## I. INTRODUCTION
Among the most common diseases that can occur gestational diabetes is found during pregnancy. Is characterized due to hyperglycemia with values that, despite being higher than normal, are lower than those established to diagnose diabetes. This type diabetes usually occurs after 20 weeks of gestation (World Health Organization, 2020; Palani et al., 2014).
The definition postulated by the International Classification of Diseases in his $10^{\text{th}}$ edition categorizes this condition in the section "maternal diseases that can affect the fetus" with the code "O24 Diabetes Mellitus in pregnancy". And it is defined as "an alteration in the metabolism of carbohydrates, which is diagnosed for the first time during the state of pregnancy. It is a condition of insulin resistance, generally presents after the fifth month of gestation" (ICD-10, 2008, p.245).
It's necessary take into account that in gestational diabetes symptoms occasionally are not evident. However, they could present some because of high blood sugar levels. These include that patients may be thirstier than usual more frequent and heavier urination or feeling very tired or fatigued (Martínez de Salinas 2017; Gracia & Olmedo, 2017).
Some other effects associated with impaired glucose recorded in various investigations are: visual disturbances, excessive hunger, headache, headache, stomach aches, disorientation, difficulty concentrating and lethargy (American Diabetes Association, 2002). It's essential that pregnant women undergo the pertinent examinations, which should be carried out around the fifth month of pregnancy a blood glucose test to identify the pathology in time (González Ruiz et al., 2014).
Researchers have been able to point out a large number of complications that arise in pregnant women diagnosed with GDM such as increased risks for fetal abnormalities including macrosomia, neonatal hypoglycemia, respiratory distress syndrome, alteration in the development of the islet cells and malformations in the development (Reyes Burgos & Guillén Matos 2015; Crowther et al., 2005).
Concomitant to this medical symptomatology, there are some factors that could have a psychological impact and affect the quality of life of women with gestational diabetes, which can even be more serious than the pathology itself. Some of them would be associated with the severity and intensity of self-care tasks, the interference of these tasks in daily life, fear of complications and symptoms of hyperglycemia that can affect psychosocial and occupational functioning (Rubin, 2000; Craig, et al., 2020; Jones, Roche & Appel 2009).
Therefore, it is possible that, once the disease has been identified, the patients experience certain impediments in complying with the medical prescriptions, which are almost always associated with the lack of education and with skills in the management of the pathology.
According to what has been pointed out by various researchers, variables related to the complexity of the treatment (because it is clear that long periods of time to recover from this condition), together with the lack of visible immediate reinforcements, (because the effects of prevention will really be seen in the long term), can make the diagnosis of GDM and its condition a heavy burden for patients (Gatchel, Oordt & Oordt, 2003; Sacks 2014).
Several authors affirm that the lack of effective communication with the health professionals and the costs to be incurred by patients and their families to deal with the problem also hinder the success of medical interventions (Lakshmi et al., 2018).
It is important to mention that not all pregnant women have the same risk of GDM. The evidence shows that there are some factors that lead and can produce it, such as high levels of blood glucose, family history of diabetes, overweight before pregnancy or weight gain during this period, present syndrome of polycystic ovary, excessive amniotic fluid, unexplained miscarriage or stillbirth, high blood pressure, lead a sedentary lifestyle, be over 25 when you get pregnant, and having had a previous diagnosis of diabetes (ADA, 2011; Cartin, 2011).
Therefore, it is necessary to emphasize the importance of the psychoeducation of these women so that they can acquire habits and lifestyles. such as eating healthy foods, reducing fat, reduce sugar intake, avoid drug and alcohol use, exercise regularly, sufficient and adequate controls doctors, and even understand some references of the complications that can happen in pregnancy, including the presence of GDM.
It is opportune to have information that lets the woman know that she is condition is a public health problem of great relevance and that, if not If treated quickly, it can cause various alterations to the mother and the baby.
Delving into the psychological dimension that has been considered in paragraphs previous ones, it could be said that the literature and the evidence scientific report in relation to GDM. For example, various authors recorded the appearance of depressive symptoms during and after this type of diagnosis
(Antos, Nowak, & Olszewski, 2013; Diaz, et al., 2013; Dame, et al., 2017).
But in the same way there is evidence related to the presence of anxiety, stress, low self-esteem, feelings of guilt, difficulties in feeding, insomnia (Tellería, 2014; Hinkle, et al., 2016). I also know have pointed out alterations or dysfunctionalities in the social plane such as isolation, decreased communication with friends and family, difficulties with the couple, decreased function and sexual appetite, among others.
