## I. INTRODUCTION
Haemorrhoids are very common in everyday life. They may be primarily due to genetics, a natural result of human adaptation to the upright posture, straining to pass constipated stools, or secondary to rectal cancer, pregnancy, uterine tumors, chronic constipation, dysuria due to stenosis or enlargement of the prostate, and portal hypertension (1). In the past, the varicose vein theory prevailed and it was believed that haemorrhoids were caused by varicose veins in the anal canal. Now the slippage theory of the inner wall of the anal canal is popular. This suggests that haemorrhoids develop when the anal cushions supporting tissue break down or degenerates. Thus haemorrhoids is the pathological term describing an abnormal displacement of the anal cushions leading to dilated veins. There are usually three main anal cushions located at the right front, right back and left side of the anal canal, and various numbers of smaller anal cushions located in between. The anal cushions of patients with haemorrhoids show obvious pathological changes. These changes include abnormal venous dilation, vascular thrombosis, degenerative processes of collagen fibers and fibroelastic tissue, and deformation and tearing of the subepithelial muscles of the anus (2). Haemorrhoids can be classified in different ways. Mainly divided into internal type, external type and mixed type. Internal haemorrhoids lie above the dentate line and are covered with mucous membranes, while external haemorrhoids lie below the dentate line and are covered with skin (3). Another classification tells us that haemorrhoids range from grade I (symptomatic bleeding only) to grade IV (prolapsed haemorrhoids). A third classification identifies haemorrhoids based on their anatomical location, where the 3, 7, 11 o'clock positions are considered primary and the area between the three points is secondary (4). While grades I and II haemorrhoids can be managed conservatively, grades III and grade IV haemorrhoids require surgery (5). Open haemorrhoidectomy has long been perceived by patients as an inherently painful procedure. Reducing post-haemorrhoidectomy pain is an important goal, with the ultimate goal of reducing the length of hospital stay and the likelihood of day surgery. Haemorrhoidectomy performed by conventional techniques causes considerable postoperative pain (6). MIPH (Minimally Invasive procedure for Haemorrhoids) is a new concept used to overcome these problems. Stapled haemorrhoidopexy for prolapsed haemorrhoids are conceptually different from excisional haemorrhoidectomy. It is not associated with the pain
usually associated with resection of the sensitive anoderm (7).
### a) Open haemorrhoidectomy
In an open procedure, the internal villous mass is separated from the internal sphincter fibers by separating the mucus from the skin. A trans fixation suture is bound at the base of the pile mass pedicle, and the pile is excised distal to it. Each haemorrhoid is treated in this way, leaving a mucocutaneous bridge.
# b) The Minimally Invasive
MIPH involves suturing the mucosal and submucosa veins using a stapling device, by tightening around the stapler head by a purse string suture. Take care to move the purse string at least $4\mathrm{~cm}$ above the dentate line. Secure and lock the stapler for 45 seconds holding the stapler along the axis of the anal canal. Then gently extract with a donut of excised tissue. All bleeding points are closed with haemostatic sutures.
## II. PATIENTS AND METHODS
### a) Study design
A Hospital based prospective type of analytical study.
### b) Site of study
### c) Type and Duration of Study
The study is a prospective analytical study in patients who are operated for Grade III, Grade IV haemorrhoids by either OPEN or MIPH presented in Shri Mahant Indresh Hospital, Patel Nagar, Dehradun with complaints of mass and/or bleeding per rectum. Study will be conducted over 18 months time period.
### d) Study planning
After obtaining consent of the patient for participation, all patients admitted through surgery OPD with Grade III or IV internal haemorrhoids, will be explained about both the procedures and depending upon patient's preference of procedure, patients will be divided into two groups. Group A will undergo open haemorrhoidectomy, whereas Group B will undergo MIPH. Both groups will receive injections of Diclofenac AQ 1 ml at the end of procedure and Diclofenac AQ IV twelve hourly post operatively. Breakthrough pain will be treated by Injection Tramadol. Both groups of patients will be assessed by visual scale at 12, 24, 48 hours post-operatively. Duration of surgery, duration of hospital stay, intra-operative bleeding along with any incidence of post-operative urinary retention, bleeding, rectal discharge for first 48 hours will be recorded. Patient will be followed up telephonically for 3 months for any symptoms suggestive of Anal stricture, incontinence or recurrent bleeding and called to OPD for re-examination, if required.
