


I. INTRODUCTION
Pregnancy, a real challenge for the human body, is associated with a set of physiological and pathological changes. One of the most important pathologies accompanying pregnancy is the syndrome of preeclampsia/eclampsia. Toxaemia of pregnancy, or preeclampsia, is a general syndrome that affects of pregnant women, typically in the last trimester of pregnancy. It is characterized by arterial hypertension associated with proteinuria. It can be responsible for different ophthalmological manifestations. Visual symptoms affect up to of patients with severe preeclampsia and of patients with eclampsia, and numerous ophthalmologic manifestations have been described.
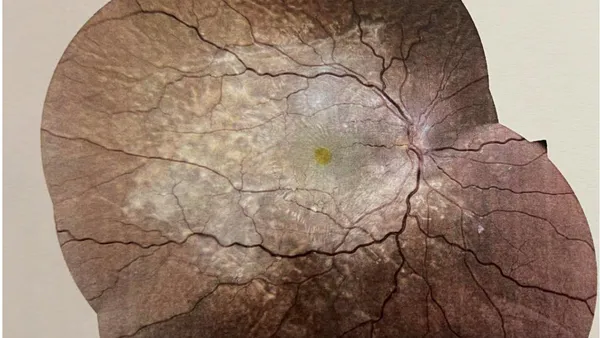
Clinical observation A 25-year-old patient, with no significant pathological history, primigravida, consulted the emergency room at 36 weeks of amenorrhea for headaches, edema of the lower limbs and bilateral visual blurring. A general clinical examination showed blood pressure at , heart rate at 90 bpm, fetal heart rate at 130 bpm. The proteinuria on the urine dipstick was 3 crosses , and the level of hepatic transaminases was high. The patient was hospitalized and an emergency caesarean was performed after fetal lung maturation. On day 1 postpartum, the blood pressure figures normalized and the edema subsided. On the other hand, the visual blurring worsened. The ophthalmological examination found visual acuity at 'counting fingers' from a distance in both eyes. The anterior segment was calm. Fundus examination reveals in both eyes, in a fairly symmetrical detachment with macular retinal folds and stage 1 papilledema (Figure. 1). OCT mapping shows in both eyes disorganization of the inter-papillo-macular retina with cystoid macular edema, macular thickening and presence of a cloudy DSR (Figure. 2) The patient was put on Acetazolamide by oral route at the rate of 3 times a day, Dorzolamide eye drops at the rate of 1 drop x3 per day and AINS eye drops at the rate of 1 drop x3 per day. The evolution at 15 days was favorable. Visual acuity was 5/10 in the right eye and 4/10 in the left eye. At 1 month postpartum, visual acuity was 9/10 in the right eye and 8/10 in the left eye with drying of the macular edema and serous detachment and disappearance of the papilledema.
II. DISCUSSION
Pre-eclampsia is defined by the World Health Organization (WHO) as being the association of arterial hypertension, proteinuria greater than hours or greater than 2 crosses on the urine dipstick from the 20th week of amenorrhea with or without edema of the lower limbs [1]. Severe pre-eclampsia (SPE) is defined by the appearance from the 20th week of amenorrhea of arterial hypertension whose systolic blood pressure (SBP) is greater than or equal to and/or diastolic blood pressure (TAD) greater than or equal to , and proteinuria greater than or equal to hours or greater than or equal to 3 crosses on the urine dipstick [1]. SPE can be complicated by eclampsia, which is a paroxysmal accident with dominant neurological expression, manifested by tonic-clonic convulsive seizures occurring in the context of unrecognized or untreated severe pre-eclampsia. It produces a repeated convulsive state followed by a comatose state and can occur during pregnancy after the 20th week of amenorrhea, during childbirth, or postpartum [1]. Pre-eclampsia/eclampsia is a public health problem. In fact, it is one of the three main causes of maternal mortality in the world [1, 2]. The ocular complications of pre-eclampsia are essentially due to arterial spasm and its consequences on the retinal and choroidal vascular circulation [3]. During pregnancy, pre-existing ocular pathologies can worsen, such as diabetic retinopathy and uveitis. Other ocular pathologies are specific to pregnancy and are complications of pre-eclampsia/eclampsia [4]. Visual symptoms include visual blurring, diplopia, transient amaurosis, photopsia, visual field deficit. These signs may be attributed to posterior cerebral artery vasospasm or cerebral edema in the occipital region. The most common ocular manifestation is the constriction of retinal arterioles found in of cases [4,5]. Other ocular manifestations are possible such as hypertensive retinopathy, retinal detachment, vitreous hemorrhage. Serous retinal detachment is a rare cause of decreased visual acuity in pre-eclampsia/eclampsia with an incidence of approximately in severe pre-eclampsia and in patients with eclampsia [6] The management of pre-eclampsia/eclampsia is multidisciplinary, it is carried out by obstetrician-gynecologists, cardiologists or anesthesiologists who administer the appropriate treatment. Regular monitoring of all severe forms of pre-eclampsia is recommended by measuring visual acuity and examining the fundus to detect ocular lesions early and indicate a cesarean in time [7, 8, 9, 10-12]. The signs observed at the fundus are elements of maternal vital prognosis but especially fetal.
III. CONCLUSION
Pre-eclampsia/eclampsia is a serious pathology for the mother and her future baby. It is sometimes accompanied by ocular but especially retinal lesions predicting the fetal and maternal prognosis, the early detection of which by an ophthalmologist helps to preserve the life of the mother-child couple. Because the risk for these patients of having a fetal death is one and a half times higher than in patients without lesions.



