## I. INTRODUCTION
M eckel's diverticulum is the most common congenital malformation of the gastrointestinal tract.
Due to the rarity of cases in adults, it is still misdiagnosed preoperatively.
We describe in our case a patient with bowel obstruction due to meckel's diverticulum.
## II. CASE PRESENTATION
Patient was 41-year-old man.
He had no medical history.
He was referred to our emergency, he had symptoms of intestinal obstruction: he couldn't have a pass gas, he noticed stomach pain and a swollen belly. He had no external gastrointestinal bleeding.
On examination, he was afebrile, with normal respiratory rate and normal resting heart rate.
On physical exam, the patient's abdomen was distended, tympanic on percussion.
Digital rectal exam was normal with no hematochezia.
Abdominal CT scan showed small and large bowel distention with a caliber disparity in the right iliac fossa and air-fluid levels.
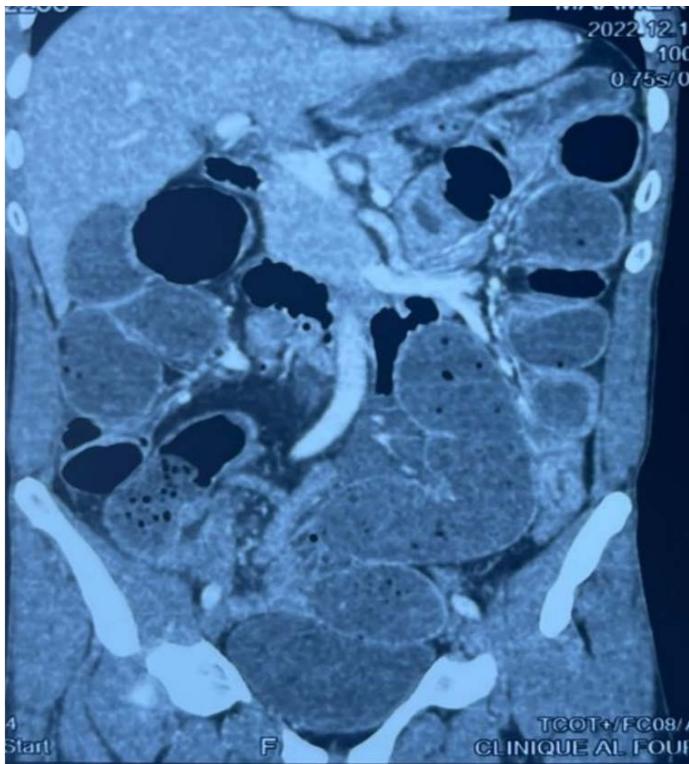 Figure 1: Caliber disparity in the right iliac fossa
 Figure 2: Air-fluid levels
On the same admission day, the patient was transferred to the operating room.
The patient and his family gave their approval to do surgery.
During laparotomy under general anesthesia, the exploration showed a meckel's diverticulum adhering to the abdominal wall, located at $60~\mathrm{cm}$ from the ileocecal valve responsible for a small bowel volvulus which is the site of perforative lesions and also responsible for distension of the small bowel measuring 5 cm.
We proceeded to $10\mathrm{cm}$ small bowel resection carrying a Meckel's diverticulum and perforative lesions and end to end bowel anastomosis.
The post-operative care was simple, he was discharged from hospital on postoperative day 5, after allowing liquid feeding without incident.
