Fundamentally an intervention refers to an action that has an agenda and is aimed by the human being to create change (Midgley 2020) according to him if the intervention is an action aimed by the human being to create change, then systemic intervention is an action aimed at creating a change in the context of reflection to the system. The International Association of ergonomics (IEA) categorizes ergonomics into three specific domains: physical, organizational, and cognitive ergonomics. The physical domain is concerned with human anatomy, anthropometry, physiological and biomechanical characteristics associated with physical activity. The domain also consists of working environments and equipment, such as hand tools, workstations and lighting and ventilation in the workplace. The domain of the organization, referring to the concern for the optimization of work systems, including organizing and even work processes for example as a frequency of work, work cycle and rest, in addition to directing in performing work. The cognitive domain is related to mental processes, such as perception, memory, judgment, and motor response.
## I. INTRODUCTION
Numerous studies have found that ergonomic factors associated with MSD symptoms (Ashley et al. 2008; Xie et al. 2016). Adjustment of physical, organizational, and cognitive ergonomic factors aimed at reducing the physical and mental burden on employees certainly reduces the risk of employees getting work-related MSDs, especially upper limbs, neck or both. Physical ergonomic interventions include providing workspaces and equipment based on the principles of employee ergonomics and anthropometry. This will reduce physical tension to the body's skeletal system, thereby automatically reducing the risk of injury. For example, the use of a separate keyboard was found to reduce the severity of MSD pain in computer users (Tittiranonda et al. 1999). Engineering interventions are part of physical ergonomic interventions such as the use of adjustable platforms to prevent lifting from floor level can be used. Organizational ergonomic interventions consist of the optimization of working intervals with rest time for the skeletal system, thus indirectly reducing the risk of performing work in the long term. Among the examples is the extra rest time for tasks to lock data into the system (Wendsche & Lohmann-haislah 2016). In addition, exposure training to good ergonomic practices and principles (Baydur & Demiral 2016) is also part of the organization's ergonomic interventions. Administrative interventions focus on changing tasks or work designs such as the introduction of work rotation, or the implementation of safe work policies, such as at least two people required during large and heavy load lifts. Cognitive ergonomic interventions consist of improving mental abilities of processing such as perception, memory and logical considerations, in addition to that also motor response through work process modification as well as training that is a safe working practice as well as part of cognitive ergonomic interventions. This will directly reduce mental workload, increase reliability, and reduce errors. However, it may only have an indirect effect in reducing tension in the body's skeletal system physically. Behavioural interventions focus on individual behaviour. Behavioural interventions refer to focusing on fitness or strength levels. In line with the Guidelines on Ergonomic Risk Assessment at Work by the Department of Occupational Safety and Health, Ministry of Human Resource in 2017. Early detection of symptoms should be emphasized through sensory detection or skeletal discomfort.
Generally, polytechnic students will be burdened with a total of around 25 hours of formal learning per week depending on the credit hours taken for prime students. At least 4 hours of it is practical work. The implementation of this learning period continues for 14 weeks of lecture for each semester. The practice of welding engineering is one of the practical subjects for students who major in mechanical engineering, and it is a mandatory graduation requirement. Generally, students will take practical subjects for 3 semesters starting from semester 1 to 3 and will be connected with 2 semester as a semester 4 and 5 in project subjects. For the practical subject of welding, there are 3 mandatory tasks which are to continue meeting, connect the open 't' and continue the contact every semester. This 4-hour-a-week period requires students to perform their assignments properly and quality, as there are certain rubrics that form the basis of the assessment, and the impact will be on the grade of value points that will be obtained at the end of the semester.
MSD can occur when performing repetitive tasks continuously, working in abnormal and awkward postures, doing heavy physical work, and using strong energy.
A common ergonomic hazard factor present during the welding process is a static and prolonged posture position, in addition to that when the posture is awkward and exposure to fumes. These ergonomic risk factors may cause MSD associated with welding activities. MSD is an injury and disease that affects the condition of muscles, nerves, tendons, ligaments, blood vessels and bones. As a result, the welder easily suffers from fatigue, lethargy, and suffering from injuries. Therefore, if the welder is not in a good level of fitness to perform the task, the quality of welding can also be affected. Poor welding quality occurs when there are defects in the welding area such as porosity, excessive splashing, incomplete connection, lack of penetration rate, excessive penetration, burning and bending (Waters & Dick 2015) (Jaffar et al. 2011) (Kalpakjian & Schmid 2009).