### e) Data collection tools and techniques
Data will be collected on clinical, lab results and proctological findings and follow up examination according to the proforma attached.
### f) Inclusion criteria
All patients with Grade III/IV uncomplicated haemorrhoids undergoing haemorrhoidectomy by open or MIPH methods.
### g) Exclusion criteria
1. Haemorrhoids secondary to any other condition like colonic malignancy.
2. Patients having fissures and/or fistulas associated with piles.
3. Patients having full thickness rectal prolapse with piles.
4. History of anal incontinence.
5. Rectocele.
6. Patients with anal stenosis.
7. Patients with any other systemic disease like renal failure, liver disorders, bleeding disorders.
### h) Study planning
- All eligible patients will be properly counselled and explained about the nature and purpose of the study. Secrecy and confidentiality will be maintained.
- Institutional ethical committee permission will be taken accordingly.
- After informed written consent, patients will be recruited into the study.
- Patient will be studied as per the working proforma attached.
- Valid and appropriate statistical tests will be applied in the data collected to obtain results.
## III. OBSERVATION AND RESULTS
A hospital based prospective analytical study was conducted at Department of Surgery, Shri Mahant Indresh hospital, Dehradun, India. Study aimed to compare the two surgical modalities to treat haemorrhoids namely Open haemorrhoidectomy and Minimally Invasive Procedure for Haemorrhoid (Stapled Haemorrhoidectomy) by comparing their immediate and early post-operative complications. Patients were allocated into two groups based on their choice of surgical intervention after thoroughly explaining the pros and cons of each procedure and written informed consent: Group A underwent Conventional haemorrhoidectomy and Group B underwent MIPH. Both groups received injections of Diclofenac AQ 1 ml at the end of procedure and Diclofenac AQ IV twelve hourly post operatively. Breakthrough pain was treated by Injection Tramadol. Both groups of patients were assessed by visual scale at 12, 24, 48 hours postoperatively. Duration of surgery, duration of hospital stay, intra-operative bleeding along with any incidence of post-operative urinary retention, bleeding, rectal discharge for first 48 hours was recorded. Patient was followed up telephonically for 3 months for any symptoms suggestive of Anal stricture, incontinence or recurrent bleeding and was called to OPD for re-examination, if required. Following observations were made during the study:
1. The mean age of the study cases was 43 years with no significant difference between study groups (p-0.47).
2. Almost identical gender distribution was observed among the two groups with a ratio of male: female being 2:1.(p-1.0).
3. No significant difference were observed between the two study groups based on presentation of patients - grade (p-0.794), pain during defecation (p-0.44), bleeding per rectum (p-0.07) and mass per rectum (p-0.77).
4. The mean operative time between two groups showed a significant difference with mean operative time for Group B MIPH being 31.24 as compared to 35.08 of Conventional haemorrhoidectomy $(p < 0.001)$. But a time difference of 4 minutes can be ignored for all practical purposes.
<table><tr><td>Type of Surgery</td><td>Mean</td><td>SD</td><td>P Value</td></tr><tr><td>CONVENTIONAL</td><td>35.08</td><td>2.66</td><td rowspan="2">0.001</td></tr><tr><td>MIPH</td><td>31.24</td><td>2.33</td></tr></table>
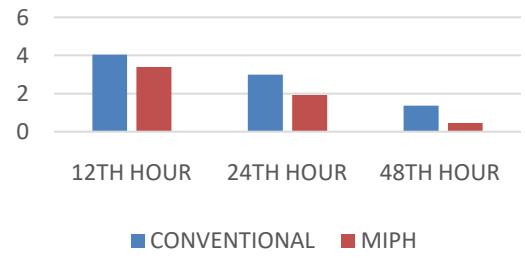
5. The mean VAS score at the end of 12 hours was 4.04 in Group A as compared to 3.4 in Group B (p-0.0004). By the end of 24 hours the mean VAS score for Group A was 03 as compared to 1.92 for Group B (p-0.0001). The mean VAS score at 48 hours showed no significant difference among the two groups (p-0.5461).