As has been seen, a significant number of investigations have been carried out on this topic that can be framed within the psychosocial perspective of GDM. Particularly in the systematic review carried out by Devsam, Bogossian & Peacock, (2013), in which 19 studies were identified who met the inclusion criteria.
Three fundamental categories stand out in this work: a) reaction initial diagnosis, in which negative thoughts are observed, feelings of loss of control, identity changes and adaptation the changes; b) concern approach, in which there is evidence of concerns about the health of the baby and the perceived severity of the DMG. Finally, category c) influencing factors is recorded, which includes cultural roles and beliefs, social stigmas, social support, support professional, adequate and appropriate information, social roles and barriers for self-care.
In any case, the results of this systematic review highlight the importance of the psychosocial considerations presents in this type of patients, among which we can mention: the psychological impact of the diagnosis, the importance of overcoming anxiety and stress to achieve better adherence to treatment, the necessary adaptation in the patient's relationship with family and health personnel, need to reduce the negative charge, both cognitively and affective, that have people who have been diagnosed with GDM, among other.
Of all these psychosocial considerations, one in particular has generated the interest of this investigative group that are the beliefs and attitudes of women diagnosed with GDM. And that is, if it can be found a dimension that leads to generate some kind of model to help the women with GDM, it would be represented by the set of cognitions, attitudes and representations that at one moment a woman has to whom diagnosis was made during pregnancy.
Around this theme there are important approximations, such as the research developed by Chávez-Courtois, et al., (2013), in which it is observed how the cognitive structure of women with GDM presents symptoms such as confusion; despair and recurring ideas; records of thoughts of the type: "my son is going to come with malformations", "I am going to die", "my son is not going to come into the world", "this pathology is irreversible", "why did it happen to me".
There is also evidence of a flow of beliefs in relationship with guilt and low self-esteem.
Despite how unflattering the previous results are, the knowledge of these beliefs, attitudes and social representations of women with GDM, can be an important input in the adequacy of guides and guidelines for the psychosocial accompaniment of women with this diagnosis, which incidentally, at least in the Latin American context, are quite scarce, reducing, in the cases in which they exist, to guides of a medical care type, ignoring the transcendent of both social and psychological variables, not only in the appearance of pathology, but in its management.
It is clear then that knowledge of beliefs, cognitions and attitudes of women with GDM, will allow progress in aspects as crucial as helping patients to adhere to treatment, generate psychoeducational models, understand the pathology and its treatment and even involve the family group and the couple in managing not only the pathology, but throughout the pregnancy process. For this reason, it is presented this research that has the purpose of carrying out a systematic review around the cognitions and beliefs present in women with gestational diabetes mellitus.
## II. MATERIALS AND METHODS
- Design and type of study: This is a systematic review carried out with the methodology of the Cochrane Collaboration (Higgins and Green, 2011) and the PRISMA statement and checklist (Moher, Liberati, Tetzlaff, and Altman, 2010).
- Search strategy: Inquiries were made in the databases of Pubmed, Scielo, Hindawi, Springer Link and BMC Medicine data, in order to identify scientific articles in English and Spanish from 2000 to 2021. The exploration was limited to the last two decades due to the interest that the scientific community has presented in the psychosocial factors associated with the GDM (Jiménez-Chafey and Dávila, 2007). Also made supplementary manual searches and retrieved the articles that met the inclusion criteria. Descriptors were used using booleans that included DMG and beliefs, attitudes and cognitions.
- Inclusion Criteria: Studies with female participants over 18 years of age (assured in one way or another by the presence of a consolidated belief system) diagnosed with GDM. Studies on the belief system, cognitions, attitudes, frames of reference and social representations. In addition, observational studies were included.
- Exclusion Criteria: Studies with samples of women under 18 years old. Likewise, studies belonging to gray literature, studies reviewed in blogs or web pages of public or private institutions.
- Selection of studies: It is presented in the PRISMA flowchart described in Figure 1. Of the 85 preselected articles, it was read the full text to arrive at a final selection that included 28 articles.
- Data extraction and analysis: A matrix was constructed that included the consulted database, article title, author, keywords, methodology, results, conclusions. Additionally, a review was constructed for each of the research included in this review. These are the supplies principles for the analysis of the results and the conclusions of this study.
## III. RESULTS
Of the 28 articles selected to be included in this systematic review (Figure 1), the most important results are indicated below.