Static position refers to a person who is in the same position or posture in a period throughout the performance of work. In order to maintain a static posture while performing the task, this condition will cause muscle tension or fatigue which is a factor in the risk of MSD. The duration of the posture position of the body, the awkward position of the posture, and the level of energy used will affect the degree of risk of injury. Static position can also be referred to as static load.
Based on epidemiological studies, occupational factors can potentially increase the risk of musculoskeletal disorders. The frequency of musculoskeletal complaints varies significantly between different employment groups. Therefore, different occupational factors can cause different MSD pain.
Basically an intervention refers to an action that has an agenda and is aimed at by human beings to create change (Midgley 2020) according to Midgley also If an intervention is an action aimed by man to create change, then systemic intervention is an action aimed at creating a change in the context of reflection to the system. The International Association of ergonomics (IEA) catalyses ergonomics into three specific domains: physical, organizational and cognitive ergonomics. The physical domain is as concerned with human anatomy, anthropometry, physiological and biomechanical characteristics as they relate to physical activity. The domain consists of working environments and equipment, such as hand tools, workstations and lighting and ventilation in the workplace. The organization's domain focuses on job system optimization, including organization and work processes, such as work frequency, work-break cycles, and directing in performing work. The cognitive domain is related to mental processes, such as perception, memory, decision-making and motor response. Therefore, the ergonomics interventions developed should cover all three ergonomic domains, namely physically, organizational and cognitive. Good ergonomic interventions must be carried out prior to the occurrence or reporting of skeletal disorders. It is one of the proactive or preventive methods in ensuring the health of a community such as students, lecturers and employees at a good level. However, reactive action in the form of correction should also be taken to curb the symptoms of skeletal disorders becoming more serious.
## II. LITERATURE REVIEW
The 3 'E' injury prevention framework is a common injury prevention framework. Usually $3'E$ will refer to Education, Engineering and Enforcement. The acronym $3'E$ refers to education which is related to knowledge and translation of skills, engineering i.e., environment and building materials and materials built and not built as well as enforcement i.e., compliance with OSH policies, laws and regulations related to OSH. The 3 E approach was created in 1923 by the director of the Kansas City Safety Council, Julien H Harvey, in his discussion on road traffic safety. Through the passage of time the 3 E approach has been expanded by including additional 'E' such as Exposure, exam, equality and even emergency. This framework actually focuses more on considering human behaviour.
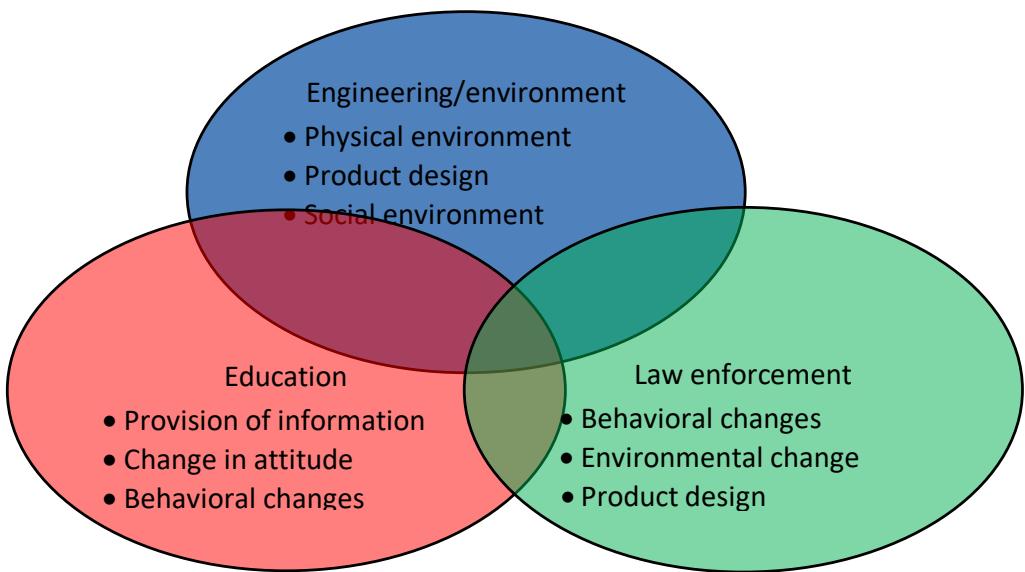 Figure 1: 3E model of injury prevention
Macro Ergonomics is a human-cantered ergonomic because it considers the professional and psychosocial characteristics of employees in planning System work and then bring the design of the working system through the ergonomic design of specific jobs and related hardware and software interfaces. According to Hendrick and Kleiner (2001), macroergonomics is a top-down approach, a strategic approach to analysis, The main focus on macroergonomics is that the analysis and design of the working system will participate in a balanced manner. (Imada 2007). Macro-ergonomics human-cantered and ergonomic participation are the main focus in macroergonomics involving workers at All organizational stage in the design process. (Hal W. Hendrick 2000) has defined several ergonomic 'levels'. These include:
- Human machine: hardware ergonomics: It mainly relates to physical characteristics and human perception to control designs, displays, seats, workstations and is used for the arrangement of related workspaces.
