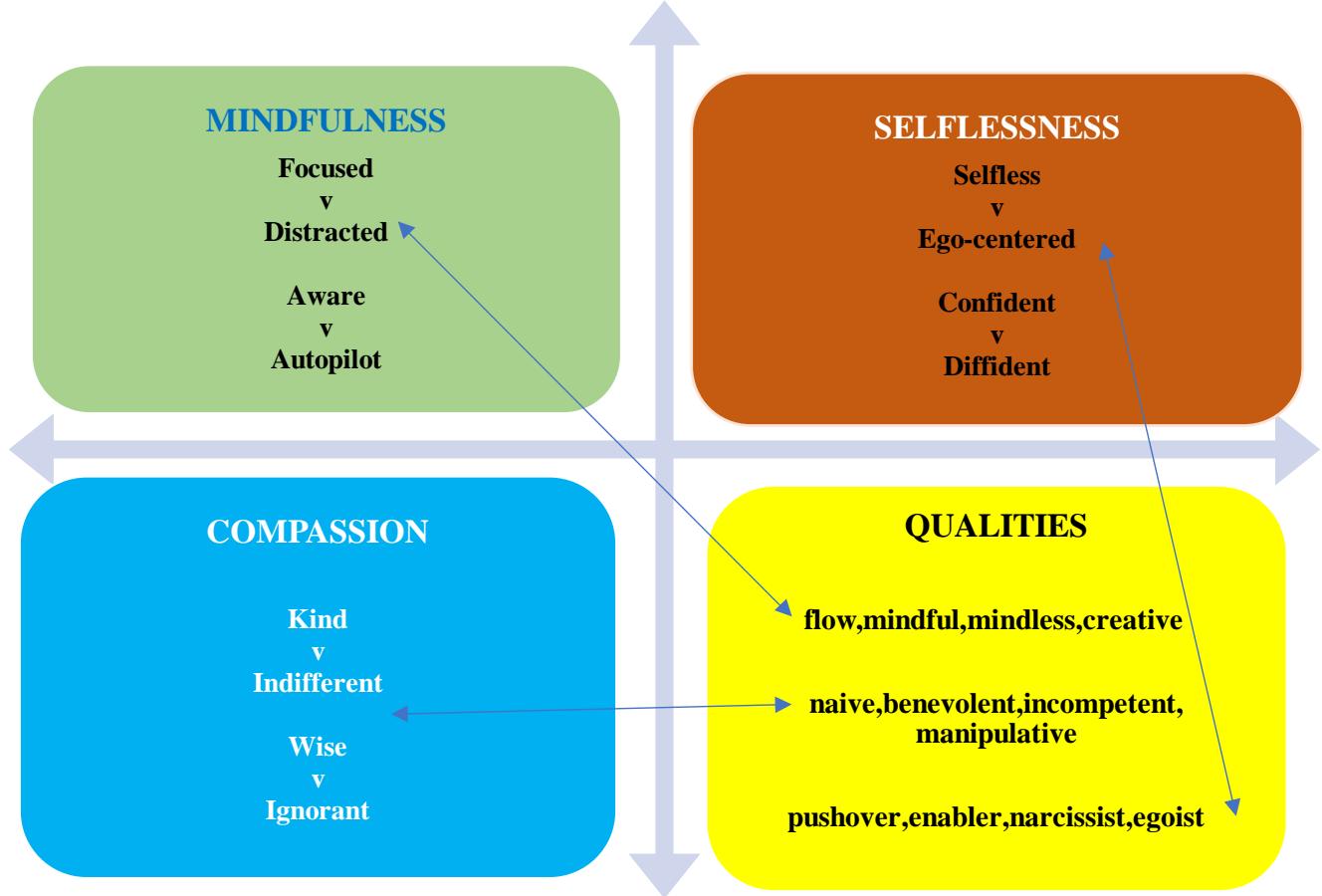
Figure 1.0: MSC Leadership (Based on Hougaard & Carter, 2018)
f) The Jamieson's Review and other Interventions Looking at the Physician as a Change or Burnout Agent
There are several considerations and interventions explored within a context that promotes individual and organizational health. Jamieson (2021) brilliantly looked at the domains of "self" and "others" using quantitative and qualitative studies. The domain of self entails the leader's mindful approach to self-care, self-awareness, and emotional regulation in conjunction with decision-making (p.44). The assertion that a leader's expression of competence, a self-construct only makes sense when it reaches others within an organization by generating positive influences, and broader organizational development, is powerful. Rupprecht et al. (2019) embraced the "self" concept as a leader's improvements in self-leadership, self-care, and self-reflection toward effective management. It seems to correlate with the principles of selflessness which can be practiced by making others better participants in an organizational setting. Hougaard and Carter (2018) explained this process as influencing organizational culture. In that culture, it is important to connect one's advocated values to agency experiences (Hougaard & Carter, 2018). Putting this into the proper context of burnout, a physician has the option to approach self-care about others if he/she realizes that it can impact others in a wider organizational context (healthcare institutions, group practices, etc.). The caveat is the physician's ability to recognize the need for help and adopt a care-seeking attitude, I contend. Shanafelt et al. (2017) used the strategy of harnessing the power of leadership for organizational success and its impact on professional satisfaction. The necessary construct, in this case, is a compassionate organization where each person is valued, and takes an active part in organizational success, Hougaard and Carter (2018) explained.