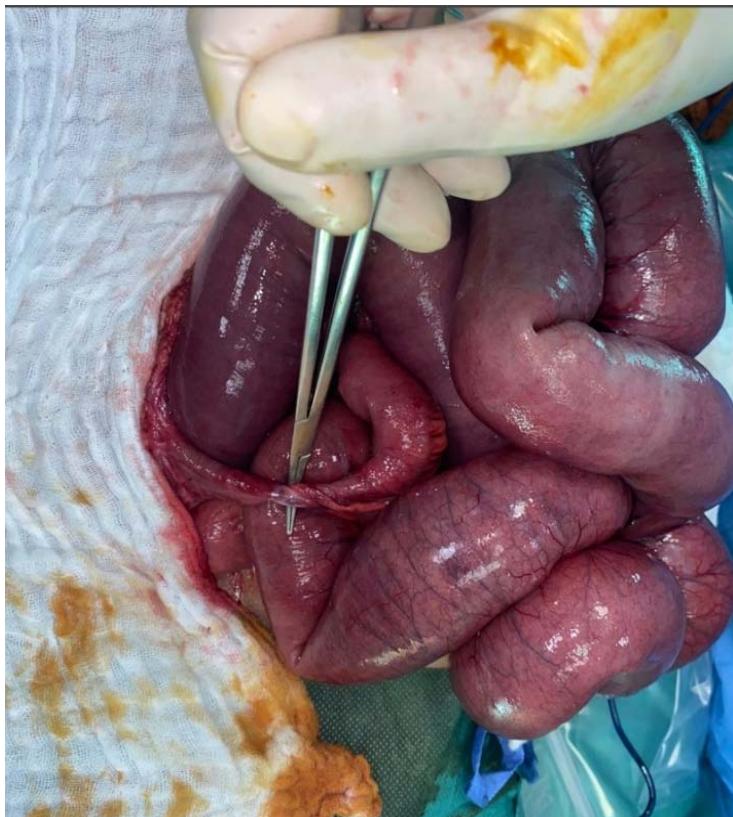 Figure 3: Meckel's diverticulum adhering to the abdominal wall

 Figure 4: Meckel's diverticulum becoming free Figure 5: A. Meckel's diverticulum-B. perforative lesions
## III. DISCUSSION
Meckel's diverticulum was named after Johann Friedrich Meckel, who described its anatomy and embryology in 1809 (2).
This anomaly is due to the incomplete obliteration of the omphalomesenteric duct during the 7th week of gestation and is classically located 2 feet proximal to the ileocecal valve (1).
Meckel's diverticula are lined with heterotopic mucosa in up to $60\%$ of cases in the following manner: gastric mucosa, $62\%$; pancreatic, $6\%$; both gastric and pancreatic, $5\%$; jejunal, $2\%$; Brunner's glands, $2\%$; and gastric and duodenal, $2\%$ (3).
Most of the population may be asymptomatic.
Bleeding from Meckel's diverticulum due to ectopic gastric mucosa is the most common clinical presentation, especially in younger patient, but it is rare in the adult population. The complications in adults include: obstruction; intussusception; ulceration; haemorrhage; and, rarely, vesicodiverticular fistulae and tumours (4).
The diverticulum is occasionally identified incidentally on imaging studies and may be found during the course of a laparotomy performed for other reasons. The preferred diagnostic method is laparoscopy in doubtful cases. However, laparoscopy is not an initial step of diagnostic modalities as it is more invasive compared to conventional imaging methods (5).
Plain X-ray, barium studies and computed tomography (CT) scans are seldom beneficial for a preoperative diagnosis of the diverticulum. The typical appearance of an intestinal obstruction may be demonstrated by plain abdominal radiographs. When distension develops in a diverticulum, diagnosis may be established due to a gas-filled viscous appearance in the right iliac fossa or middle abdomen region. If a perforation develops as a complication, the findings of pneumoperitoneum may be seen on upright chest and plain abdominal radiographs. Characteristically, the diverticulum is delineated as a contrast-filled out pouching which has a junctional fold pattern and is seated on the anti-mesenteric margin of the small bowel (5).
Ultrasonography, although not specific enough for imaging this condition, may reveal a tubular diverticulum swollen with fluid in a region away from the cecum, invagination, segmental thickening of the bowel walls, swelling of diverticular wall and pelvic abscess (6).
Capsule endoscopy is a novel technological tool for the examination of the small bowel in a noninvasive and simple manner. It has been proved in a number of studies that capsule endoscopy has the capability to detect small intestine lesions in cases with obscure gastrointestinal hemorrhage. The entire small intestine can be examined by both double-balloon enteroscopy and capsule endoscopy. For the detection of hemorrhagic lesions in the small bowel, other studies proved that the efficacy of both capsule endoscopy and double-balloon enteroscopy is similar. However, capsule endoscopy is contra-indicated and also difficult in cases under ten years of age. Furthermore, it is relatively simple to reach via the retrograde double-balloon enteroscopy method, as the distance of the Meckel's diverticulum is generally closer than a meter from the ileocecal valve (7).