- Human environment: environmental ergonomics: It deals with the effects of various physical environmental factors, such as lighting, heat, cold, sound and vibration, human performance, and is used to design physical environments for humans.
- Human software: cognitive ergonomics: It is related to the way people think, conceptualize, and process information, and is used for software design.
- Human work: work design ergonomics: It is related to job design to ensure the correct workload and characteristics such as multitasking or having different meaningful things to do in work identity or a sense of job solidity, importance or autonomy or control of the perceived meaning of work over one's work, and feedback or knowledge of results.
Human organization: macro-ergonomics: It relates to employee intermediaries with the organizational design of a more effective work system to use both personnel and technologies used in the system in responding to the external environment of the organization.


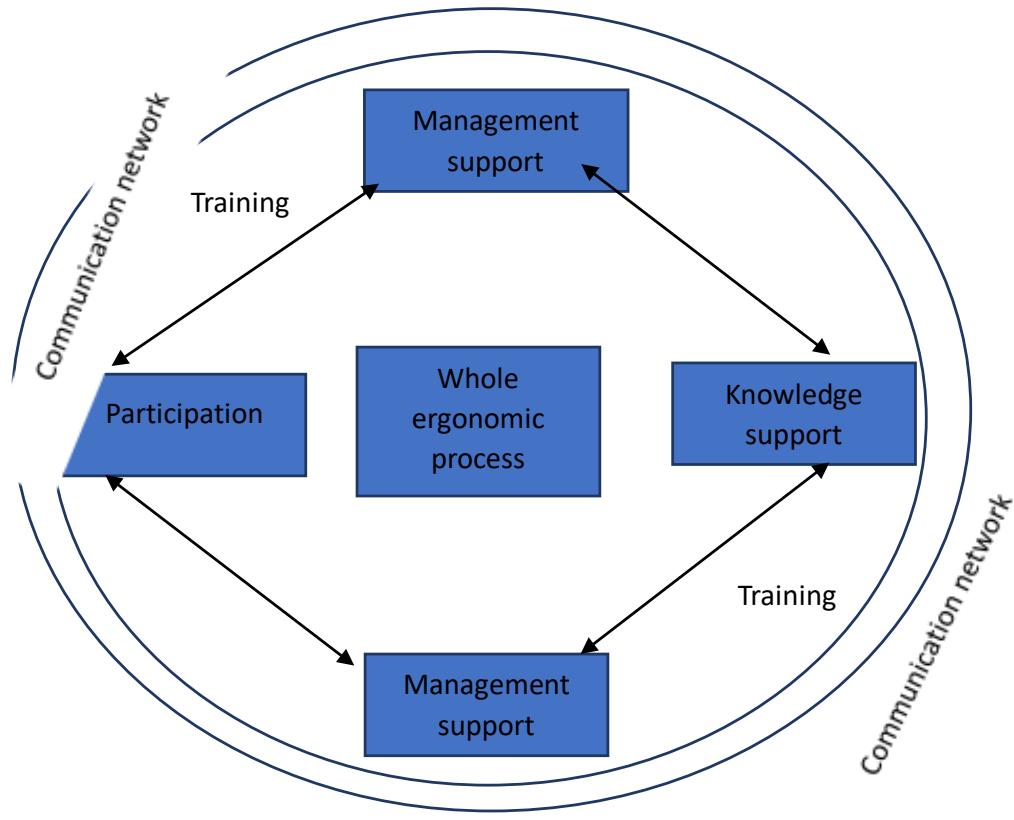 Figure 1: Overall evaluation model of ergonomics and intervention process
Since ergonomic interventions are a process of improvement in all aspects of the organization's activities, the appropriate model for implementing interventions should aim to include all aspects of the organization to address as many types of issues as possible. In general, these issues relate to technological innovation and organizational and environmental changes. From this point of view, (Hosseini et al. 2012), proposes as in Figure 2 for ergonomic interventions based on four principles:
- Management and logistics support,
- Knowledge support,
- HR participation and
- Motivation through evaluation, recognition and reward.