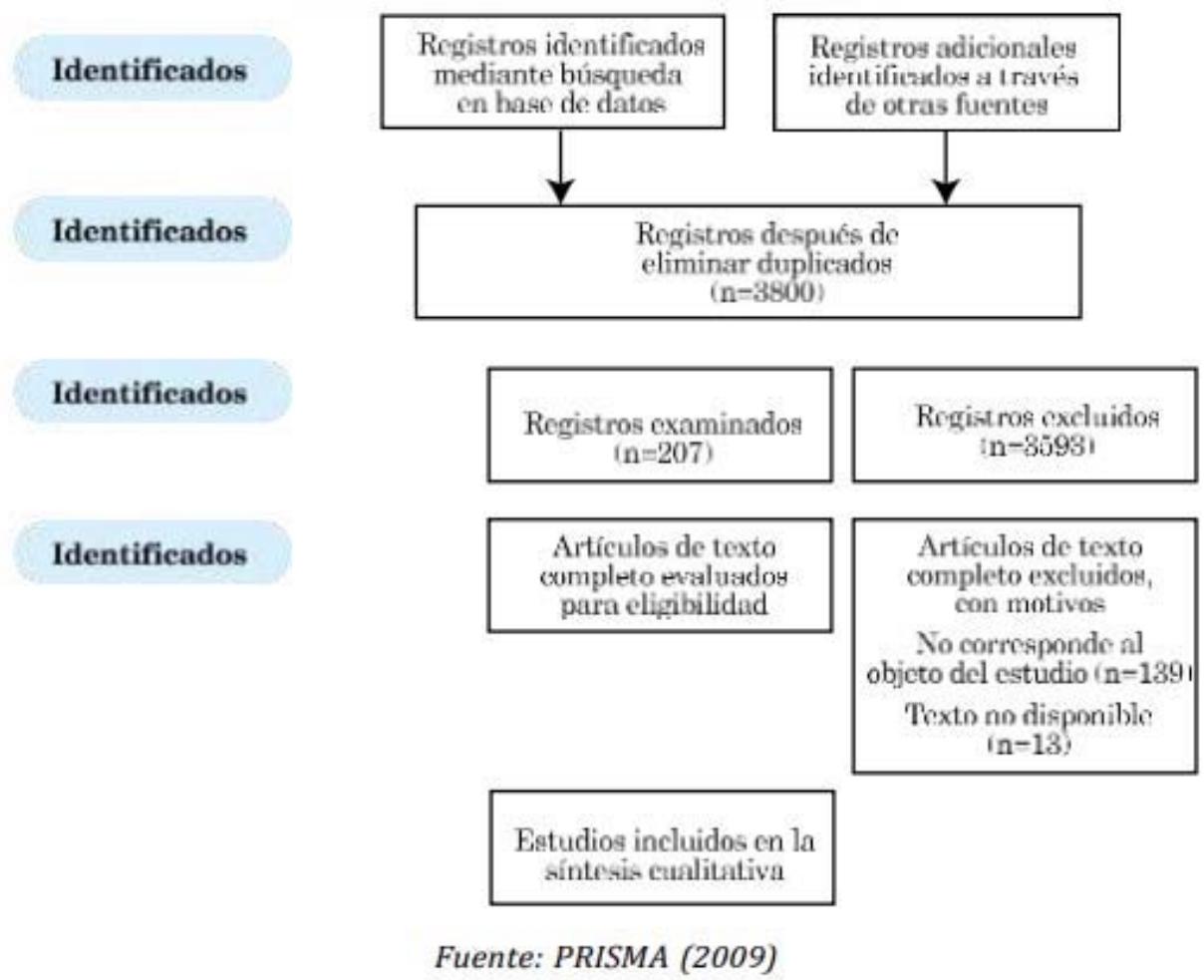 Figura 1: Diagrama de flujo PRISMA 2009
A first element in the beliefs of women with GDM is related to with what happens after diagnosis. On a recurring basis the Patients state that they experience a stress condition in which a significant number of cognitions associated with impairment arise of the future health, not only of them, but of the unborn babies.
They experience GDM as a burden and a threat to the baby-mother dyad (Razee et al., 2010; Tellería 2014; Dalfrà et al., 2011). On the other hand, many of the women may have the belief that GDM will lead to in chronic diabetes that they will suffer from for the rest of their lives. It is important to highlight that many of the beliefs, including the fears that may arise derive from the information provided by the hospital institution and health personnel (Hjelm et al., 2008; Hjelm et al., 2018).
The investigative group of Dalfrà and collaborators (2011), also investigated in their works some psychosocial variables such as depression and certain cognitions. These studies were conducted in both women with GDM, such as in patients with type II diabetes. It was possible to establish that These patients generally present depressive symptoms, which are closely related to a perception of poor health.