Dealing with the problem of physician burnout, Patel et al. (2019) presented strategies adopted by
Mayo clinic to manage physician burnout in hospital settings. They consist of managing physician burnout through measuring well-being by assessing the regulatory tentacles serving as a burden on them, annual measures comparing their data against the national database, enabling them to assess workloads and satisfaction levels per departments originating the burnout.
### g) Benefits and Disadvantages of the MSC Strategy
Physician group practices can rely on an MSC strategy to foster mindfulness interest, as a transparent option focusing on the present moment. From an organizational standpoint, it requires time, and the recruitment of qualified individuals to foster a culture of positive change. MSC, utilized as a new leadership practice, can be a positive tool in a VUCA (volatile, uncertain, complex, ambiguous) business environment. It is not the only remedy, but a much-needed one. However, it is not clear how physician group practices will embrace the MSC strategy since it has been applied in larger organizations (Hougaard & Carter, 2018). There are other areas such as quality assessment for the effectiveness of the group practice responding to the changes in payment systems that are problematic to implement, which can slow the implementation of an MSC framework. What are the costs involved in MSC and MBSR training? Is it affordable? can MSC help grow small group practices? and what are the implications?
### h) Alignment of Group Practice's Vision and Mission With MSC
There is a real concern that bringing an MSC leadership style to organizations can be a threat to the corporate work ethos. In a dog-eat-dog corporate world, is there a plausible way, how can this be possible? What is key is the idea that physician leaders or executives need to develop the MSC (mindfulness, selflessness, and compassion) qualities after being exposed and trained. There is a constant need to develop new paradigms. Kuhn (1971) enunciated that out of a crisis, new paradigms emerge. Since MSC leadership rightfully questions a failed conventional leadership paradigm neglecting the relational aspects of organizations' goals, and societal responsibilities, physician leaders with the potential to change themselves can transform their organizations by focusing on the well-being of the people at the workplace. Similarly, a mindfulness training framework and adherence to a compassionate leadership style may generate immense benefits.
### i) Ethical Concerns
The concept of McMindfulness best exemplifies the ethical question. The McMindfulness approach implies a lack of groundwork for mindfulness-selflessness-and-compassion to flourish. It is associated with the McDonaldization notion that mindfulness departs from its original Buddhist tradition and has been marketed or capitalized as a MacDonald (Hyland, 2017). McDonaldization lacks educational and transformative values and is concerned about the bottom line or profit maximization. The idea is that a McDonald is a McDonald everywhere, meaning mindfulness interventions are the same everywhere from a marketing and financial standpoint. McMindfulness can be associated with unethical interpersonal leadership behavior (Reb et al., 2019) posited. McMindfulness offers a decontextualized setting for mindfulness in small and larger venues. It is prudent to ensure that adhering to MSC is not simply a practice lacking ethical concerns from leaders' interpersonal communication.
