
I. BACKGROUND
Maternal mortality and morbidity are high in sub-Saharan Africa due to complications from microbial infections[1]. Managing of complications related to these infections during pregnancy requires the prescription of many drugs, including antibiotics. The best use of antibiotics to treat infectious diseases during the antenatal visits, in addition to iron administration and dietary supplements, could reduce maternal and baby mortality during pregnancy[2]. Reports suggest that antibiotics account for nearly of all prescription medications during pregnancy, and approximately of women receive an antibiotic during pregnancy [3-5]. Poor management of antibiotics is one of the leading causes of antibiotic resistance in microbial agents [6]. The use and choice of antibiotics during pregnancy depends on health resources, nutrition status, mode of delivery, and socio-economic factors. A better knowledge of the pharmacokinetics, potential toxicity, and teratogenic risks of these drugs is essential to optimize the efficacy and safety of antibiotic treatment [7]. The pharmacokinetics of antibiotics during pregnancy can be affected by multiple factors, including absorption, distribution, metabolism, and elimination [8]. Some antibiotics can potentially to affect embryo-fetal development at different stages of pregnancy. Teratogenic effects occur mainly during the embryonic period (first trimester of pregnancy) [9]. Prescribing in pregnancy always raises the issue of drug risks to the embryo or fetus, an additional pharmacokinetic compartment related to transplacental drug distribution. The use of medications during pregnancy is a significant concern for patients and prescribers. The incidence of thalidomide in the 1960s and the teratogenic effects discovered in 1971 with diethylstilbestrol are some examples of the hazards that prescription drugs may pose to pregnant patients [10, 11]. Pregnancy is associated with changes in the physiological, psychological, and psychosocial aspects of a woman life. Antibiotics are among the more frequently prescribed medicines in pregnant women, and the use of antibiotics is increasing. However, with limited studies available in this population, the safe use of antibiotics in pregnancy remains a concern.
The Food and Drug Administration (FDA) categorization of drugs based on their risk of pregnancy should be considered before prescribing a medication to pregnant women. The health center receives pregnant women for prenatal consultations and various types of care.
No study on antibiotics prescribed in pregnant women and their compliance with the FDA classification on drug safety during pregnancy has been done in this village. This study will contribute to the improvement of antibiotic prescription in pregnant women.
II. METHODS
The study was carried out in the district health centers of Kangaba, a malaria-endemic area located 80 km southwest of Bamako. A cross-sectional study was carried out from January to March 2021 to collect data on the use and prescription of antibiotics during the antenatal visits. The sampling consisted of all prescriptions for pregnant women with at least one antibiotic drug and recorded in a registry. The nature of the antibiotic drugs, the dosage, the duration of treatment, and the type of prescribed antibiotic combination were analyzed based on the FDA classification guidelines. A non-compliant prescription was defined as any breach of one or more of the parameters listed above concerning, to the FDA classification guidelines. In the registries, we also collected information about the socio-demographic characteristics (age and sex of the patient). In addition, a report form was administered to all prescriber's Data focusing on their professional qualification and their level of knowledge of the FDA classification.
FDA classification of drug safety in pregnancy[12]
- Category A: No adverse effects in human pregnancies. Safety established using well controlled human studies.
- Category B: Presumed safety in human pregnancies. Limited human studies/no adverse effects in animal studies.
- Category C: Uncertain safety: Limited human studies/adverse effects in animal studies.
- Category D: Adverse effects in pregnancies. Benefits may outweigh associated risks.
- Category X: Adverse effects in pregnancies. Risks outweigh possible benefit.
Anti-Microbials: D and X FDA drug categories[12]
- Category D: Aminoglycosides: Gentamycin, Streptomycin, Tobramycin, Tetracyclines, Doxycycline, Minocycline, Tetracycline, Voriconazole, Chloramphenicol, Antimycotics (Amphotericin B, 5-flucytosine, Griseofulvin).
- Category X: Quinine, Thalidomide, Ribavirin, Miltefosine, oral contraceptives, statins.
III. STATISTICAL ANALYSIS
Data were collected on a report form, entered into Excel, and analyzed using the statistical software Epi info 6.04.
a) Ethical considerations
Our study protocol was approved by the ethics committee of the Faculty of Medicine and Odontostomatology, and Pharmacy of the University of Sciences, Techniques, and Technologies of Bamako (USTTB). The health and administrative authorities of Kangaba were informed before the beginning of data collection.
The information found in the logs was kept entirely confidential and was not disclosed to anyone outside the study investigators. The personal information concerning each pregnant woman was coded. Only the principal investigator could identify the patients during the data analysis for publication of the results.
