Situs inversus totalis is a rare congenital malformation that results in mirror positioning of the thoracic and abdominal organs. Situs inversus abdominalis is a right-left inversion limited to the abdomen; The association of situs inversus with intestinal band occlusion is infrequent; We report a case of acute intestinal obstruction associated with situs inversus abdominalis, the diagnosis was confirmed by abdominopelvic CT scan, and the treatment consisted of a gallbladder resection with anastomosis, with good postoperative results.
## I. INTRODUCTION
Situs inversus totalis is a rare autosomal recessive condition (1) (1 in 8,500) (2-3) that results in mirror positioning of the thoracic and abdominal organs.; Situs inversus abdominalis, also known as situs inversus with levocardia or left-sided heart, is a condition with right-left inversion limited to the abdomen (4-5). SIA is a recognized cause of obstruction in the pediatric population due to intestinal abuse; Despite, this reason of acute surgical emergencies in adults is extremely rare; this case describes a small bowel obstruction in an adult patient with SIA (2).
## II. CASE PRESENTATION
The patient was 67 years old, with no previous pathological history, and was admitted to the surgical emergency room for an occlusive syndrome of vomiting, generalized abdominal pain, and cessation of food and gas that had been evolving for three days; Clinical examination revealed a conscious patient with tachycardia at 120 bpm, BP: 100/60 mmHg, the temperature of 37.3, distended abdomen and tympanic with generalized abdominal tenderness; on rectal examination, the rectal ampulla was empty without palpable mass. Abdominal radiography showed gregarular hydroaeric hydroaerobic. Abdominopelvic CT showed a bowel obstruction upstream of an area of hypogastric caliber disparity, with A complete abdominal situs inversus with the liver, and portal trunk visible on the left, spleen and stomach visible on the right and heart in place.
 Fig. 1: Situs Inversus Abdominalis: Stomach on the Right, Liver and Gallbladder on the Left
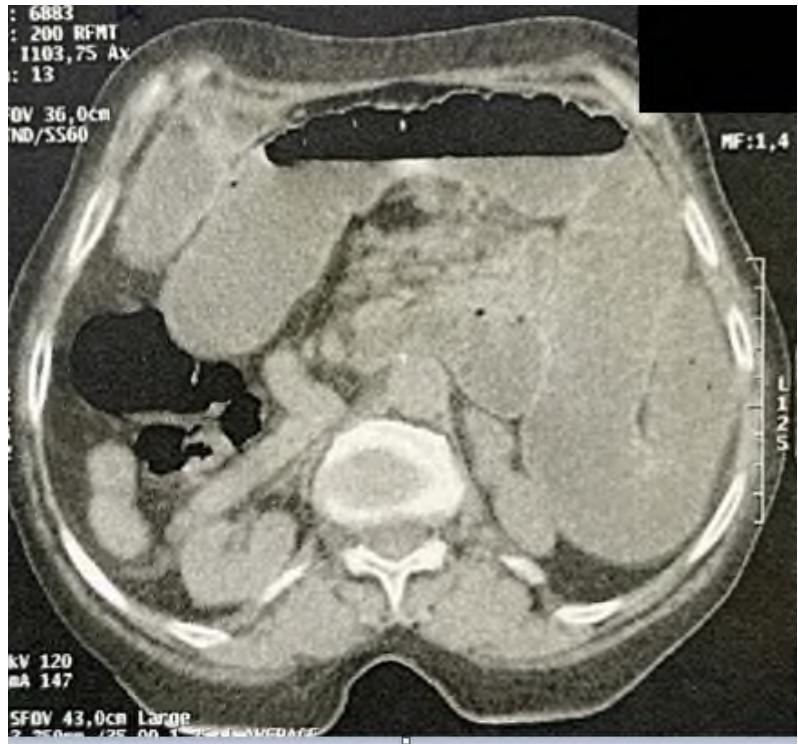 Fig. 2: Small Bowel Obstruction and Situs Inversus Abdominalis
The patient was operated on in the emergency room after resuscitation measures. The surgical exploration found a 4 cm dilatation of the bowel upstream of a gremo-mesenteric flange at $1.80\mathrm{m}$ from the duodenojejunal angle and 50 cm from the ileocaecal junction with necrosis of 1 m of the small bowel and the presence of a complete abdominal situs inversus and common mesentery. The procedure consisted of segmental resection of $1\mathrm{m}$ of the small intestine with necrosis of the small intestine and a small intestine anastomosis. The postoperative course was simple. The patient was discharged from the hospital on the fifth day and recovered four months later.
 Fig. 3: Intraoperative Images Showing Bowel Necrosis
 Fig. 4: Intraoperative Images Showing the Stomach on the Right, the Liver and Gallbladder on the Left Confirming the Situs Inversus Abdominalis
## III. DISCUSSION
SIT is a rare congenital malformation (1-6), first reported by Fabricius in 1600 (7), characterized by an inverted position of all viscera, including dextrocardia; the normal lung anatomy is inverted; The liver and gallbladder are located on the left side, and the spleen and stomach are on the right side (5).