Thus, ergonomic intervention is a process developed by managers, staff and members of the working group through contact. Another element of the model is feedback, prepared and designed on the basis of four principles of this model. Corresponding communication systems and networks are established between those involved in the intervention to establish this framework to ensure continuity. Training is also seen as a core element of the model, as ergonomic interventions begin and end with training. Ergonomic training and knowledge is an ongoing process in which the state of intervention of ergonomic knowledge is provided in the system (Abarghouei, Nasab, 2012). Training allows the transmission of organizational knowledge and helps participants understand how to use certain ergonomic interventions in different working groups. In addition, training ensures a deep understanding of how to actually implement a step or decision that is not ergonomic. Ergonomic intervention is a long-term process and it requires the constant support of management. Feedback becomes important when it is the only indicator of the measures that have been implemented fulfilling the original goal. Feedback should be in the form required by a particular group. "The management system should encourage working team members to be active and continue to participate. Therefore, for a successful and continuous intervention process, the evaluation and monitoring system should be considered (Hosseini et al. 2012). The intervention process should be evaluated at regular intervals by a management-certified assessment team to confirm the progress of the intervention. Along with a robust evaluation system, good progress needs to be encouraged and praised. Those involved in this intervention should be encouraged to collaborate among members of the organization. Typically, activities cause increased production, improvement in quality of work, improvement of health, safety and satisfaction of staff and job safety (Abarghouei, Nasab, 2012). In order
to improve intervention results and effectiveness, management needs to provide adequate support for all measures and implementation efforts. The main thing is that top management must turn ergonomically related work procedures into a significant part of the organizational culture. Communication between top management and employees can bring the possibility of avoiding certain risks and quickly addressing all the issues and job risks that frighten the organization.
This model has a systemic structure because all of the above elements are interconnected and operate together with the aim of ensuring efficient ergonomic interventions.
## III. DATA AND FINDING
In order to ensure that this intervention is reliable and able to achieve the Desire as a leading indicator, the views of the welding experts comprising academics and practitioners should be considered.
### a) Cohen Kappa Test
The study protocol questions as listed in Table 3.5 of the interview question protocol. Where it is built through the results of intervention theories such as the intervention model developed in the previous section.
Table 1: The value of the cohen kappa index and the consent scale
<table><tr><td>Cappa value</td><td>Scale of consent</td></tr><tr><td>Below 0.00</td><td>Very weak</td></tr><tr><td>0.00-0.20</td><td>Weak</td></tr><tr><td>0.21-0.40</td><td>Moderately weak</td></tr><tr><td>0.41-0.60</td><td>Simple</td></tr><tr><td>0.61-0.80</td><td>Good</td></tr><tr><td>0.81-1.00</td><td>Very nice</td></tr></table>
The value of Cohen Kappa can be calculated by referring to the following formula:
$$
K = \frac {f _ {a} - f _ {c}}{n - f _ {c}}
$$
Based on the following formula, the calculation of the Cohen Kappa reliability index for ergonomic intervention interviews at TVET institutions in Table 3.12 such as following:
Where:
K - Coefficient value fa - Frequency of consent
fc - Frequency of $50\%$ expected agreement
N – Number of units assessed by consent
Based on the following formula, the calculation of the Cohen Kappa reliability index for ergonomic intervention interviews at TVET institutions in Table 3.12 such as following:
Table 2: Data Cohen Kappa (K) between expert panels
<table><tr><td colspan="6">Cohen Kappa (K) test</td></tr><tr><td rowspan="2" colspan="3"></td><td colspan="2">2</td><td rowspan="2">Total</td></tr><tr><td>yes</td><td>no</td></tr><tr><td rowspan="4">1</td><td rowspan="2">yes</td><td>Count</td><td>10</td><td>1</td><td>11</td></tr><tr><td>Expected Count</td><td>6.5</td><td>4.5</td><td>11.0</td></tr><tr><td rowspan="2">no</td><td>Count</td><td>0</td><td>6</td><td>6</td></tr><tr><td>Expected Count</td><td>3.5</td><td>2.5</td><td>6.0</td></tr><tr><td rowspan="2" colspan="2">Total</td><td>Count</td><td>10</td><td>7</td><td>17</td></tr><tr><td>Expected Count</td><td>10.0</td><td>7.0</td><td>17.0</td></tr></table>
Table 3: Kohan Kappa Analysis
<table><tr><td colspan="6">Symmetric Measures</td></tr><tr><td colspan="2"></td><td>Value</td><td>Asymp. Std. Errora</td><td>Approx. Tb</td><td>Approx. Sig.</td></tr><tr><td>Measure of Agreement</td><td>Kappa</td><td>0.876</td><td>0.119</td><td>3.640</td><td>0.000</td></tr><tr><td colspan="2">N of Valid Cases</td><td>17</td><td></td><td></td><td></td></tr><tr><td colspan="6">a. Not assuming the null hypothesis.</td></tr><tr><td colspan="6">b. Using the asymptotic standard error assuming the null hypothesis.</td></tr></table>