## III. CONCLUSION
This article taps into a broad field of organizational leadership using individual mindfulness towards a collective application to deal with physician burnout. The literature covers the span of burnout from internal and external threats to physicians in hospitals, such as excessive demands to provide quality care to patients, insurmountable paperwork, and not well-defined goals by management. A physician's scope of practice in this volatile, uncertain, complex, and ambiguous environment (VUCA) is changing. Physicians' group practices are not exempt. Stress reduction is a prominent issue to consider within the VUCA environment. Leaders embracing the concept of mindfulness-selflessness-compassionate (MSC) leadership can add mindfulness stress reduction (MBSR) experiences to highlight the benefits of applying individual mindfulness in a collective sphere. However, it is not enough. Physicians in group practices may have a greater latitude to implement the MSC leadership vision from the individual to the organization to strive for efficient successes, reach higher heights in providing care to their patients, and even change their practices' mission, vision, and value statements. There is a wide-open door for them to enter. Further research is needed.
Generating HTML Viewer...
References
19 Cites in Article
Atul Grover,Michael Dill (2021). New Workforce Model Suggests Continued Physician Shortages in Nonprimary Care Specialties.
Jack Cochran,Gary Kaplan,Robert Nesse (2014). Physician leadership in changing times.
Ciro Conversano,Rebecca Ciacchini,Graziella Orrù,Mariagrazia Di Giuseppe,Angelo Gemignani,Andrea Poli (2020). Mindfulness, Compassion, and Self-Compassion Among Health Care Professionals: What's New? A Systematic Review.
E Derman,D Patel,C Nossel,M Schwellnus (2008). Healthy lifestyle interventions in general practice.
Claire Harris,Kelly Allen,Richard King,Wayne Ramsey,Cate Kelly,Malar Thiagarajan (2017). Sustainability in Health care by Allocating Resources Effectively (SHARE) 2: identifying opportunities for disinvestment in a local healthcare setting.
Sheila Hofert,Sean Tackett,Neda Gould,Erica Sibinga (2020). Mindfulness instruction for community-hospital physicians for burnout and patient care: A pilot study.
Anne Hofmeyer,Ruth Taylor,Kate Kennedy (2020). Fostering compassion and reducing burnout: How can health system leaders respond in the Covid-19 pandemic and beyond?.
R Hougaard,J Carter (2018). The mind of the leader: How to lead yourself, your people, and your organization for extraordinary results.
Terry Hyland (2017). McDonaldizing Spirituality.
K Jamieson (2021). Exploring healthcare leaders' descriptions of implementing mindfulness in the workplace during the COVID-19 pandemic.
T Kuhn (1971). The structure of scientific revolution.
Rikinkumar Patel,Shiana Sekhri,Narmada Bhimanadham,Sundus Imran,Sadaf Hossain (2019). A Review on Strategies to Manage Physician Burnout.
Jochen Reb,Sankalp Chaturvedi,Jayanth Narayanan,Ravi Kudesia (2019). Leader Mindfulness and Employee Performance: A Sequential Mediation Model of LMX Quality, Interpersonal Justice, and Employee Stress.
Maya Romani,Khalil Ashkar (2014). Burnout among physicians.
Silke Rupprecht,Pia Falke,Niko Kohls,Chris Tamdjidi,Marc Wittmann,Wendy Kersemaekers (1081). Mindful Leader Development: How Leaders Experience the Effects of Mindfulness Training on Leader Capabilities.
Tait Shanafelt,John Noseworthy (2017). Executive Leadership and Physician Well-being.
Daniel Tawfik,Jochen Profit,Timothy Morgenthaler,Daniel Satele,Christine Sinsky,Liselotte Dyrbye,Michael Tutty,Colin West,Tait Shanafelt (2018). Physician Burnout, Well-being, and Work Unit Safety Grades in Relationship to Reported Medical Errors.
Hanne Verweij,Ruth Waumans,Danique Smeijers,Peter Lucassen,A Donders,Henriëtte Van Der Horst,Anne Speckens (2016). Mindfulness-based stress reduction for GPs: results of a controlled mixed methods pilot study in Dutch primary care.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Clarence St.Hilaire. 2026. \u201cPhysician Leader as a Change or Burnout Agent in Physician Group Practices: Leadership Approach from a Mindfulness, Selflessness, and Compassion (MSC) Outlook\u201d. Global Journal of Human-Social Science - H: Interdisciplinary GJHSS-H Volume 22 (GJHSS Volume 22 Issue H6).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Physician Leader as a Change or Burnout Agent in Physician Group Practices: Leadership Approach from a Mindfulness, Selflessness, and Compassion (MSC) Outlook



































