The etiology of situs inversus has not been fully elucidated; studies have shown that it is related to genetic factors, changes in chromosome structure and number (8-6-9), maternal diabetes, and exposure to retinoic acid (10). In our patient no associated congenital anomalies were identified.
Some authors have reported that $60\%$ of patients with situs inverus have other congenital anomalies of the gastrointestinal tract, such as gallbladder or intestinal atresia, splenic agenesis or colonic duplication. These anomalies manifest themselves in childhood, which leads to early diagnosis, if not prenatal diagnosis (8-3-10-5). Congenital heart defects are present in about $5 - 10\%$ of patients (3).
Situs inverus can be asymptomatic and diagnosed incidentally during laparotomy or autopsy (5), and its revelation by occlusive syndrome would be a rare event (5-8), and its revelation by an occlusive syndrome would be a rare event (8). This is the case of our patient; she was asymptomatic and did not know that she was carrying a situs inversus abdominalis (8), and it was the abdominal CT scan requested to support the diagnosis of intestinal obstruction, which allowed the discovery of the diagnosis of SIA by showing a reversal of the position of the abdominal viscera (8). This paraclinical examination is the critical examination to confirm the diagnosis of this anomaly.
In the literature, three cases of small bowel obstruction have been documented in adult patients with situs inversus abdominalis. The first case, described by Brown et al. involved a 54-year-old woman who presented with a bowel obstruction secondary to a trans mesenteric internal hernia, the second case, by Mallick et al., described a bowel obstruction secondary to a volvulus on incomplete common mesentery. The third case is of a 38-year-old woman with a band occlusion bowel or internal hernia (2).
In general, surgery in a patient with SIA is difficult (11), so preoperative diagnosis is important to plan the surgical incision and abdominal procedures (12). Our patient was approached by median laparotomy, and exploration confirmed the diagnosis of visceral inversion (8).
## IV. CONCLUSION
Situs inversus totalis is a rare and asymptomatic congenital malformation. The latter is the cause of diagnostic and therapeutic difficulties encountered in many clinical situations, especially if the patient is not known to be a carrier of this malformation (13).
The association of situs inversus with intestinal obstruction on flange is very rare. Preoperative diagnosis of situs inversus is important for appropriate incision placement and surgical planning (12).
Generating HTML Viewer...
References
13 Cites in Article
Laparoscopic Roux-en-Y gastric bypass in a patient with situs inversus totalis: Case report, technical tips and review of the literature -PubMed.
Danika Jurat,Adrian Teo (2020). Small bowel obstruction with situs inversus abdominalis.
Ademolaolusegun Talabi,Oludayoadedapo Sowande,Adebayogbenga Tanimola,Olusanya Adejuyigbe (2013). Situs inversus in association with duodenal atresia.
A Kitasato,T Miyoshi,T Okamoto,A Yoneda,H Takeshita,T Kuroki (2022). Hepatocellular carcinoma with situs inversus totalis treated by caudate lobectomy: A case report.
Rahul Gupta,Varsha Soni,Prakash Valse,Ram Goyal,Arun Gupta,Praveen Mathur (2017). Neonatal intestinal obstruction associated with situs inversus totalis: two case reports and a review of the literature.
Di Buono,G Maienza,E Buscemi,S Randisi,B Romano,G Agrusa,A (2020). Acute appendicitis in a patient with situs viscerum inversus totalis: Role of laparoscopic approach. A case report and brief literature review.
H Bedioui,F Chebbi,S Ayadi,A Makni,F Fteriche,R Ksantini (2006). Cholécystectomie laparoscopique chez un patient porteur d'un situs inversus.
Nabonswindé Ouédraogo,Korotimi Sanogo,Mohamed Traoré,Jacques Simporé,Si Traoré (2020). A case report of management of gastric perforation in situs inversus totalis in a 45-year-old adult. A case report.
Deng Xiang,Jiannan He,Zimeng Fan,Fangfang Xiong,Gang Liu,Sufen Chen,Wu Wen,Jianfeng Li,Junhua Ai,Renhua Wan,Gongxian Wang,Jun Shi (2018). Situs inversus totalis with solid pseudopapillary pancreatic tumor.
R Gupta,V Soni,P Valse,R Goyal,A Gupta,P Mathur (2017). Neonatal intestinal obstruction associated with situs inversus totalis: two case reports and a review of the literature.
Kengo Shibata,Hideki Kawamura,Nobuki Ichikawa,Kazuaki Shibuya,Tadashi Yoshida,Yosuke Ohno,Shigenori Homma,Akinobu Taketomi (2018). Laparoscopic total gastrectomy for advanced gastric cancer in a patient with situs inversus totalis.
Abhishek Chinya,Kirti Naranje,Ankur Mandelia (2019). Situs inversus abdominalis, polysplenia, complex jejunal atresia and malrotation in a neonate.
E Masson Situs inversus totalis révélé par un syndrome occlusif : à propos d'une observation.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Mounir Bouali. 2026. \u201cA Case Report of Management of Intestinal Obstruction in a Patient with Situs Inversus Abdominalis\u201d. Global Journal of Medical Research - K: Interdisciplinary GJMR-K Volume 23 (GJMR Volume 23 Issue K4).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.