## INTRODUCTION
A 14-year-old female presented with multiple dark coloured, itchy lesions on legssince5 months. On examination, multiple violaceous papules to plaques of varying sizes (1cm - 5cm) were present on the extensor aspects of legs, forearm and dorsum of feet bilaterally. (Figs 1-3). Skin biopsy from the lesion showed hyperkeratosis, hypergranulosis, vacuolar degeneration of basal layer, band of dense lymphocytic inflammatory infiltrate in the papillary dermis, with perivascular histiocytic infiltrate confirming the diagnosis of lichen planus (LP) (Fig 4,5). She was started on topical corticosteroids, antihistamines and emollients. After 3 months patient had aggravation of LP with patchy hair loss over the scalp. On examination multiple, smooth alopecic patches of varying sizes, the largest being $4 \times 3 \mathrm{~cm}$, were noticed on the scalp. She was diagnosed clinically as alopecia areata (AA) (Fig 6). Investigations like complete blood count, liver function test, thyroid profile, anti-nuclear antibody, rheumatoid arthritis factor, C-reactive protein, ESR, VDRL, HBV, HCV, urine microscopy were normal. In view of progressing lesions of LP and AA, she was started on oral mini pulse therapy-betamethasone 5 mg twice weekly and was advised for follow-up. Good response was noticed by four weeks withresolution of LP and regrowth of hair over few patches.
LP and AA are autoimmune dermatoses and are associated with other conditions like diabetes mellitus, vitiligo, autoimmune thyroid diseases etc to name a few. So far, only 3 reports of co-localization of AA and LP have been published in the literature. Till now, no case report of coexistence of LP and AA has been reported. Plasmacytoid dendritic cells (pDCs) are specialized dendritic cells exhibiting plasma cell morphology, expressing CD4, CD123, HLA-DR, blood-derived dendritic cell antigen-2 (BDCA-2), Toll-like receptor (TLR)7 and TLR9 within endosomal compartments and their role in autoimmune diseases is gaining traction recently. On activation, they produce type I IFN, against pathogenic agents and link the innate and adaptive immunity by controlling the function of myeloid dendritic cells, T, B and natural killer cells. pDCs are absent in normal skin but infiltrate when injured, thereby contributing in the pathogenesis of inflammatory dermatoses (like LP and AA). Vries et al found pDCs in close approximation to basal layer in lesional LP, corresponding to lymphocytic infiltration. It has been hypothesized that some common antigenic determinant may be a triggering factor for onset of both diseases, and thus, a primary autoimmune process directed against basal epidermal cells in LP could have possibly resulted in disruption of hair follicle immune privilege zone thereby exposing the hidden antigens from hair follicles, leading to pDCs recruitment, production of IFN-gamma and resulting in aggravation of LP and occurrence of secondary autoimmune response i.e., AA.
This explains the coexistence of LP and AA in our case report. This rare case of sequential occurrence of LP followed by AA has not been reported previously and might offer possible theories which contributes to the literature of T cell mediated autoimmune disorders.
1. Mushtaq S. Lichen Planus and Alopecia Areata Co-Localization. Indian J Dermatol 2021; 66: 101-103.
2. Kar BR, Ebenezer G, Job CK. Colocalisation of alopecia areata and lichen planus. Indian J Dermatol VenereolLeprol2004; 70: 242-3.
3. Hassan I, Anwar P, Sajad P. Co-localisation of alopecia areata and lichen planus: Rare presentation. Nepal J Dermatol VenereolLeprol2014; 12: 45-7.
4. De Vries HJ, van Marle J, Teunissen MB, Picavet D, Zorgdrager F, Bos JD et al. Lichen planus is associated with human herpesvirus type 7 replication and infiltration of plasmacytoid dendritic cells. Br J Dermatol 2006; 154: 361-4.
5. Chan LS, Vanderlugt CJ, Hashimoto T, Nishikawa T, Zone JJ, Black MM et al. Epitope spreading: lessons from autoimmune skin diseases. J Invest Dermatol 1998; 110: 103-9.

Figure 1: Multiple violaceous papules to plaques of varying sizes over the extensor aspects of both legs bilaterally.

Figure 2: Multiple violaceous papules to plaques over the dorsum of feet bilaterally.