IV. RESULTS
| Antibiotics | Age of the pregnancy | Total n (%) | ||
| First Trimester N (%) | Second trimester N (%) | Third Trimester N (%) | ||
| Amoxicillin | 225(36.6) | 0(0) | 0(0) | 225(15) |
| Erythromycin | 195(31.7) | 355(54.9) | 95(40.1) | 645(43) |
| Azithromycin | 96(15.6) | 193(29.8) | 49(20.7) | 338(22.5) |
| Metronidazole | 28(4.6) | 64(9.9) | 70(29.5) | 162(10.8) |
| Ciprofloxacin | 11(1.9) | 19(2.9) | 16(6.8) | 46(3.1) |
| Doxycycline | 0(0) | 12(1.9) | 7(2.9) | 19(1.3) |
| Cefixime | 4(0.7) | 0(0) | 0(0) | 4(0.3) |
| Gentamycin | 53(8.6) | 0(0) | 0(0) | 53(3.5) |
| Lincomycin | 2(0.3) | 0(0) | 0(0) | 2(0.1) |
| Ceftriaxone | 1(0.2) | 0(0) | 0(0) | 1(0.1) |
| Associated | 0(0) | 4(0.6) | 0(0) | 4(0.3) |
| Total | 615(100) | 647(100) | 237(100) | 1499(100) |
| Therapeutic class of antibiotics | Age of the pregnancy | Total n (%) | ||
| First trimester N (%) | Second trimester N (%) | Third trimester N (%) | ||
| Aminosides | 53(8.6) | 0(0) | 0(0) | 53(3.5) |
| Bêta-lactamines | 226(36.7) | 0(0) | 0(0) | 226(15.1) |
| Céphalosporines | 4(0.7) | 0(0) | 0(0) | 4(0.3) |
| Lincosamides | 2(0.3) | 0(0) | 0(0) | 2(0.13) |
| Macrolides | 291(47.3) | 550(85) | 144(60.8) | 985(65.7) |
| Macrolides+bêta-lactamines | 0(0) | 1(0.2) | 0(0) | 1(0.06) |
| Macrolides+ Fusidanines | 0(0) | 1(0.2) | 0(0) | 1(0.06) |
| Macrolides+ Nitroimidazoles | 0(0) | 1(0.2) | 0(0) | 1(0.06) |
| Nitroimidazoles | 28(4.6) | 63(9.7) | 70(29.5) | 161(10.7) |
| Quinolones | 11(1.8) | 19(2.9) | 16(6.8) | 46(3) |
| Téttracyclines | 0(0) | 12(1.8) | 7(2.9) | 19(1.39) |
| Total | 615(100) | 647(100) | 237(100) | 1499(100) |
| Variables | Category | (%) |
| Dosage of antibiotic in mg | <500mg | 77(5.1) |
| 500mg | 1419(94.7) | |
| 1000mg | 3(0.2) | |
| >1000mg | 0 | |
| Daily frequency of antibiotic use | Once | 65(4.3) |
| Twice | 1216(81.2) | |
| Thrice | 13(0.9) | |
| Four times | 205(13.7) | |
| Forms of antibiotics | Tablet | 1450(96.7) |
| Injection | 49(3.3) | |
| Duration of treatment | <7days | 1487(99.2) |
| 7days | 10(0.7) | |
| >7days | 1(0.1) |
| Drug/ FDA recommendation | Age of the pregnancy | ||
| 1sttrimester | 2ndtrimester | 3rdtrimester | |
| FDA recommended | Amoxicillin, Erythromycin, Azithromycin, Metronidazole, Ceftriaxone, Cefixime | Erythromycin, Azithromycin, Metronidazole, Ciprofloxacin | Erythromycin, Azithromycin, Metronidazole, Ciprofloxacin |
| Not FDA recommended | Ciprofloxacin, Gentamycin, Lincomycin | Doxycycline | Doxycycline |
V. DISCUSSION
Most pregnant women are exposed to some type of medication during pregnancy. Drugs prescribed during pregnancy can exercise a teratogenic effect on fetuses, and those prescribed during breastfeeding can also impact on infant health. Antibiotics are among the more frequently prescribed types of medications during pregnancy and lactation [13].
The risk of antibiotic exposure was highest in the first and second trimesters but lowered in the third trimester. Mensah et al. 2017 in Ghana found that the risk of antibiotic exposure was highest in the last trimester. This is reassuring because the acquisition of specific fetal immunity begins in the third trimester, and is highly dependent on the microbiome, which can be altered by antibiotics [14].