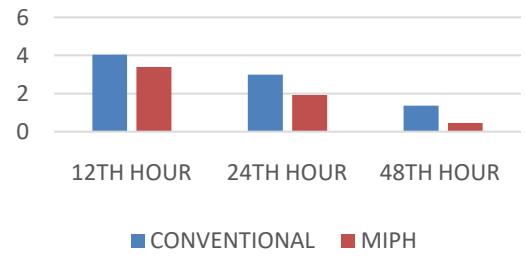
PAIN SCORE (VAS)
6. The breakthrough analgesic requirement was significantly high for Group A (required by 7 out of 25 patients) as compared to Group B (required by 1 out of 25 patients) (p-0.0).
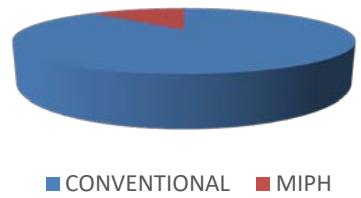 BREAKTHROUGH ANALGESIA
7. The mean duration of hospital stay in Group B was significantly low 3.04 days as compared to Group A 4.92 days $(p < 0.0001)$.
<table><tr><td>Duration</td><td>CONVENTIONAL</td><td>MIPH</td><td>P value</td></tr><tr><td>Mean days</td><td>4.92</td><td>3.04</td><td><0.0001</td></tr></table>
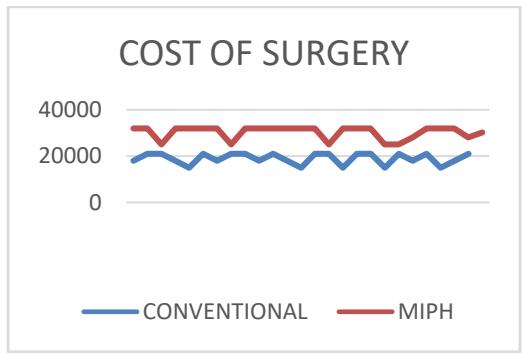
8. The mean cost of surgery for Group A was 18,960 as compared to 30,280 for Group B (p-0.001). The significant difference of 11,320 is attributed to the use of stapler gun used in MIPH.
9. There was no significant difference noted among immediate complications – urinary retention (p-0.29), post operative bleed (p-0.55) or early complications – anal stricture (0.55), anal incontinence or recurrence (p-0.16).
## IV. DISCUSSION
### a) Baseline data
In our study the mean age of Group A was 41.8 ranging from 18 to 70, for Group B mean age was 44.52 ranging from 15 to 78. The demographic age variable is comparable in both the samples and is age matched with a P value of 0.47. In their study Dr Nambalu Malyadri et al of 80 patients, found that study cases had a mean age of 34 for patients undergoing Conventional haemorrhoidectomy and 35 for patients undergoing MIPH with no particular predisposition to particular age group (8). Out of 60 patients that underwent similar case study conducted by Dr Yogesh Yadav et al, the mean age for Conventional haemorrhoidectomy was 44.77 and those who underwent MIPH was 45.53 (9). Similar results were found in case studies held by Dr Shalabh Gupta et al, Dr P Krishna Kishore et al and Dr Varun Raju et al.
In our study out of 50 patients 34 (68%) were males and 16 (32%) were females. Among the 34 male patients 17 (50%) were operated in Group A by Conventional method And 17 (50%) were operated in Group B with MIPH. Among the 16 females 8 (50%) were operated with Conventional method in Group A and 8 (50%) were operated by MIPH in Group B. Gender distribution is matched with P value of 1.0. In study conducted by Dr Yogesh Yadav et al a Male predominance of 52 (86.7%) was observed. Among 80 patients who underwent case study trials, Dr Shalabh Gupta et al, 49 were males (61.25%) and 31 were females (38.75%) (10). Similar results were found in case study conducted by Dr P Krishna Kumar et al (11).
