Bilateral internal carotid artery agenesis is a very rare congenital anomaly. Intracranial blood circulation in the affected internal carotid artery side is provided by collateral vasculature, contralateral internal carotid artery through the anterior communicating artery, and from the vertebrobasilar system through the posterior communicating artery. People with this abnormality may be asymptomatic for many years. However, patients may also be present with ischemic stroke or subarachnoid hemorrhage, headache, and blurred vision. Diagnosis is usually incidental by the performance of carotid artery doppler ultrasonography or cervical/cranial magnetic resonance imaging owing to other symptoms. We report a case of bilateral internal carotid artery agenesis with pulsatile tinnitus lasting five years in the light of clinical presentation and imaging findings.
## I. INTRODUCTION
Tinnitus is the perception of sound in the absence of a corresponding external acoustic stimulus. This perception of the sound is associated with activity in the peripheral and central nervous systems that does not match the resonant or mechanical activity in the cochlea. The etiology of tinnitus development and maintenance is still unclear. One of the most common causes of tinnitus is pathological changes along the auditory pathway. Many abnormal conditions of the cochlea, such as sudden hearing loss, noise induced hearing loss, presbycusis or the use of ototoxic drugs, accompany this pathology. These lesions causing hearing loss can result in abnormal neuronal activity in the central auditory pathway. Other risk factors for tinnitus development or maintenance are rarely known (1-2). Tinnitus can be sometimes observed in the patients with normal hearing. The patient describes hearing as similar to ringing, roaring, buzzing, or other sounds. $10\% - 15\%$ of the population had tinnitus. It has two types: subjective and objective (3-4). Objective tinnitus is caused by a vascular or muscular origin. The first may be caused by either venous, arterial sources, or arteriovenous shunting. Vascular internal flow reflects rhythmically to the ear in accordance with the heartbeat and blood flow due to the disruption of turbulence. In patients with advanced pulsatile tinnitus, the clinician can sometimes hear these pulsatile sounds during auscultation of the neck and around the ear area. And also as, muscular pulsatile tinnitus results from myoclonus spasm of muscles, most commonly the palatal, tensor tympani, and stapedius. The most common form of tinnitus is non-pulsatile tinnitus, mostly associated with hearing loss and ear diseases (5,6). Pulsatile tinnitus is uncommon, not associated with ear disease but more often in the presence of abnormal extracranial or intracranial blood vessels or intracranial hypertension. Pulsatile tinnitus caused by intracranial hypertension is not synchronized with the heartbeat, and its differential diagnosis is more difficult. Intra-arterial or intravenous angiography, Computer tomography (CT) angiography, and magnetic resonance are used to diagnose classic vascular pulsatile tinnitus.
In this case, we report a patient with an infrequent vascular cause of ipsilateral tinnitus – bilateral internal carotid artery agenesis.
## II. CASE REPORT
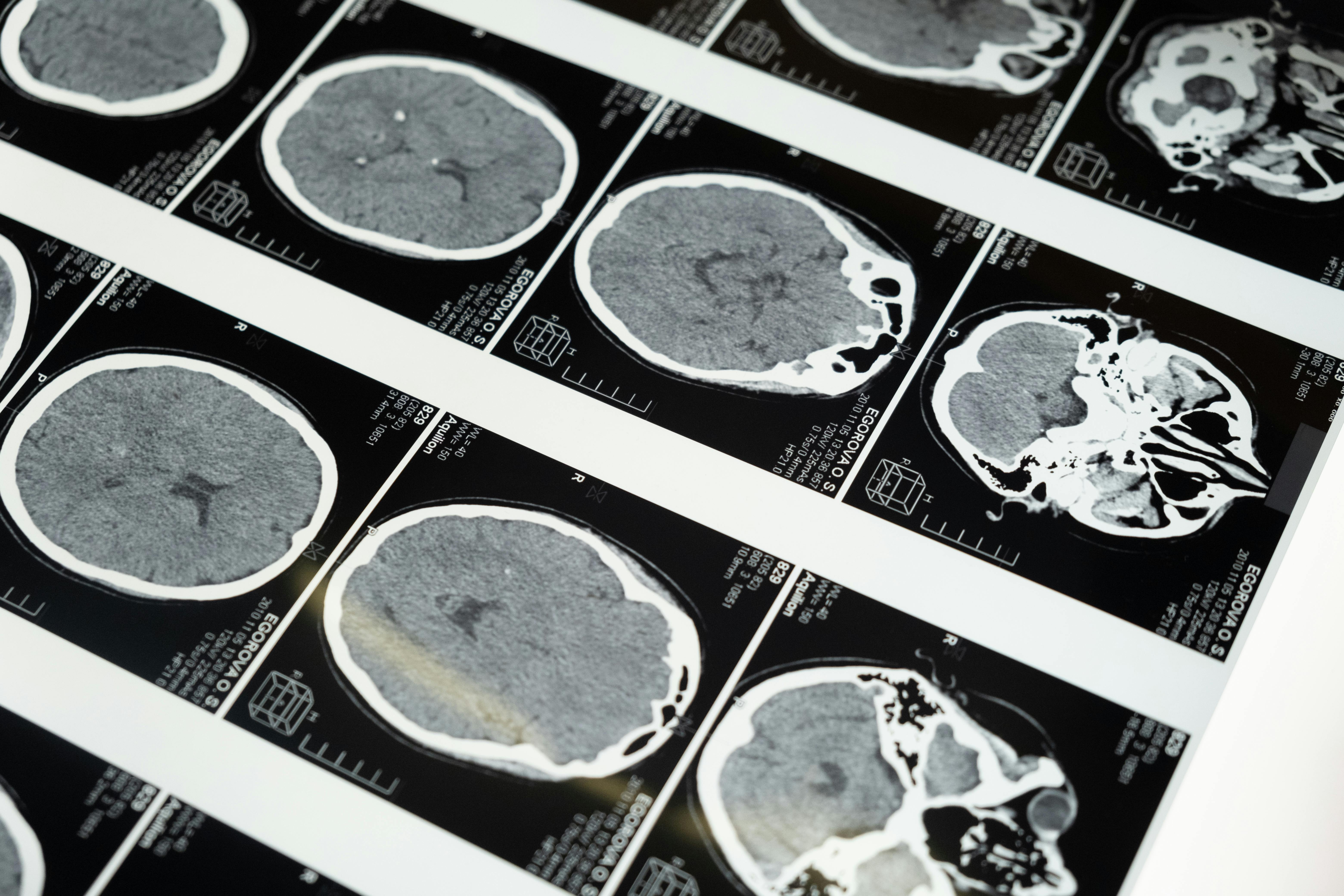