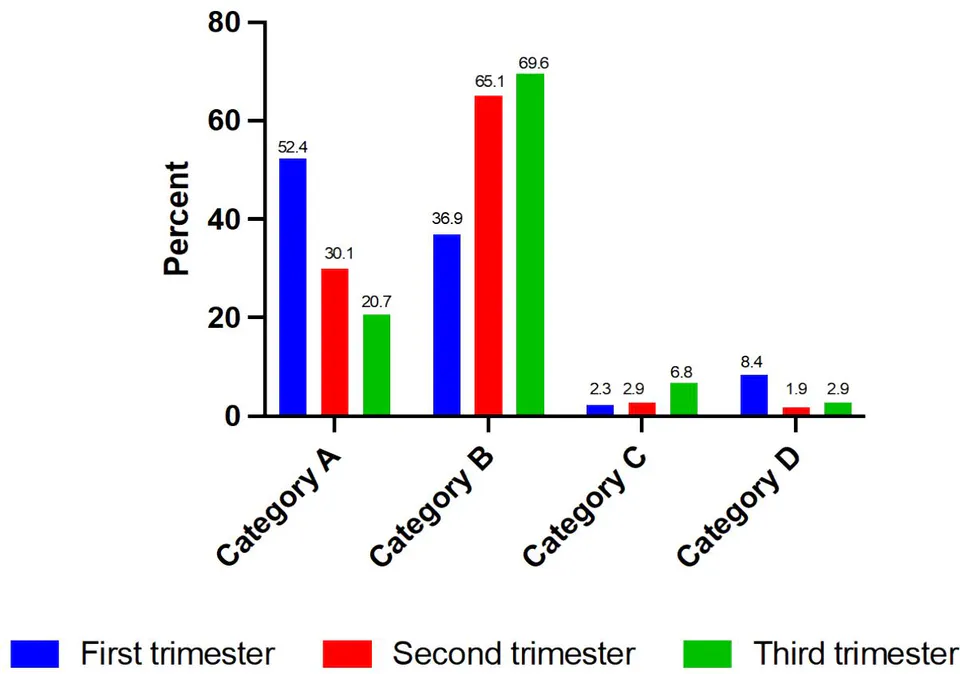
Amoxicillin (category A) at , erythromycin (category B) at , and azithromycin (category A) at , were the mainlydrugs prescribed during the first trimester of pregnancy (Table 1). Erythromycin (category B) at , azithromycin (category A) at , and metronidazole (category B) at , were the mainly drugs prescribed during the second trimesters (Table 1). In the third trimesters, erythromycin (category B) at , metronidazole (category B) at , and azithromycin (category A) at , were the mainly drugs prescribed (Table 1). A study carried out in northern Nigeria by Ogboma et al. in 2019 reported that ciprofloxacin and erythromycin were the mainly drugs prescribed during pregnancy[15].
In Kangaba health center, macrolides were the most prescribed antibioticsat , followed by beta-lactamsat , and nitroimidazoleat . Ogboma et al. in 2019 in Nigeria, and Elizabeth C. Ailes et al. in 2018 in the USA reported that fluoroquinolones were the most prescribed class in pregnant women with and , respectively [15, 16]. A study carried out in Ghana between 2011 and 215 by Mensah et al. reported that of prescriptions for antibiotics in pregnant women were beta-lactams [14].
Prescribing macrolides during pregnancy is common, as similar results have been reported in the literature[17-20]. The use of macrolides in pregnancy is, however, a growing concern [18]. Significantly, a recent study by Fan et al. followed 104,605 children from birth to 14 years old, and it was concluded that prescribing macrolides in any trimester was associated with an increased risk of genital malformation [18]. Whereas a previous cohort of 1,033 women exposed to macrolides (erythromycin, azithromycin, clarithromycin or roxithromycin) reported that there was no association between this drug and the development of significant abnormalities in the fetus [17].
The dosage in mg of most drugs prescribed was 500mg with regardless of the age of pregnancy. This result is similar to that observed by Ogboma et al. in 2019 in Nigeria [15]. The dosage frequency per day of most drugs prescribed was twice with . The most common route of administration was oral with, . The dosage form of most prescribed drug was tablet . The duration of treatment in most of the prescriptions was less than one week . This does not appear to be in line with the management of antibiotic resistance, where a minimum of seven days and a maximum of twenty-one days is recommended to avoid resistance that could result from incomplete treatment. The duration of treatment depends mainly on the nature of the disease, the severity, the presentation of the drug (dosage in mg and dosage form), the age of the pregnancy, and the pharmacokinetic of medicarion.