The treatment for Meckel's diverticula is shown in this algorithm (8):
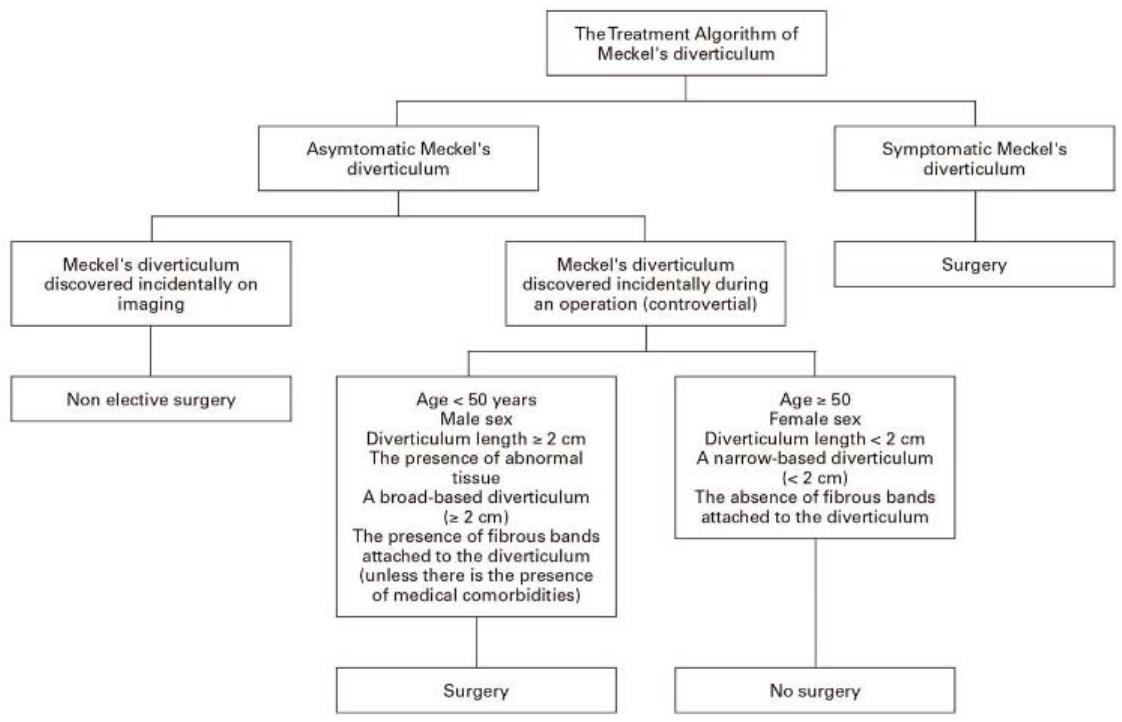 Figure 6: The treatment algorithm of Meckel's diverticulum
## IV. CONCLUSION
Meckel's diverticulum is the most prevalent congenital abnormality of the gastrointestinal tract. Most of the population may be asymptomatic.
A good level of knowledge of the clinical, embryological, radiological and pathological features of Meckel's diverticulum will enable a rapid and proper diagnosis of patients, thereby allowing treatment via a timely surgical intervention.
John Opitz,Rüdiger Schultka,Luminita Göbbel (2006). Meckel on developmental pathology.
Miltiadis Matsagas,M Fatouros,B Koulouras,A Giannoukas (1995). Incidence, Complications, and Management of Meckel's Diverticulum.
Jayesh Sagar,Vikas Kumar,D Shah (2006). Meckel's Diverticulum: a Systematic Review.
Shams-Ul-Bari,K Wani,A Khaja,A Malik (2010). Meckel′s diverticulum -Revisited.
V Miele,De Cicco,M Andreoli,C Buffa,V Adami,L David,V (2001). US and CT findings in complicated Meckel diverticulum.
C Zheng,Y Huang,Z Tang,L Chen,Y Leung,Kit (2014). Double-balloon enteroscopy for the diagnosis of Meckel's diverticulum in pediatric patients with obscure GI bleeding.
Serdar Kuru,Kemal Kismet (2018). Meckel�s diverticulum: clinical features, diagnosis and management.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Benjelloun Touimi Kenza. 2026. \u201cBowel Obstruction due to Meckel’s Diverticulum : A Case Report\u201d. Global Journal of Medical Research - K: Interdisciplinary GJMR-K Volume 23 (GJMR Volume 23 Issue K2).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