The patient was a 54-year-old white man who came to the ENT department with a 5-year history of bilateral tinnitus. The tinnitus prevented the patient from sleeping. A physical examination, rutin otorhinolaryngology controls, audiometry, and other tests were normal. Also, tinnitus was not heard during auscultation. We decided to evaluate the patient for another rare cause of tinnitus. A carotid duplex ultrasound study showed no bilaterally internal carotid arteries and blood flow. We performed cranial-cervical Magnetic resonance imaging (MRI) and CT angiography of the patient. CT angiography demonstrated agenesis of the bony carotid canal and smaller cavernous sinus (Figure 1). Blood circulation was supplied via the posterior and anterior communicating arteries. Bilateral ophthalmic arteries were supplied from meningeal arteries.
After consultation with the radiologist, the patient was definitively diagnosed with bilateral carotid agenesis. It was concluded that pulsatile tinnitus occurred in the patient in accordance with the rhythm of the heartbeat due to abnormal blood flow and turbulent flow. The patient was informed, all cardiological and cranial scans were performed, and no additional pathology was found. It was reported that there was no clear and definitive treatment for pulsatile tinnitus, and the patient was satisfied with this opinion and continued his routine controls.
## III. DISCUSSION
Internal carotid artery (ICA) agenesis is a very rare congenital anomaly with $< 0.01\%$ incidence (7,8). Tode reported the first absence of ICA in 1787 (9). Though unilateral ICA defect is common, a bilateral variant is also reported[6]. It is usually asymptomatic because of blood supply through anastomosis in the circle of Willis. In addition, blood circulation is possible with continuous embryologic vessels like the trigeminal artery and collaterales that originate extracranially[3,4]. But, it occasionally may be symptomatic and be associated with other congenital anomalies and acquired defects, like partial brain hypoplasia, a functional deficit of cranial nerves, etc.(10-13). Because of decreased blood supply in the affected size, adaptation may be provided unusual vasculature. So, it can cause abnormal vascular conditions like aneurysms and AVMs. Congenital ICA defects were described less in light of clinical neurological conditions. The clinical presentation includes commonly ischemic or hemorrhagic stroke, migraine, subarachnoid hemorrhage, contralateral motor weakness, Horner's syndrome, external ear defect, decreased hearing, and rarely tinnitus (7,8,12,13). Although the affected side is more susceptible to ischemia and can potentially cause clinical symptoms in unilateral cases, the contralateral side is becoming sensitive because of decreased circulation due to the shift of circulation to the affected side.
It should be considered the difference between agenesis, aplasia, and hypoplasia. Agenesis is a completely unsuccessful development with absent primordial tissue by definition. Aplasia is an absent organ in spite of the presence of the main primordial tissue. Hypoplasia is incomplete development, although primordial tissue is presented. Demonstration of the carotid canal is a nuance for differentiation. Even though MRI angiography is performed, CT of the head and neck should be administered to determine the presence/absence of a bony carotid canal(14). In our case, ICA is absent without a carotid canal, so we described it as agenesis. Also, we found a smaller cavernous sinus in the patient that is compatible with other cases in the literature (7).