### b) Presentation of patient
Patients with haemorrhoids often present with complaints of pain while defecation, bleeding per rectum, something coming out of anal canal (mass per rectum) and itching. Painless bleeding associated with bowel movements with or without intermittent tissue protrusion is the most common complaint of patients with symptomatic internal haemorrhoids. Depending upon the grade of haemorrhoid, the line of treatment varies. Grade I and II are usually managed conservatively while Grade III and IV require a much active plan of care and surgical intervention.
In our study out of 25 patients who underwent conventional haemorrhoidectomy, 16 patients had Grade III haemorrhoids while 09 had Grade IV haemorrhoids while out of 25 patients who underwent MIPH, 15 had Grade III haemorrhoids while 10 had Grade IV haemorrhoids and were grade matched with a P value of 0.77. Although study conducted by Dr Shailendra Pal Singh et al of 60 patients showed contradiction to our study with cases of Grade III haemorrhoids being $93.3\%$ and that of Grade IV haemorrhoids being $6.7\%$ (p-0.038) (12).
In our study, out of 25 patients who underwent conventional haemorrhoidectomy, 22 (88%) patients presented with complaints of pain during defecation while 20 (80%) presented with complaints of pain among patients who underwent MIPH, 19 (76%) presented with complaints of bleeding PR and 12 (48%) presented with complaints of mass PR while out of 25 patients who underwent MIPH, 20 (80%) presented with complaints of pain, 13 (52%) presented with complaints of bleeding PR and 13 (52%) presented with complaints of mass PR. This is in concordance with the studies conducted by Dr Nambula Malyadri et al and Dr Yogesh Yadav et al which showed no significant difference in the presenting complaints among individuals undergoing Conventional haemorrhoidectomy and MIPH.
### c) Intra-operative findings
The duration of operation was compared between two groups.
In our study the mean operating time for Group A Conventional method was 35.08 when compared to MIPH Group B mean 31.24, the duration of surgery in MIPH group was significantly lower by 4 minutes when compared to the Conventional Group with a P-value of less than 0.001. There was no intraoperative complications and all the pedicles were ligated without any failure. The time difference of less than 4 minutes can be neglected as it did not affect the post operative morbidity. The findings were in concordance with studies conducted by:-
- Dr Shalabh Gupta et al who conducted a case study of 60 individuals, among 30 individuals who underwent Conventional haemorrhoidectomy, the mean duration of surgery was 46.73 minutes while that for MIPH was 25.9 minutes (p<0.001)
- Dr Nambula Malyadri et al observed similar findings with mean duration of surgery for Conventional haemorrhoidectomy was 50 minutes and for MIPH was 40 minutes (p-<0.001)
- Dr Yogesh Yadav et al case study produced identical data to study conducted by Dr Shalabh Gupta et al with mean duration for Conventional haemorrhoidectomy being 46.73 minutes while that for MIPH being 25.90 (p-<0.001)
- Mean duration for Conventional Haemorrhoidectomy was 36.2 minutes while that for MIPH was 28.76 (p<0.05) in study conducted by Dr Varun Raju et al (13).
### d) Post operative assessment
The most common encountered and troublesome morbidity post haemorrhoidectomy is the pain. Emphasis has been made to counter the problem as the pain is so excruciating that it can lead to other morbidities like urinary retention and constipation. Various approaches to haemorrhoids have been advised over time keeping in mind the post procedural pain associated with Conventional haemorrhoid- dectomy.
In our study the post operative pain was assessed and was scored using visual analogue scale from 0 to 5. Patients were administered analgesics as required.