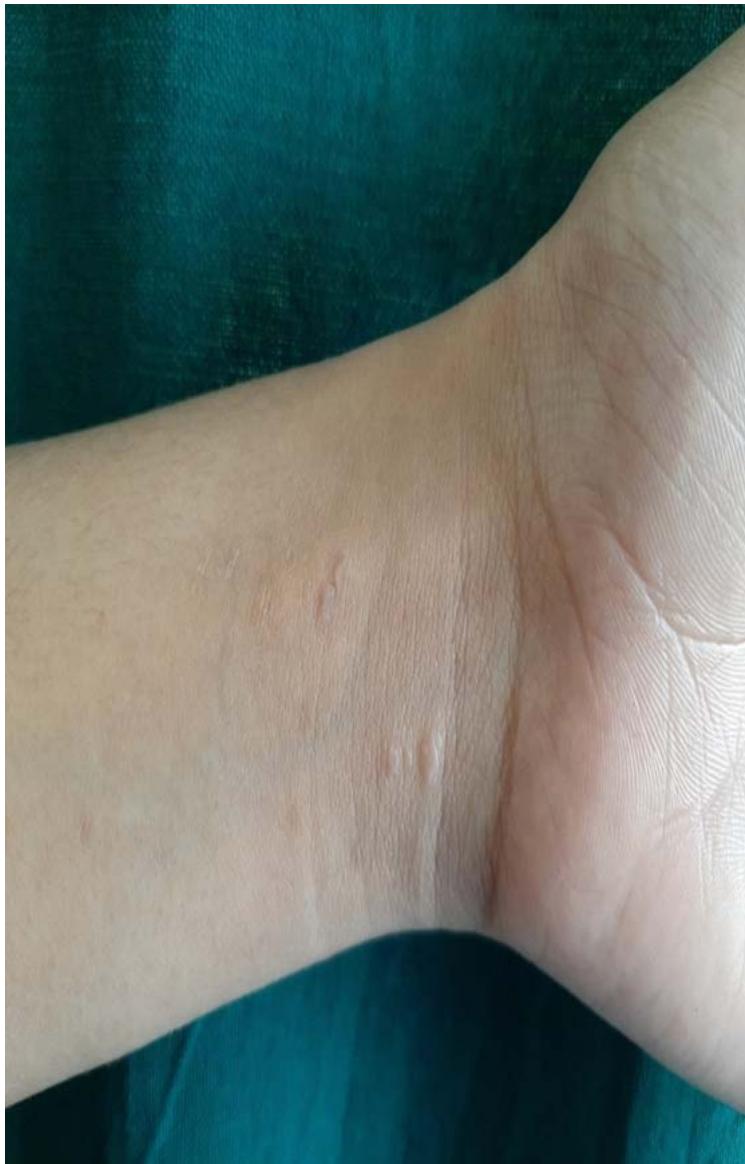
Figure 3: Few erythematous papules over the wrist area.
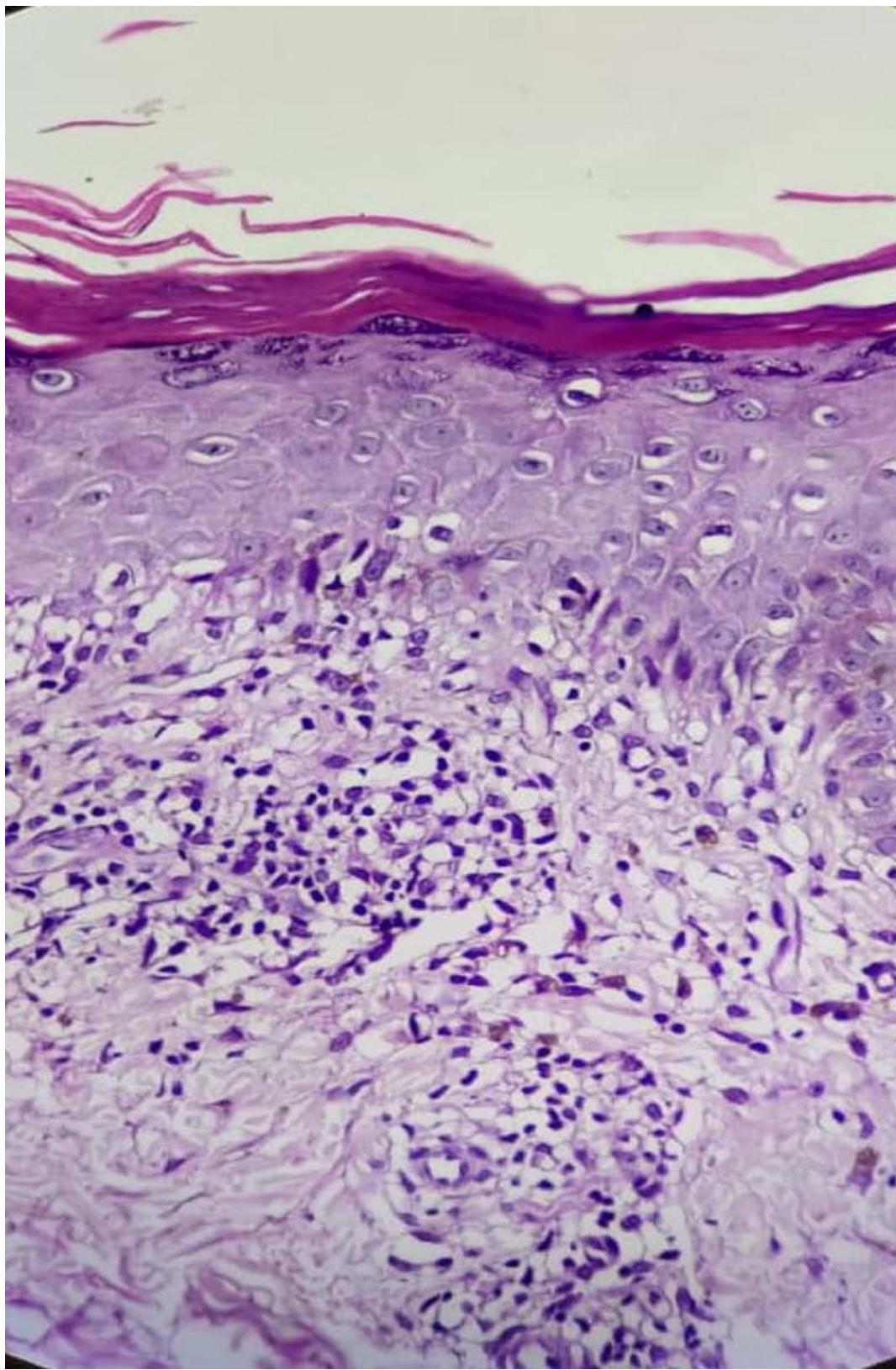
Figure 4: Photomicrograph showing hyperkeratosis, parakeratosis, hypergranulosis, band of dense lymphocytic inflammatory infiltrate, histiocytes admixed with congested blood vessels, along with periadnexal inflammatory infiltrate. (H & E, x 40).
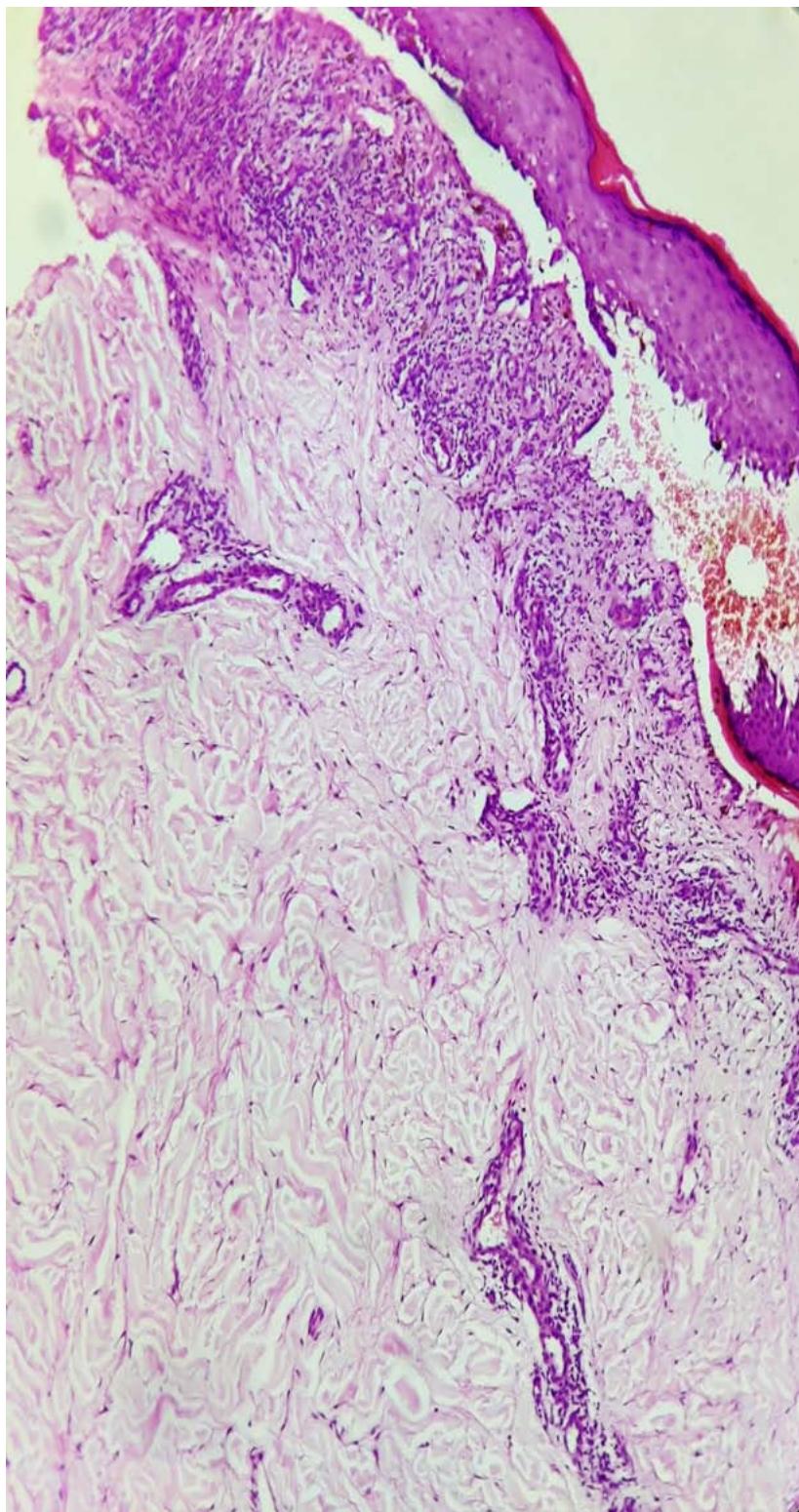
Figure 5: Photomicrograph showing hyperkeratosis, parakeratosis, hypergranulosis, artifactual cleft formation between epidermis and papillary dermis (Max Joseph space), band of dense lymphocytic inflammatory infiltrate, histiocytes admixed with congested blood vessels, along with periadnexal inflammatory infiltrate. (H & E, x 10).