The issue for women is complicated if they have other children who are younger than they depend on them. Some have support from their extended family, but others they must leave their children with people who are not their family. Only with the purpose of offering a reference is the testimony of a woman diagnosed with GDM: "I was suddenly hospitalized with diabetes and I couldn't get some belongings home before I was hospitalized" (Araujo et al., 2013).
On the other hand, Chávez-Courtois et al., (2014) who approached the system of beliefs, perception and experiences of women with DMG, report valuable findings. Several of the women with this condition are very certain that, although it is a delicate pathology, the self-care practices, physical exercise, diet and, in general, medical recommendations, will augur good results in overcoming the diabetes. The women interviewed for this research generally they are quite clear about the risks and lifestyles that are not healthy that can lead to the generation of GDM.
Among the most significant answers that can be considered are: "I feel that the disease has to do with eating food with a lot of sugar, or eating late. Also, I hardly ever ate breakfast. I have generally had bad eating habits". In other cases, there are thoughts of these women, around the fact that it is a hereditary condition. And in several cases patients feel guilty for not having healthy habits before and during pregnancy.
In fact, in the study by Hjelm et al., (2018), the influence of these psychosocial variables. African migrant women residing in Sweden were compared with women from the European country where both groups were diagnosed with GDM. It was found that women from Africa did not know what GDM was and its causes and how consequently they had a passive attitude of self-care. Coincidentally you are patients reported more pregnancy-related problems. In contrast, Swedish women had higher risk awareness, higher concern for your health and that of your baby and therefore more self-care, including the use of medications.
The importance of culture is also evidenced in the research carried out in an Asian context by Ge, et al., (2016), in which It seems that a diagnosis of GDM does not cause major concerns, as it could be in western countries. Some of the women with these types of diagnoses just let nature take its course and they rely a lot on the type of food they consume. Thoughts regarding this condition are not as negative and generally believe will have a good prognosis, which makes the emotional and family effect don't be so dramatic.
In the meta-analysis by Chida & Hamer (2008), in which they wanted to establish the incidence of adverse psychosocial factors with poor control of diabetes, statistically significant associations were found. This was determined through pooled correlation coefficients $r = 0.096$, $p = 0.006$. In the same sense, the lack of social support also contributes to poor control of diabetes.
In the study carried out by Ansarzadeh et al., (2020), in which negative correlations between quality of life and the presence of GDM that reach -0.78, a positive correlation was found between the results obtained by the participants in the scale of knowledge, attitudes and self-care and the results obtained in social support.
Patients with GDM who have the perception that they have with high levels of social support and a high level of knowledge of the pathology, tend to have positive attitudes towards their condition and generally high levels of self-care. On the other hand, the research shows that the presence of levels of anguish is correlated negatively with self-management. That is, before levels of anguish, little can the person do to contribute from their own management to leave forward in the pathology suffered. In this case the correlation is reported in -0.857. There is also a positive correlation between the level of knowledge and self-management, equivalent to 0.848.
On the other hand, Park et al., (2018), start from the assumption that breastfeeding affects positively in the metabolic regulation of women with GDM, also favoring that these pregnant patients decrease the probability of developing type II diabetes after pregnancy (Kelishadi & Farajyan, 2014; Brahm & Valdés, 2017).
As has been recorded through these results, from various perspectives that articulate the research and theoretical interests of health and disease with the social sciences, we wanted to find the incidence of psychosocial variables such as attitude, motivation, personality, beliefs, among others, in the health of patients and/or in the effectiveness of medical procedures (Limonero and Bayés, 1995; Arranz et al., 2003; Mancuso et al., 2006; Pineapple Booksellers, 2012; Oblitas Guadalupe et al., 2017). Which is actually not an easy task.
For example, in the research by Hussain et al., (2015), an attempt was made to explore the relationship between the attitude of patients, satisfaction with treatment and the decrease in glycemic levels in patients with GDM, which would give rise to thinking about overcoming the pathology in these women. Although there were no conclusive results, this study was able to demonstrate that the presence of negative attitudes and levels Low satisfaction with treatment correlates with high glycemic levels.
There are other investigations that, although they were not developed exactly with women with GDM, are somewhat related to variables associated with the appearance of this pathology.
In the work of Lindsay et al., (2019), carried out with pregnant women for the first time developing excessive body weight, it was established that These women do not know exactly what the line is between being overweight and the obesity. That is, most of the study participants did not they knew if their body weight was in the healthy range. In addition, most of the women had accepting attitudes towards their weight gain, which suggests that pregnant women have beliefs related to the fact that weight gain is normal among pregnant.