The most common cause of objective vascular tinnitus is an arteriovenous malformation (AVM) in the posterior fossa (15). ICA agenesis is a very rare cause of tinnitus. Cohen et al. Reported one case of tinnitus caused by unilateral carotid artery agenesis (7).
Diagnosis is usually made incidentally with the performance of carotid artery doppler ultrasonography or cervical/cranial MRI and CT due to other symptoms (7). Also, CT or MRI angiogram is required to confirm the diagnosis and assess differential diagnoses (8). Differential diagnoses include congenital or acquired ICA stenosis, common carotid artery hypoplasia, and other aortic arch anomalies (12,16,17).
We report a rare case of bilateral tinnitus caused by bilateral ICA agenesis. There are less than 30 "Bilateral internal carotid artery agenesis" cases in the current literature. According to our knowledge, our report is the first case in which bilateral ICA causes tinnitus.
AA: Study design, examination of patients, data collection and analysis, manuscript development, and review of the final manuscript.
ZK: Manuscript development, writing, and review of the final manuscript.
OY: Manuscript development, and review of the final manuscript.
F.R.A: Manuscript development, and review of the final manuscript.
Funding: The authors have no funding or financial relationship to declare.
Availability of data and material: Data and material are available on request.
Conflict of interest: The authors declare that they have no conflict of interest.
Ethics approval: For A Case Report N/A
Consent to participate: Informed consent was obtained from the participant before including him in the case report.
Generating HTML Viewer...
References
17 Cites in Article
D Baguley,D Mcferran,D Hall (2013). Tinnitus.
S Pavaci,F Tortorella,A Fioretti,A Angelone,L Businco,M Lauriello (2019). Analysis of the audiological characteristics and comorbidity in patients with chronic tinnitus.
Alf Axelsson,Anders Ringdahl (1989). Tinnitus—a study of its prevalence and characteristics.
Dirk De Ridder,Ana Elgoyhen,Ranulfo Romo,Berthold Langguth (2011). Phantom percepts: Tinnitus and pain as persisting aversive memory networks.
Paul Ward,Richard Babin,Thomas Calcaterra,H Konrad (1975). Operative Treatment of Surgical Lesions with Objective Tinnitus.
M Paparella,O Shumric,W B Otolaryngology,Saunders (1973). Unknown Title.
José Cohen,John Gomori,Ronen Leker (2013). Internal carotid artery agenesis: diagnosis, clinical spectrum, associated conditions and its importance in the era of stroke interventions.
C Given,F Huang-Hellinger,M Baker,N Chepuri,Pearse Morris,P (2001). Congenital Absence of the Internal Carotid Artery: Case Reports and Review of the Collateral Circulation.
Tode Unknown Title.
Zoran Rumboldt,Mauricio Castillo,Sten Solander (2003). Bilateral congenital absence of the internal carotid artery.
P Clarós,R Bandos,I Gilea,A Clarós Jr.,A Capdevila,J Garcı́a Rodrı́guez,A Clarós (1999). Major congenital anomalies of the internal carotid artery: agenesis, aplasia and hypoplasia.
Z Berkman,M Erfiah‹n,N B‹ber,H Somay (2007). Metin ORAKDÖ⁄EN Agenesis of the Left Internal Carotid Artery Associated with Anterior Communicating Artery Aneurysm: Case Report Anterior Kominikan Arter Anevrizmas› ile Sol ‹nternal Karotid Arter Agenezisinin Birlikteli¤i: Olgu Sunumu.
Rebika Dhiman,Bhavya Gorimanipalli,Deepa Swamy,Sanjay Sharma,Ajay Garg,Rohit Saxena (2018). Congenital Third Nerve Palsy Associated With Midbrain Hypoplasia Due to Bilateral Segmental Internal Carotid Artery Agenesis.
Cole Graham,Gerald Capps,F Wippold (1999). Magnetic Resonance Imaging in Internal Carotid Artery Agenesis with Computed Tomography and Angiographic Correlation.
Iglauer Objective (1933). TINNITUS AURIUM: WITH REPORT OF FOUR CASES.
Omer Kaya,Cengiz Yilmaz,Bozkurt Gulek,Gokhan Soker,Gokalp Cikman,Ibrahim Inan,Selahaddin Demirduzen (2014). An Important Clue in the Sonographic Diagnosis of Internal Carotid Artery Agenesis: Ipsilateral Common Carotid Artery Hypoplasia.
Chang-Woo Park,Eun-Ju Jeon (2012). Pulsatile Tinnitus Arising from Aberrant Internal Carotid Artery at Nasopharynx.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Aynur Aliyeva. 2026. \u201cBilateral Internal Carotid Artery Agenesis : Very Rare Cause of Bilateral Pulsatile Tinnitus\u201d. Global Journal of Medical Research - J: Dentistry & Otolaryngology GJMR-J Volume 23 (GJMR Volume 23 Issue J1).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.