 Figure 6: Multiple well demarcated, smooth, bald, round alopecic patches of hair loss of varying sizes on the scalp.
Generating HTML Viewer...
References
6 Cites in Article
S Mushtaq (2021). Lichen Planus and Alopecia Areata Co-Localization.
B Kar,G Ebenezer,C Job (2004). Colocalisation of alopecia areata and lichen planus.
I Hassan,P Anwar,P Sajad (2014). Co-localisation of alopecia areata and lichen planus: Rare presentation.
De Vries,H Van Marle,J Teunissen,M Picavet,D Zorgdrager,F Bos,J (2006). Lichen planus is associated with human herpesvirus type 7 replication and infiltration of plasmacytoid dendritic cells.
Lawrence Chan,Carol Vanderlugt,Takashi Hashimoto,Takeji Nishikawa,John Zone,Martin Black,Fenella Wojnarowska,Seth Stevens,Mei Chen,Janet Fairley,David Woodley,Stephen Miller,Kenneth Gordon (1998). Epitope Spreading: Lessons From Autoimmune Skin Diseases.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Dr. Harshita Sharma. 2026. \u201cCo-Occurrence of Lichen Planus and Alopecia Areata: A Possible Role of Plasmacytoid Dendritic Cells\u201d. Global Journal of Medical Research - F: Diseases GJMR-F Volume 23 (GJMR Volume 23 Issue F3): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