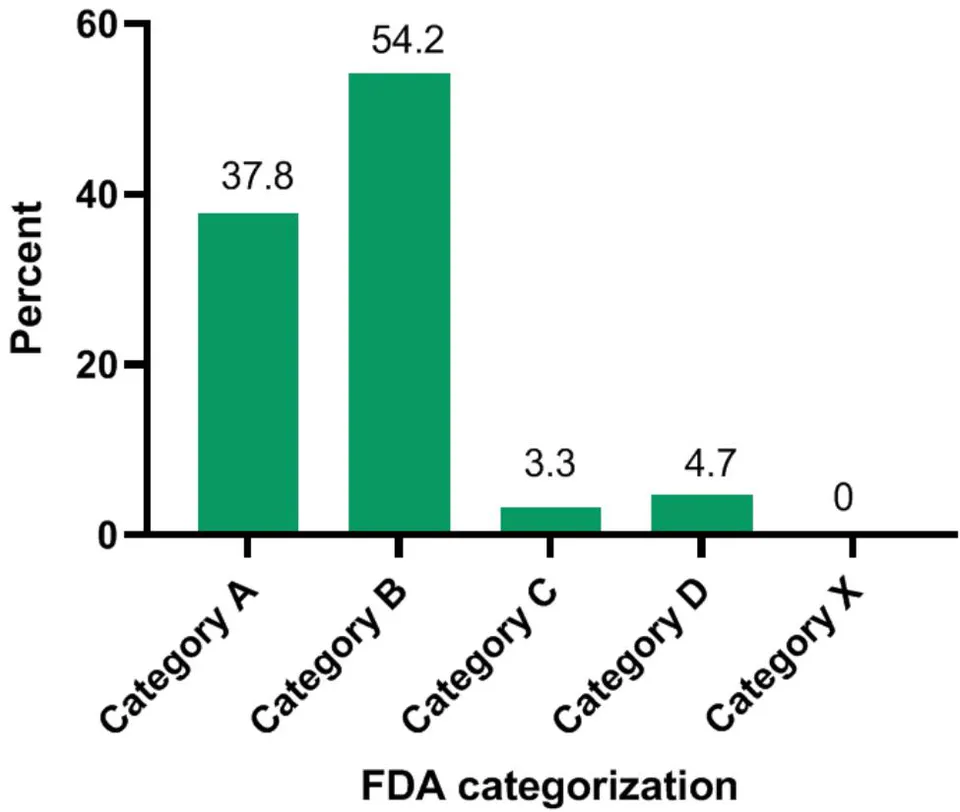
Most drugs fell into category B at , and category A at . Mensah et al. 2017 in Ghana reported that most of the antibiotics prescribed were of category B at , followed by C and D at and , respectively [14]. Drugs in categories C and D are toxic to the fetus but can be used during pregnancy if the benefits to the mother outweigh the risks to the fetus.
The prescription of, ciprofloxacin (1.85%), gentamycin (8.6%) and, lincomycin (0.3%) in the first trimester of pregnancy does not conform to FDA recommendations. According to the FDA, ciprofloxacin, gentamycin, and lincomycin should be prescribed in the second and third trimesters of pregnancy due to their potential embryotoxicity.
The prescription of, doxycycline (Category D) in second and third trimesters of pregnancy is not recommended by FDA, because doxycycline is toxic on the fetus.
VI. CONCLUSION
The antibiotics prescribed for pregnant women fell within the FDA risk categories A and B, with rare cases of prescription occurring in categories C and D. The most frequently prescribed antibiotic in Kangaba was the macrolides.
Singles
FDA: Food and Drug Administration
MRTC: Malaria Research, and Training Center
USTTB: University of Sciences, Techniques, and Technologies of Bamako
Contribution
Karim Traore, Seidina Diakite, Sekou Bah, and Mahamadou Diakite participated in the conception and design of the manuscript. Karim Traore, Bourama Keita, Sory I Diawara, and Drissa Konaté performed the statistical analysis, and Karim Traore Mahamadou Ballo, Modibo Sangaré drafted the manuscript. All authors read, and approved the final version of the manuscript.
Funding
Authors did not get funding for this project. Authors paid for the cost the project.
Conflict of interest: None
ACKNOWLEDGMENTS
We sincerely thank the communities of Kangaba; we thank the technicians, clinicians, and the nursing staff for their assistance. We are grateful to many colleagues at the Malaria Research, and Training Center (MRTC) for providing critical reviews of the manuscript.