b) Ergonomic Intervention Questions
1. Is there ergonomic training or ergonomic intervention program to students of your institution
2. What is the level of success of the program in your institution now
3. Who should be involved in ergonomic intervention programmes or ergonomic training
4. What is the most important element in the development of ergonomic training or ergonomic intervention programs to students
5. What are the data or studies conducted on your institution in relation to MSD injuries
6. If students are given adequate training and are aware of ergonomic hazards, can MSD injuries in your institution be avoided
7. In the context of ergonomic programmes in tvet institutions, student behaviour is a factor that contributes to ergonomic injury (MSD) during practice
8. Should a comprehensive ergonomic intervention programme be applied in the syllabus related to the workshop
9. What exposure to ergonomic interventions is required for students to leave work after the end of employment
10. Is there a need in integrating theoretical and practical related ergonomic interventions in any subject during study
11. What is the main content needed in ensuring that ergonomic interventions deliver good results
12. Do tvet institutions require a suitable ergonomic intervention program for the entire tvet system (1 system fit to all)
13. Other things to include in the development of the ergonomic intervention program to be developed
The result of the expert's view states that 11 items are accepted for use as interview protocols to informants i.e. items 1 and 2 in the informant background as well as items 1,2,3,4,6,7,8 and 13. Although there are differences of opinion between experts on item 5 on the part of the ergonomic intervention, the item is still used in obtaining data from informants for interview sessions. Last 6 items were dropped i.e. items 3 and 4 on the informant background as well as item 9,10,11,12 for the ergonomic intervention section. In total only 11 items are applied to the interview protocol conducted to the informant with 10 items agreed on a basis, 1 item there is a difference of opinion between the expert as a whole and 6 items disagree and be dropped.
Table 1 showing the results of Cohen Kappa's reliability agreement. According to expert assessment for ergonomic intervention interviews. For this purpose, the researcher employs the services of two field experts who are assumed to be sufficient to see consent weighting as suggested by Cohen (1960). The assessment, found that the coefficient value (K) of 0.746 The value shows a good consensus level between experts 1 and 2 at the level of $5\%$ understanding. In addition, (Bogdan & Biklen 2003) Declaring supervisor verification is one of the forms of data reliability methods. The supervisor's verification can also help in terms of the regularity of the studies carried out. For this study, both the method of validity and reliability was implemented, namely through the calculation of the alpha coefficient of Cronbach and the review of the supervisor.
### c) Proposed for Implementation Ergonomic Interventions of Malaysia TVET Institutions
The findings of the interview from the informant, found that ergonomic interventions need to be comprehensive in addition to meeting the creteria as one of the leading indications for osh ergonomic interventions can be broken down into 3 phased clusters i.e. physical, organizational, and cognitive. This is in line with the framework that has been planned at the previous stage.
## i. Physical Ergonomic Interventions
This intervention specialises directly in the prevention of work-related MSDs, especially those at high risk of the neck, back and thighs. Among the ergonomic interventions that can be implemented are through the approach.
- Implementation of posture assessment
- Use of technology
- Workplace layout and conditional environment
Through the approach of implementing posture assessment in the early stages. Enabling students and citizens of TVET institutions involved in the commission of work to be detected or prevented before the occurrence of skeletal disorders (MSD) among the proposed instruments is the use of posture assessment when performing REBA work. The assessment of this posture is not just a data analysis but it will be able to provide a different point of view to the perpetrator by knowing the appropriate posture position while carrying out welding work. For the use of technology, the initial intention was to minimize the risks to the implementer including the use of appropriate self-protection devices such as gloves that are able to provide a comfortable grip, anti-tremor and grip perfectly. In addition, the design of the workplace should be suitable for the work performer, for example, it can be adjusted according to the height and suitable workspace and not too large to prevent the perpetrator from placing side workpieces and causing twisted body.
