



I. INTRODUCTION
Amniotic fluid is a clear, yellow fluid which is found within the first 12 days following conception within the amniotic sac. It surrounds the growing baby in the uterus[^1]. It is colorless with slight to moderate turbidity. Amniotic fluid is necessary for human fetal growth and development. The fluid volume cushions the fetus, protecting it from mechanical trauma. Its bacteriostatic properties may helps to maintain a sterile intrauterine environment. The space created by the amniotic fluid allows fetal movement and aids in the normal development of both the lungs and the limbs2,3.
The rate of amniotic fluid production depends on the gestational age. It produced at a rate of 10 mL/week at first trimester, 50-60 mL/week from 19-25 weeks of gestation, so it increases progressively between 10 to 30 weeks of gestation. It measures about <10 mL at 8 weeks, 50 mL at 12 weeks, 400 mL at 20 weeks, 770 mL at 28 weeks, 1 L at 36-38 weeks. But after 36 weeks, volume decreases at a rate of 60 mL/week at 40 weeks gestation, so it measures 600-800 mL at 40weeks and subsequently decline in volume per week3.
Ultrasound is a safe method to estimate the AFV. A number of techniques to measure AFV are used. First method is to measure Maximum Vertical Pocket (MVP) depth. It refers to the vertical dimension of the largest pocket of amniotic fluid not containing umbilical cord or fetal extremities and measured at a right angle in the uterine surface. Oligohydramnios is considered if the depth of MVP cm and Polyhydramnios is considered if the MVP depth is cm. The second method is to measure Amniotic Fluid Index (AFI). It is calculated by first dividing the surface markings of the uterus into four quadrants using the linea nigra and umbilicus. The maximum vertical amniotic fluid pocket diameter in each quadrant not containing cord or fetal extremities is measured in centimeters and then the sum of these measurements constitutes the AFI. Oligohydramnios is labeled when AFI is cm and Polyhydramnios is labeled when AFI cm. The assessment of AFV in twin pregnancies is especially important, given their high perinatal mortality rate. The MVP technique seems to be the most appropriate in twins, using the same definitions that are used in singletons. The use of the AFI in twins has poor inter and intra observer variability, and therefore should not be used in clinical practice .
Oligohydramnios, occur in of all pregnancies and of post- date pregnancies . This may be evident in cases of leaking fluid from a tear in the amniotic membranes, measuring small in volume for a certain stage of pregnancy by ultrasonography or if the fetus is not moving as much as it would be expected to. It can also be occurs in mothers with a history of any of the medical conditions, like prior growth-restricted pregnancies, Hypertensive disorders in pregnancy, Problems with the placenta, (for example, abruption), Diabetic disorders in pregnancy, SLE and other autoimmune conditions, Multiple pregnancies (for example twins or triplets), Birth defects, such as kidney abnormalities, Delivering past the due date and other unknown reasons, known as idiopathic.
According to the American Pregnancy Association, polyhydramnios can be occurs in of all pregnancies[^1]. Fetal disorders that can lead to polyhydramnios include gastrointestinal disorders (duodenal or esophageal atresia, gastroschisis, and diaphragmatic hernia), Brain or nervous system disorders (anencephaly or myotonic dystrophy), Achondroplasia, Fetal heart rate problems, Infection, Beckwith-Wiedemann syndrome, Fetal lung abnormalities, Hydrops fetalis, Twin-to-Twin Transfusion syndrome and Rh incompatibility or Kell diseases. Poorly controlled maternal diabetes also increases the risk. Too much fluid can also be produced during multiple pregnancies[^3].
Polyhydramnios causes maternal symptoms like abdominal pain and difficulty breathing due to the enlargement of the uterus. Other complications include preterm labour, premature rupture of membranes, placental abruption, stillbirth, postpartum hemorrhage, fetal malposition, cord prolapsed[^3].
Amniotic fluid volume disorders can happen during any trimester but is more evident during second and third trimesters. During that time, there is a higher risk for loss of pregnancy, preterm birth, or neonatal loss of life[^4]. Associated birth defects are mostly the cause of abnormal amniotic fluid volume and also responsible for adverse perinatal outcome3,9.
II. METHODS
III. RESULTS
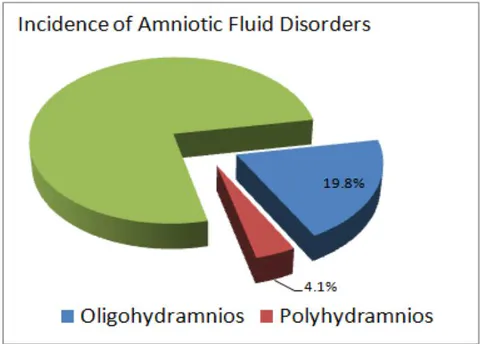
During the year of 2020 total 656 patients were admitted in Maternal-Fetal Medicine unit of Obs and Gynae department, Dhaka Medical College and Hospital, Bangladesh. Among them 130 (19.8%) patients were diagnosed as having oligohydramnios in their current pregnancy and 27 (4.1%) patients were diagnosed as having polyhydramnios (Fig 1).
The mean age of our patients having polyhydramnios were years. All patients oligohydramnios was years and were of south-east Asian origin.