On the other hand, there is also research interested in trying to modify psychosocial dimensions (habits, beliefs, lifestyles) in women diagnosed with GDM (Represas Carrera, 2021; Jelsma et al., 2016). Generally, these studies are carried out through interventions controlled. Brown et al., (2017), conducted lifestyle interventions with GDM in about 4501 women.
Intervention programs included physical activity, diet, blood glucose self-monitoring, health education. Results show some very important data such as the fact that women belonging to the experimental groups have a lower probability of develop postpartum depression. Additionally, these women improve their body weight significantly. From this investigative perspective there is quite hopeful findings for psychosocial treatment, both of women with GDM, as in diabetic patients of all kinds.
Finally, systematic reviews were consulted, such as the one developed by Craig et al., (2020), in relation to attitudes, perceptions and experiences of the women with GDM. These authors in a rigorous search and after ruling out several studies, they identified some 840 articles dealing with the theme in question.
After applying the inclusion and exclusion criteria, they reviewed full text 88 documents. Carrying out a systematization of these articles, 8 key themes of the experiences and subjectivities of women with GDM were identified: initial psychosocial impact, communication of the diagnosis, perception of irrigation, management before the DMG, load of the diagnosis of GDM, social support and gaining control.
## IV. DISCUSSION
The aim of this review was to conduct a systematic review around cognitions and beliefs present in women with GDM to improve knowledge of the pathology and adherence to treatment, generate models psychoeducational and involve the family group and the couple in the management only of the pathology, but throughout the pregnancy process.
In this research it was possible to establish that the beliefs and cognitions of women with this condition are located in two great edges. One of them called living experiences that bring happiness and the second experiencing experiences that cause suffering (Araujo et al., 2013).
Accordingly, it can be inferred that pregnant mothers with GDM, alternately run between these two polarities. surely there is some patients in whom one experience prevails more than the other. The most recurrent cognitions related to happiness are related to with ideas like "I am going to be a mother; I am with other women in the same conditions as mine and we will have a treatment that will help us overcome the pathology".
While the negative thoughts are located in the fact of moving away from home and in the pathology itself and its consequences, leading them to generate fear of their own death or that of their babies. Some recalled deaths of family members and acquaintances from illnesses associated with diabetes.
Going a little deeper into this negative set of cognitions and thoughts related to the diagnosis of GDM, it is necessary to mention the appearance of feelings of sadness, unfailingly articulated with human cognition system.
If the diagnosis is received untimely, as usually happens, recurrent thoughts full of concern associated with a number of events such as abrupt removal from home, hospitalization, loss of the continuity of daily life and the abrupt rupture of relationships relatives.
Other studies report the existence of beliefs around three themes fundamental: illness, health and self-care, which are formed as expected, due to the effects of socialization, education and previous experiences. Furthermore, the evidence shows that this system of beliefs remains stable over time (Hjelm et al., 2018).
However, a situation that worries women recurrently is the real possibility of having to make changes in their lifestyles, especially everything on topics such as diet or exercise. They are also concerned about the possibility having to take insulin.
In the field of health and disease, beliefs report a central element, both in health promotion and prevention of the disease, fundamental axes that cannot be left aside. In fact, care programs must be nourished by dimensions derived from culture, from the characteristics of groups, from the idiosyncrasies of peoples, from values, attitudes and beliefs and from other number of psychosocial variables. These elements are taken up by authors to adapt models around social education in health, called Health Belief Models (Rosenstock et al., 1988).
Accordingly, the beliefs and in general the cognitive system of the women with GDM depend largely on cultural dimensions and on the way in which societies construct their social representation of disease in general and particular pathologies.
The study of cognitions in people with GDM is important not only because such aspects are necessary in program design aimed at improving adherence to treatment and reducing food harmful for this type of patients.
There is something even more complex, and it is the fact that, although research is still incipient, this type of psychosocial variables (conditions cognitive difficulties, behavioral coping and the use of social support) presented in a negative way, can lead to stress and the appearance of various pathologies (Chida & Hamer 2008; Luceno Moreno et al., 2004; Vieco Gomez & Abello Llanos, 2014; Fernandez-Prada et al., 2017).
Ideas and cognitions that women with GDM have related to that this type of pathology can lead to a chronic disease such as type I or II diabetes, which some may think is irrational, Tellería (2014) highlights it as a belief that would act as a protective factor for initiate self-care behaviors in relation to eating and physical activity. This same author emphasizes that invariably the Women with this diagnosis tend to develop depression, anxiety, changes in their thoughts and attitudes about their lifestyles. The Anxiety is often related to future health.