The layout of the workplace and the conducive environment refer directly to the terms of lighting, ventilation and noise sources. Appropriate lighting is able to help with good posture while performing the proposed lighting work for the workshop is around 300


lux according to the recommendations from DOSH in the 2008 workplace lighting guidelines. This is because the executor does not need to bend to carry out the work to see the results of the completed work. As is generally known the workshops are mostly hot works involving heat especially welding work therefore a good ventilation system is indispensable. The use of natural ventilation alone may not be sufficient to ensure that the fumes produced during the work of the welding are not sucked into the lungs. Therefore, the use of effective ventilation such as the use of LEV to trap fumes and fans for surrounding ventilation is very helpful. The last is noise related, basically the welding workplace will be designed by isolating between one welder and the other using a permanent or temporary barrier. The issue is that when there is noise, the noise reflecting onto the barrier can double and this can cause the noise to pass the threshold of 85dba. Therefore, the arrangement of welders in the workplace on a non-adjacent basis can reduce the risk of welders by imprisoning from noise sources. The use of sound soaking.
## ii. Organizational Ergonomic Interventions
Organizational ergonomic interventions are broken down into two levels of administrators and implementers. Slightly different from physical intervention, it is private in nature. But for organizational ergonomic interventions it is group in nature. Among the preventive measures or organizational interventions that can be implemented are;
- Early exposure of ergonomic education and training
- Management support for ergonomic interventions
- Management of skeletal risk during the implementation of work
Through the approach Early exposure of ergonomic education and training can provide new dement to the need for occupational disease prevention. The fact is that there are tvet institutions that are able to implement exposure as early as semester 1 of diploma studies through the application of OSH subjects. However, this initial exposure is theoretical learning only and does not succeed in integrating with physical training. Among the essences that should be present in such ergonomic education and training are ergonomic theory, good posture, effects and consequences of skeletal disorders of the body and most important is to self-assess the current state of sensation of body disorder. To support the concept of prevention, the executor should be able to obtain early exposure to education and to ergonomic interventions. When they know they will be conscious when they are aware that they will control and avoid the risk of self-awareness This is an important element to shape an individual's attitude. These social attitudes or values include effective aspects (feelings towards an object), behaviour (the tendency to act on behaviour).
Ergonomic intervention education and training should be carried out regularly. ini to ensure that they are able to change from attitude to culture. Referring to this pearl of the word "practice makes perfect" gives the impression that the exercises performed continuously will produce results that Perfect. The same goes for developing individual skills requires early exposure and continuous training to students to be better prepared with the realm of work. Efficacy research is also very important and needs to be carried out to prevent such matters from achieving objectives and not waste. a checklist of ergonomic interventions should be available to facilitate the evaluation and effectiveness of ergonomic interventions in line with this concept of plan, do, check and follow-up action (PDCA) because ergonomic interventions are dynamic and always need improvement.
Management support for ergonomic interventions is very significant in ensuring that ergonomic interventions are successful. The establishment of a policy of ergonomic intervention and safe work should be accelerated. With the existence of this intervention policy, it demonstrates management's commitment. It will be followed by the provision of provisions that support ergonomic interventions and the acquisition of supporting equipment to ergonomic intervene and bodily injury. Often the program in TVET institutions are zero exclusively for students only or for employees only or for management only. For ergonomic interventions it should be inclusive regardless of the person's background and level. This is due to occupational diseases not only towards students or employees but to all. Among the factors of the feasibility of ergonomic interventions is through physical and financial support from management.
The last for organizational intervention is the management of the risk of using the skeleton during the implementation of the work. The management can implement the work implementation schedule by applying the concept of micro breaks, or the frequency of every 10 minutes of work will be given a short break of about 30 seconds. This break refers to a passive state (no activity) nor active rest (a combination of rest with stretching or light exercise). Not least the start of a working session with a meting toolbox as well as exercise activities and brief stretching to prepare the body physically and mentally to perform the task. In addition, the distribution of hand bills or pocket-sized safe work leaflets is capable of self-warning. Changes from SOP standard operating procedure to safe operating procedure are also preventive measures or ergonomic risk mitigation measures.
Generally, when an organization achieves a level of self-awareness, it will indirectly stimulate the culture of ergonomic interventions.
## iii. Cognitive Ergonomic Interventions
The last ergonomic intervention is a congenital ergonomic intervention. It is the best of these interventions, this because this intervention involves the whole institution. Not just the management or the employees or the students. It is collective and comprehensive, between ang contained in the cognitive ergonomic intervention is to establishment of a culture of intervention.