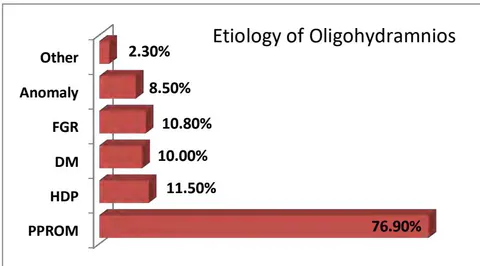
Most of the oligohydramnios (76%) were due to preterm prelabor rupture of membrane. Other associated conditions of oligohydramnios were hypertensive disorders of pregnancy and growth restricted fetus (11.5%), Diabetic disorders (10.0%), Anomalous fetus (8.5%) and undetermined causes (2.3%).
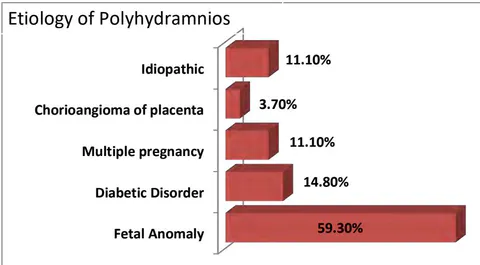
Polyhydramnios was mainly associated with fetal anomaly (59.3%) but a little percentage was associated with gestational diabetes (14.8%), multiple pregnancies (11.1%), chorioangioma (3.7%) and undetermined (11.1%) causes.
The total number of polyhydramnios patients 27 and 20 patients were delivered in our hospital. The mean gestational age of delivery was weeks. Among them 10 (50.00%) babies were born alive and 10 (50.00%) were still birth. 5 (25.00%) of the live babies needed admission in NICU and 4 (20.00%) of the admitted babies died during their neonatal period.
IV. DISCUSSION
Dhaka Medical College Hospital (DMCH) is the largest tertiary hospital of Bangladesh which is fully supported by government. High risk pregnancy patients came here from all over the country and got admitted in
Maternal Fetal medicine unit of Department of Obs and Gynae, for better management.
In this study the total number of admitted patient under Maternal Fetal Medicine unit of ObGyn department DMCH were 656 in the year 2020. Out of them 130 (19.8%) patients were diagnosed as having oligohydramnios and 27 (4.1%) patients having polyhydramnios in their current pregnancy. Bakhsh et al found incidence of oligohydramnios 11.7% and polyhydramnios 2.8% in a secondary care hospital of Saudi Arabia[^6]. As our hospital is a tertiary center and the current study was conducted in a high risk pregnancy unit so incidences are higher in our study.
The mean age of our patients having oligohydramnios was years and polyhydramnios were years. All patients were of south-east Asian origin.
Most of the oligohydramnios (76%) were due to preterm prelabor rupture of membrane. Other associated conditions of oligohydramnios were hypertensive disorders of pregnancy and growth restricted fetus (11.5%), Diabetic disorders (10.0%), Anomalous fetus (8.5%) and undetermined causes (2.3%). Bakhsh et al showed 13.7% Diabetic Disorders, 5.2% fetal anomaly but no hypertensive disorders among oligohydramnios patient[^6]. Lavanya B et al found 24% hyperhensive patients and 15% of growth restricted fetus with oligohydramnios[^7]. The inclusion of prelabor rupture of membrane in our study may be the most influential factor for making etiological difference from other studies.
Polyhydramnios was mainly associated with fetal anomaly (59.3%) but a considerable percentage was associated with gestational diabetes (14.8%), multiple pregnancies (11.1%), chorioangioma (3.7%) and undetermined (11.1%) causes. Bakhsh et al showed 42.9% diabetic disorder, 7.1% hypertensive disorders, 14.2% fetal anomaly among polyhydramniotic patients[^6]. Abele et al found 40% of the polyhydramnios cases as idiopathic[^10]. The percent of idiopathic in our study was found less may be caused by advancement of investigation facilities.
The total number of polyhydramnios patients 27 and 20 patients were delivered in our hospital. The mean gestational age of delivery was weeks. Among them 10 (50.00%) babies were born alive and 10 (50.00%) were still birth. 5 (25.00%) of the live babies needed admission in NICU and 4 (20.00%) of the admitted babies died during their neonatal period. Bakhsh et al showed of babies from polyhydramnios pregnancy as NICU admission. So polyhydramnios is a major factor for adverse perinatal outcome. This may be due to the strong association of anomaly babies and diabetic mothers.
V. CONCLUSION
To identify pregnancies with risk of poor perinatal outcomes, AFI measurement can be used as one of the important method. Ultrasound evaluation of abnormal amniotic fluid volume indicates a wide range of pregnancy complications and can predict adverse perinatal outcome for that pregnancies.
Recommendations for future research:
- To conduct large study in a more precise way so that the rare etiologies come in front.
- Long term outcome of babies should be followed to evaluate the consequences.
ACKNOWLEDGEMENTS
I would like to express my gratitude and acknowledge the following persons for their active participation and inspiration through-out this research work:
*All Subspecialty trainee of Maternal Fetal Medicine, Dhaka Medical College Hospital.
Conflict of interest: There is no conflict of interest in this study.
Funding: Self funding by authors.