Comparison was done between two groups with regards to pain VAS score. The pain scores were noted at $12^{\text{th}}$ hour, $24^{\text{th}}$ hour, $48^{\text{th}}$ hour post operatively. In our study the mean pain score at $12^{\text{th}}$ hour was 4.04 for Group A (Conventional haemorrhoidectomy) and 3.4 for Group B (MIPH). The pain score at $12^{\text{th}}$ hour was significantly low in stapled haemorrhoidectomy with P value of 0.0004. The mean score at $24^{\text{th}}$ hour for Group A was 03 and 1.92 for Group B which was also statistically significant with p value of 0.0001. But the mean pain score at $48^{\text{th}}$ hour showed no significant difference between the two groups. Hence the post operative pain was significantly low in stapled haemorrhoidectomy group in comparison to Conventional approach. The data is in concordance with the studies conducted by Dr Shalabh Gupta et al and Dr Yogesh Yadav et al for significant pain comparison at $12^{\text{th}}$ and $24^{\text{th}}$ hours but contradicting to data for later stage.
Dr Shalabh Gupta et al in their study noted a mean pain score of 6.87 in patients who underwent Conventional haemorrhoidectomy as compared to 3.73 among patients who underwent MIPH (p<0.0001), at $24^{\text{th}}$ hour among the individuals who underwent Conventional haemorrhoidectomy the mean pain score was 5.67 as compared to 2.10 among patients who underwent MIPH (p-<0.0001). The study also showed significant mean pain score difference on post operative day 7 among the two groups.
- Dr Yogesh Yadav et al in their study noted a mean pain score of 6.90 in patients who underwent Conventional haemorrhoidectomy as compared to 3.37 among patients who underwent MIPH (p<0.0001), at $24^{\text{th}}$ hour among the individuals who underwent Conventional haemorrhoidectomy the mean pain score was 3.57 as compared to 1.43 among patients who underwent MIPH (p<-0.0001). The study also showed significant mean pain score difference on post operative day 7 among the two groups.
In our study the requirement for breakthrough analgesia for Group A conventional method was 07 out of total 25 patients while that for MIPH Group B was 01 out of total 25 patients, the breakthrough analgesia requirement in MIPH group was significantly low when compared to the conventional group and has a P value of 0.02
### e) Duration of hospital stay
Faster wound healing, better patient compliance, less post operative pain along with shorter stay at hospitals has resulted in better acceptability of stapled haemorrhoidectomy over the years.
In our study the mean duration of stay for Group A conventional method was 4.92 days while that for MIPH Group B was 3.04 days, the duration of hospital stay in MIPH group was significantly low when compared to the conventional group and has a P value of less than 0.0001. The results are consistent with the findings of Dr Shalab Gupta et al (Conventional method - 5.93 days, MIPH -2.07 days (P - <0.0001)), Dr Yogesh Yadav et al (Conventional method - 5.93 days, MIPH - 1.07 days (P - 0.001)), Dr NambulaMalyadri et al (Conventional method - 3 days, MIPH - 1 day (P - <0.001)) and Dr Varun Raju (Conventional method - 2.3 days, MIPH - 1.1 days (P - <0.05)).
#### Cost of surgery
In our study the mean operating cost for Group A conventional method was 18960 when compared to MIPH Group B mean 30280, the cost of surgery in MIPH group was significantly higher by 11320 when compared to the conventional group with a P value of 0.001. It is in concordance with the findings of study conducted by Dr Yogesh Yadav et al who reported a mean difference of Rs 22,000 among the two groups mainly attributing the findings to the cost of MIPH stapler guns.
### g) Post operative complications
In our study the immediate complications among Group A conventional method were comparatively higher being 05 out of total 25 patients (Urinary Retention=03, Post operative Bleeding=02) while that for MIPH Group B was 02 out of total 25 patients (Urinary retention=01, Post-operative bleeding=01), the immediate complications in MIPH group was comparatively low when compared to the conventional group.
In present study the early complications among Group A conventional method for recurrences were comparatively higher being 04 out of total 25 patients while that for MIPH Group B was 01 out of total 25 patients, no anal incontinence cases were reported in either of groups, while anal stenosis incidence were high In MIPH Group B with 02 out of total 25 patients as compared to 01 out of 25 patients for conventional method Group B.