Applying a culture of intersensitivity and safe work is not easy. In general, basic and mid-level interventions i.e. physical and organizational ergonomic interventions should be achieved in whole or in part. The establishment of specialized officers who manage OSH matters, especially occupational diseases such as MSD disorder problems, are also among the factors that are seen to be a catalyst for the culture of the intervention. Many workplaces only chant a culture of safe work but when it comes to occupational diseases no one takes care or even takes indifferent action. Apart from that recognition is also able to help the culture of intervention bloom in TVET institutions. In contrast to the approach by always showing tvet citizens with punishment is better approach positively through internally and externally implemented. There have been many organizations that have implemented the recognition of OSH such as the government through national council for occupational safety and health (NCOSH) and department of occupational safety and health (DOSH) as well as non-governmental organizations such as the MALAYSIAN SOCIETY FOR OCCUPATIONAL SAFETY & HEALTH (MSOSH) association. Evaluation of occupational diseases such as skeletal gagging (MSD) problems at the end of the study should be carried out in order to ensure that the workforce produced by TVET institutions is certified healthy and able to enter the job market. Therefore, students are not only provided with academic transcripts, but occupational disease-free testimonials can also be included. Creating a holistic occupational disease reference center for TVET institutions is also capable of enhancing the image of TVET institutions. This reference center is not just to store data on occupational diseases but to be a training center for the same use in different TVET institutions of the ministry to raise awareness of occupational diseases especially in ergonomic issues, regardless of the development of the syllabus, selection of workplace design and the implementation of ergonomic interventions. The operation of this reference center can be with the industry in achieving the reduction of occupational diseases in the future.
## IV. RESULT
### a) Intervention Framework Recommendations
The findings of ergonomic interventions in practical work in TVET institutions can be formulated in Figure 3 as follows:
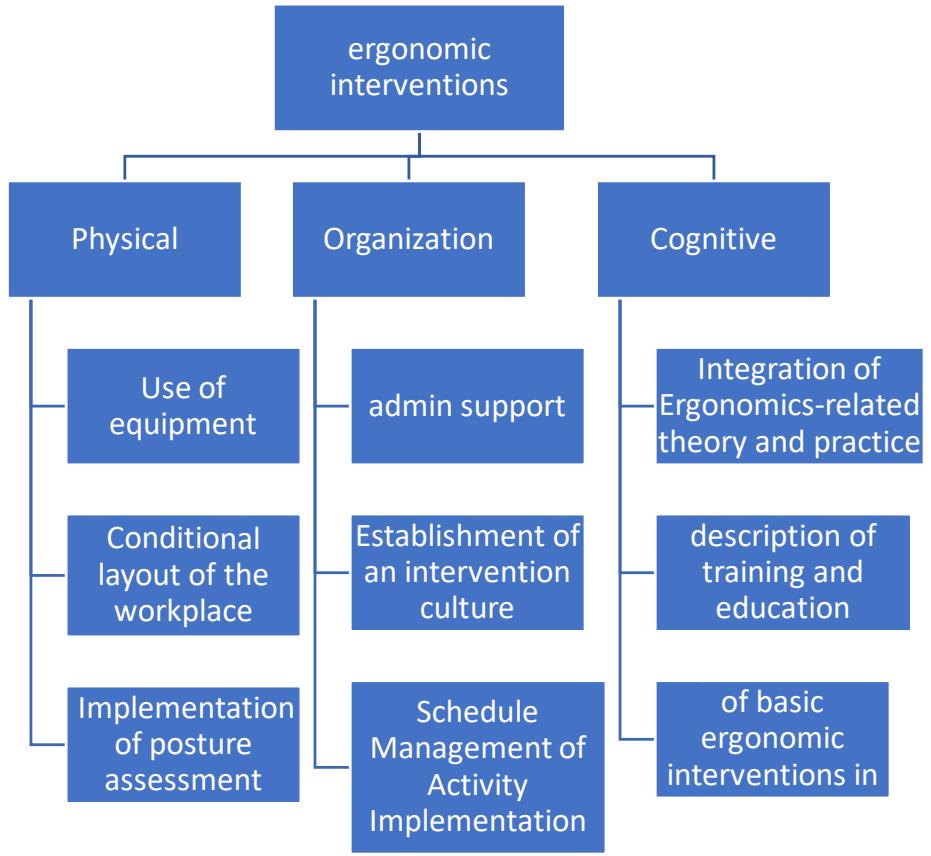
Figure 2: Recommendations Framework of ergonomic interventions

Generally, ergonomic interventions can be attributed to 3 large clusters by including physical, organizational and cognitive interventions. This ergonomic intervention also represents certain levels of level 1 physical ergonomics i.e. basic, moderate-level level organizational ergonomic interventions and high level 3 organizational interventions.