Under this consideration, it is very important then, that the system of beliefs of these people allows the existence of favorable attitudes towards breastfeeding and also towards activities that promote health, to have higher levels of self-efficacy, greater perceived benefit, and less alcohol consumption.
But in reality the most relevant in relation to life experiences of women with this diagnosis and their cognitions, is that in general patients focus their thoughts, behaviors and motivation, around changes in their lifestyles to overcome the pathology and to prevent future problems for them and their babies, not only during the gestation period but also after childbirth.
## V. CONCLUSIONS
From this systematic review, firstly, it was observed that immediately after diagnosis women are invaded by a series of ruminations and thoughts that denote the level of concern in your belief system. Among the most recurrent ideas find "considering that this pathology will be irreversible, from now on Later I will have a chronic affection, I will have to use insulin for life" and others. There are also ideas related to the fact that the pregnancy will not come to term and even that her life is in danger and of your baby.
Likewise, many consider that the pathology they are suffering from is due to the fact that they did not take the necessary care in relation to the diet before pregnancy and are generally blamed for the lifestyle adopted until that moment. Despite this, it is also recorded by many women with GDM, who in general terms do meet the medical prescriptions and adopt the recommendations of officials health to get ahead.
From what is observed, the belief system of doctors and nurse's health personnel in general, notably influences the attitudes and thoughts of these patients. Hence the recommendations and instructions of this personnel are so important to mark habits and practices that lead to the permanent search for the well-being of these patients. In this sense, a very important power of reference is observed on the part of the medical staff.
Another element found is that the emergence of beliefs and systems of thought in relation to health and disease originate from the influence of parents, teachers, communication systems, processes of socialization, among others, which is why social and cultural variables are so telling in the formation of a certain system of beliefs. In addition, research shows that these systems are consolidated, being sometimes difficult to modify.
Although the investigation is still incipient, there are records that allow establish that psychosocial variables such as attitude, beliefs, cognitions, motivation, among others exert an influence on related to the appearance of certain pathologies. Similarly, variables of this type, like attitudes, beliefs, cognitions they can be quite promising for the management of many pathologies.
and interpretation: A.C.M.B., J.C.M.E., S.C.M.M., A.M., M.M.A., E.D.A.P.; Principal Investigator: A.C.M.B. Research: A.C.M.B., J.C.M.E., S.C.M.M., M.M.A., E.D.A.P.; Manuscript writing—Original draft preparation: A.C.M.B., J.C.M.E., S.C.M.M., A.M.; Drafting, revision and editing of the manuscript: A.C.M.B., J.C.M.E., S.C.M.M., A.M., M.M.A., E.D.A.P.; Visualization: J.C.M.E., S.C.M.M. Supervision, J.C.M.E., S.C.M.M. Acquisition of funds: J.C.M.E.
Acknowledgments: The authors present their thanks to the Simon Bolívar University of Barranquilla, Colombia. Conflict of interest: the authors state that they have no conflict of interest.
Financing funds: Self-financed.
Generating HTML Viewer...
References
53 Cites in Article
(2011). Standards of Medical Care in Diabetes—2011.
S Ansarzadeh,L Saléis,Z Mahmoodi,A Mohammadbeigi (2020). Factors affecting the quality of life in women with gestational diabetes mellitus: a path analysis model.
E Antos,B Nowak,J Olszewski (2013). The analysis of midwives' knowledge on the education of women with gestational diabetes and preparation for it.
Márcio Araújo,Sarah Pessoa,Marta Damasceno,Maria Zanetti (2013). Diabetes gestacional na perspectiva de mulheres grávidas hospitalizadas.
(2002). Guía completa sobre la diabetes.
P Arranz,C Coca,R Bayés,C Del Rincón,F Hernández-Navarro (2003). Intervención psicológica en pacientes que deben someterse a un trasplante de médula ósea.
Paulina Brahm,Verónica Valdés (2017). Beneficios de la lactancia materna y riesgos de no amamantar.
J Brown,N Alwan,J West,S Brown,C Mckinlay,D Farrar,C Crowther (2017). Lifestyle interventions for the treatment of women with gestational diabetes.
A Cartín (2011). Diabetes mellitus gestacional: generalidades.
Gabriel Morales,Joan Chipa (2008). Desarrollo de un Sistema de Información de Salud (SIS) basado en la Clasificación Internacional de Enfermedades (CIE-10) para el Centro de Atención Médica Integral de la Universidad de Los Andes.