In present study the post operative complication such as bleeding, urinary retention, incontinence, recurrence and anal stenosis were noted in both the groups following Conventional haemorrhoidectomy And MIPH without any significant difference. This is in concordance with the studies conducted by Dr Shalab Gupta et al, Dr Nambula Malyadri et al, Dr Yogesh Yadav et al and Dr Varun Raju et al. However a contradiction can be found to the findings among the post operative bleeding with a significant difference among the two groups in studies conducted by Dr Nambula Malyadari et al who reported a significant difference regarding post operative bleed among individuals who underwent Conventional haemorrhoidectomy (12) as compared to those who underwent MIPH (2)(P - <0.001) while Dr Shalabh Gupta et al reported greater number of individuals who underwent MIPH (8) to have post operative bleed when compared to individuals who underwent Conventional haemorrhoidectomy (1)(P - 0.05). Dr Yogesh Yadav et al showed a significant association between anal incontinence and individuals who underwent Conventional haemorrhoidectomy (6) as compared to those who underwent MIPH (0) (P - 0.024).
## V. CONCLUSION
There are reports of better post operative outcome following stapler haemorrhoidectomy in terms of pain and wound healing. Both conventional and stapler approach are less expensive and safe, easy to perform with satisfactory results. In present study we found that the important advantages of MIPH over the Milligan-Morgan conventional approach is that there are reduced pain in post operative period with fewer less breakthrough analgesics requirement to control the pain, leading to reduced hospital stay and early return to work along with better wound healing rate. but the stapled technique has these advantages at the expense of higher cost and surgical expertise. The present study thus recommends MIPH stapler haemorrhoidectomy has better results over conventional approach for Grade III and Grade IV haemorrhoids.
Generating HTML Viewer...
References
13 Cites in Article
Peter Chong,David Bartolo (2008). Hemorrhoids and Fissure in Ano.
(2012). Unknown Title.
O Kaidar-Person,B Person,S Wexner (2007). Hemorrhoidal disease: a comprehensive review.
P Alonso-Coello,M Marzo Castillejo (2003). Dispepsia y redes neuronales.
Brian Kann,Charles Whitlow (2004). Hemorrhoids: diagnosis and management.
S Jayaraman,P Colquhoun,R Malthaner (2006). Stapled versus conventional surgery for haemorrhoids.
J Tjandra,M Chan (2007). Systematic review on the procedure for prolapsed and hemorrhoids (stapled hemorrhoidopexy).
Nambula Malyadri,Veera Jayachandra Allu (2021). A Prospective Comparative Study of Stapler Hemorrhoidectomy Vs Open Haemorrhoidectomy (Milligan Morgan) in its Outcome and Postoperative Complications.
Yogesh Yadav (2018). Minimal invasive procedure for haemorrhoids (MIPH) versus Open haemorrhoidectomy: a comprehensive study.
Shalabh Gupta*,Apoorv Goel,Yogesh Yadav,Prakhar Garg,Tripta S Bhagat (2019). A comparative study between open haemorrhoidectomy and minimal invasive procedure for haemorrhoids (MIPH) in cases of grade III and IV haemorrhoids.
P Krishna Kishore,B Manju,G Sruthi,Obulesu (2016). Comparative study between stapler and open hemorrhoidectomy in the management of grade III/ IV hemorrhoids.
Shailendra Singh,Somendra Singh,Vipin Gupta,Kutubuddin Quadri,Mohit Gupta (2018). Comparison between stapler hemorrhoidectomy and open hemorrhoidectomy in the management of grade III and IV hemorrhoids: a prospective randomized study.
Raju Varun,Ramachandrer Thirumalagiri,Rao (2017). A Comparative Study of Open Haemorrhoidectomy with Minimally Invasive Procedure for Haemorrhoids.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Hirein H Malhotra. 2026. \u201cA Comparative Study of Open Haemorrhoidectomy with Stapler Haemorrhoidectomy (MIPH) in Relation to Immediate and Early Complications\u201d. Unknown Journal GJMR-I Volume 23 (GJMR Volume 23 Issue I1): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.