## V. CONCLUSION
In order to create a comprehensive intervention program, it is necessary to fill it with all three clusters. However, it is given a level due to the difficulty and impact of the implementation on the organization. For example, a physical ergonomic intervention at a basic level focuses only on the perpetrator but the impact is only on one sub-unit within the institution. The most difficult the implementation method but the easier it is to see the overall change, very importantly if an institution only implements a basic ergonomic intervention, it does not mean that it does not carry out the intervention activity but it is not enough and it is best to start with the basic level and be followed up with the next level to get a good intervention effectiveness.
The implementation of this ergonomic intervention is not mandatory. Must be implemented as a whole but it should be implemented according to the suitability of the place. It is in line with the implementation of ergonomic guidelines in the workplace in the Occupational Safety and Health Act 1994 on a voluntary basis. Perhaps sometime these guidelines will be made mandatory.
Generating HTML Viewer...
References
17 Cites in Article
Candi Ashley,Christina Luecke,Skai Schwartz,Maeen Islam,Thomas Bernard (2008). Heat strain at the critical WBGT and the effects of gender, clothing and metabolic rate.
N Abarghouei,H Nasab (2012). An ergonomic evaluation and intervention model: Macro ergonomic approach.
H Baydur,Y Demiral (2016). Effects of participatory ergonomic intervention on the development of upper extremity musculoskeletal disorders and disability in office employees using a computer.
R Bogdan,S Biklen (2003). Qualitative Research for Education.
J Cohen (1977). Statistical Power Analysis for the Behavioural Sciences.
Philip Harvey (2019). Domains of cognition and their assessment.
Hal Hendrick (2000). The technology of ergonomics.
H Hosseini,N Abarghouei,H Nasab (2012). An ergonomic evaluation and intervention model: Macro ergonomic approach.
A Imada (2007). Meeting Diversity in Ergonomics.
N Jaffar,A Abdul-Tharim,I Mohd-Kamar,N Lop (2011). A Literature Review of Ergonomics Risk Factors in Construction Industry.
S Kalpakjian,S Schmid (2009). Manufacturing Engineering And Technology Sixth Edition In SI Units.
Gerald Midgley (2020). Science as Systemic Intervention: Some Implications of Systems Thinking and Complexity for the Philosophy of Science.
P Tittiranonda,D Rempel,T Armstrong,S Burastero (1999). Effect of four computer keyboards in computer users with upper extremity musculoskeletal disorders.
T Waters,R Dick (2015). Evidence of health risks associated with prolonged standing at work and intervention effectiveness.
J Wendsche,A Lohmann-Haislah (2016). The impact of supplementary short rest breaks on task performance -A meta-analysis.
Y Xie,G Szeto,J Dai,P Madeleine (2016). A comparison of muscle activity in using touchscreen smartphone among young people with and without chronic neck-shoulder pain.
Nurulfajar Manap,Azma Putra,Zakiah Halim,Anis Zain (2024). Enhancing Personalized Learning in Engineering Education through TUAH Digital Portfolio: A Framework for Equitable TVET in Malaysia.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Khairul Fahzan bin Salleh. 2026. \u201cAn Intervention Ergonomic Framework for Malaysia TVET Higher Education\u201d. Global Journal of Research in Engineering - G: Industrial Engineering GJRE-G Volume 24 (GJRE Volume 24 Issue G1): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Fundamentally an intervention refers to an action that has an agenda and is aimed by the human being to create change (Midgley 2020) according to him if the intervention is an action aimed by the human being to create change, then systemic intervention is an action aimed at creating a change in the context of reflection to the system. The International Association of ergonomics (IEA) categorizes ergonomics into three specific domains: physical, organizational, and cognitive ergonomics. The physical domain is concerned with human anatomy, anthropometry, physiological and biomechanical characteristics associated with physical activity. The domain also consists of working environments and equipment, such as hand tools, workstations and lighting and ventilation in the workplace. The domain of the organization, referring to the concern for the optimization of work systems, including organizing and even work processes for example as a frequency of work, work cycle and rest, in addition to directing in performing work. The cognitive domain is related to mental processes, such as perception, memory, judgment, and motor response.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.