Louise Craig,Rebecca Sims,Paul Glasziou,Rae Thomas (2020). Women’s experiences of a diagnosis of gestational diabetes mellitus: a systematic review.
Caroline Crowther,Janet Hiller,John Moss,Andrew Mcphee,William Jeffries,Jeffrey Robinson (2005). Effect of Treatment of Gestational Diabetes Mellitus on Pregnancy Outcomes.
Mayra Chávez-Courtois,Chelsea Graham,Irma Romero-Pérez,Georgina Sánchez-Miranda,Bernarda Sánchez-Jiménez,Otilia Perichart-Perera (2014). Experiencia y percepciones de la diabetes gestacional y su automanejo en un grupo de mujeres multíparas con sobrepeso.
Yoichi Chida,Mark Hamer (2008). Chronic psychosocial factors and acute physiological responses to laboratory-induced stress in healthy populations: A quantitative review of 30 years of investigations..
Y Chida,M Hamer (2008). An association of adverse psychosocial factors with diabetes mellitus: a meta-analytic review of longitudinal cohort studies.
M Dalfrà,A Nicolucci,T Bisson,B Bonsembiante,A Lapolla (2012). Quality of life in pregnancy and post-partum: a study in diabetic patients.
Bianca Devsam,Fiona Bogossian,Ann Peacock (2013). An interpretive review of women's experiences of gestational diabetes mellitus: Proposing a framework to enhance midwifery assessment.
M Díaz,R Amato,J Chávez,M Ramírez,S Rangel,L Rivera,J López (2013). Depresión y ansiedad en embarazadas.
P Damé,K Cherubini,P Goveia,G Pena,L Galliano,C Façanha,M Nunes (2017). Depressive symptoms in women with gestational diabetes mellitus: the LINDA-Brazil study.
M Fernández-Prada,J González-Cabrera,C Iribar-Ibabe,J Peinado (2017). Riesgos psicosociales y estrés como predictores del burnout en médicos internos residentes en el Servicio de Urgencias.
Robert Gatchel,Mark Oordt (2003). Clinical health psychology and primary care: Practical advice and clinical guidance for successful collaboration..
V Gracia,J Olmedo (2017). Diabetes gestacional: conceptos actuales.
M González-Ruiz,C Rodríguez-Bandala,M Salcedo-Vargas,E Martínez-Lara,F Enríquez-Espinoza,S Polo-Soto,. &floriano-Sánchez,E (2014). Actualidades en diabetes gestacional.
L Ge,B Albin,E Hadziabdic,K Hjelm,M Rask (2016). Beliefs about health and illness and health-related behavior among urban women with gestational diabetes mellitus in the southeast of China.
(2011). Cochrane Clinical Answers.
S Hinkle,G Louis,S Rawal,Y Zhu,P Albert,C Zhang (2016). A longitudinal study of depression and gestational diabetes in pregnancy and the postpartum period.
Katarina Hjelm,Kerstin Berntorp,Anders Frid,Anders Åberg,Jan Apelqvist (2008). Beliefs about health and illness in women managed for gestational diabetes in two organisations.
Katarina Hjelm,Karin Bard,Jan Apelqvist (2018). A qualitative study of developing beliefs about health, illness and healthcare in migrant African women with gestational diabetes living in Sweden.
Zahid Hussain,Zuraidah Yusoff,Syed Sulaiman (2015). Evaluation of knowledge regarding gestational diabetes mellitus and its association with glycaemic level: A Malaysian study.
Judith Jelsma,Karen Van Leeuwen,Nicolette Oostdam,Christopher Bunn,David Simmons,Gernot Desoye,Rosa Corcoy,Juan Adelantado,Alexandra Kautzky-Willer,Jürgen Harreiter,Frans Van Assche,Roland Devlieger,Dirk Timmerman,David Hill,Peter Damm,Elisabeth Mathiesen,Ewa Wender-Ozegowska,Agnieszka Zawiejska,Pablo Rebollo,Annunziata Lapolla,Maria Dalfrà,Stefano Del Prato,Alessandra Bertolotto,Fidelma Dunne,Dorte Jensen,Lise Andersen,Frank Snoek,Mireille Van Poppel (2016). Beliefs, Barriers, and Preferences of European Overweight Women to Adopt a Healthier Lifestyle in Pregnancy to Minimize Risk of Developing Gestational Diabetes Mellitus: An Explorative Study.
M Jiménez Chafey,M Dávila (2007). Psicodiabetes. Avancesen Psicología Latinoamericana.
Emily Jones,Cathy Roche,Susan Appel (2009). A Review of the Health Beliefs and Lifestyle Behaviors of Women with Previous Gestational Diabetes.
Roya Kelishadi,Sanam Farajian (2014). The protective effects of breastfeeding on chronic non-communicable diseases in adulthood: A review of evidence.
D Lakshmi,A John William Felix,R Devi,M Manobharathi (2018). Study on knowledge about gestational diabetes mellitus and its risk factors among antenatal mothers attending care, urban Chidambaram.
J Limonero,R Bayés (1995). Bienestar en el ámbito de los enfermos en situación terminal.
Ana Lindsay,Márcia Machado,Sherrie Wallington,Mary Greaney (2019). Sociocultural and interpersonal influences on latina women’s beliefs, attitudes, and experiences with gestational weight gain.
Liliana Libreros Piñeros (2012). El proceso salud enfermedad y la transdisciplinariedad.
Luceño Moreno,L Martín García,J Rubio Valdehita,S Díaz Ramiro,E (2004). Factores psicosociales en el entorno laboral, estrés y enfermedad.
Carol Mancuso,Melina Rincon,Wendy Sayles,Stephen Paget (2006). Longitudinal study of negative workplace events among employed rheumatoid arthritis patients and healthy controls.
Martínez De Salinas,M (2017). Perfil de la mujer con diabetes mellitus y enfermedad cardiovascular.
David Moher,Alessandro Liberati,Jennifer Tetzlaff,Douglas Altman,The Prisma Group (2010). Ítems de referencia para publicar Revisiones Sistemáticas y Metaanálisis: La Declaración PRISMA.
Luis Oblitas Guadalupe,Rosmery Turbay Miranda,Kelly-Johana Soto Prada,Tito Borrero,Omar Cortes Peña,Mildred Scarpati,María Ucrós Campo (2017). Incidencia de Mindfulness y Qi Gong sobre el Estado de Salud, Bienestar Psicológico, Satisfacción Vital y Estrés Laboral.
Seungmi Park,Jung Lee,Jang In Sun,Youngji Kim (2018). Knowledge and health beliefs about gestational diabetes and healthy pregnancy's breastfeeding intention.
S Palani,N Joseph,Y Tegene,A Zacharia,T Marew (2014). Gestational Diabetes.
Diana Uchuya Ramos (2011). Estilos de vida en pacientes adultos con diabetes mellitus tipo II del programa de hipertensión y diabetes - centro de salud - San Clemente 2024.
Husna Razee,Hidde Van Der Ploeg,Ilse Blignault,Ben Smith,Adrian Bauman,Mark Mclean,N Wah Cheung (2010). Beliefs, barriers, social support, and environmental influences related to diabetes risk behaviours among women with a history of gestational diabetes.
Xiomara Luna Zarsoza (2015). Nivel de conocimiento y actitudes preventivas sobre diabetes gestacional en gestantes atendidas en el Centro Materno Infantil San Genaro de Villa durante el periodo de julio a septiembre del año 2022, Lima-Perú.
Demian Herrera Morban,Manuel Colomé-Hidalgo (2020). Brechas de la investigación pediátrica en la República Dominicana.
Irwin Rosenstock,Victor Strecher,Marshall Becker (1988). Social Learning Theory and the Health Belief Model.
R Rubin (2000). Psychotherapy and counselling in diabetes mellitus.
D Sacks (2014). Diagnosis of gestational diabetes mellitus: it is time for international consensus.
Solange Flores Vásquez (2014). Nivel de depresión en pacientes con diabetes mellitus tipo II atendidos en el centro de salud Enrique Montenegro en el año 2022.
Germán Vieco Gómez,,Raimundo Abello Llanos (2014). Psychosocial factors at work, stress and morbidity around the world.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Juan Carlos Marín-Escobar. 2026. \u201cBeliefs and Attitudes in Women with Gestational Diabetes Mellitus. A Systematic Review\u201d. Global Journal of Medical Research - F: Diseases GJMR-F Volume 23 (GJMR Volume 23 Issue F2): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Subject: Global Journal of Medical Research - F: Diseases
Authors:
Juan Carlos Marín-Escobar, Sara Concepción Maury-Mena, Antolín Maury, Andrea Carolina Marín-Benítez, María Molina-Arteta, Emily Dayana Acuña-Polo, María Molina-Arteta,Emily Dayana Acuña-Polo (PhD/Dr. count: 0)
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































