BA Kadiatou $^\alpha$, Tall Aichata $^\sigma$, Sidibe Moro $^\rho$, Danfaga Bakary $^\circ$, Cissoko Sadio $^\yen$, Diallo Oumar $^\varsigma$, Simaga Assiatou $^\chi$, Toure Aoua Ibrahim $^\nu$, Diallo Seydou $^\theta$, Toure Ousmane $^\zeta$, Sidibe Mohamed Kolé $^\ell$, Saye Gounon $^\epsilon$, Sissoko Modibo $^\sharp$, Coulibaly Mory $^\tau$, Dembele Adama $^\varphi$, Coulibaly Abdoulaye Nouhoum $^\text{※}$ & Sylla Fatoumata $^\ddagger$
## I. INTRODUCTION
Myiases correspond to infestations of humans and animals by Diptera larvae[1]; [2], characterized by the accidental presence of fly larvae in the conjunctiva[3]; [4]; [5]. They are mainly found in populations living in direct contact with ungulates, sheep and goats [1], [6]. There are two types of ophthalmological involvement: external conjunctival ophthalmomyiasis, which is most often benign and quite frequent, and internal ophthalmomyiasis, which constitutes $5\%$ of all ophthalmomyiases but which often leads to serious complications [1]; [7]. Human ophthalmomyiasis externa is cosmopolitan but seems more common in Mediterranean countries [8]. We report two cases of external ophthalmomyiasis (conjunctival myiasis).
Author p Φ: Regional Hospital of Sikasso, Mali/Alliance for the Development of Community Ophthalmology (ADOC), Bamako, Mali Author C ¥: Kati Reference Health Center, Koulikoro, Mali.
Author $\S A$: Alliance for the Development of Community Ophthalmology (ADOC), Bamako, Mali.
The purpose of this study is to draw the attention of ophthalmologists to this rare pathology, to clarify its diagnosis, its treatment and its complications.
## II. OBSERVATION
### a) Observation 1
It was a 9-year-old boy residing in a peri-urban area with his grandmother who keeps sheep at home, received in emergency consultation for sensations of foreign bodies moving in the right eye, with pain and redness. The interrogation allowed us to know that the child received an insect blow (unidentified) at the level of this eye 17 hours before the consultation. Visual acuity was 10/10 at both eyes.
Slit lamp examination (LAF) revealed diffuse tarsal and bulbar conjunctival hyperaemia in the right eye, there presence of small moving bodies whitish in appearance, about 1 mm long dispersed on the ocular surface at the level of the tarsus and in the conjunctival cul-de-sac (about ten), fowing light from the LAF (photophobic) (Figure 1). The rest of the anterior segment examination as well as the posterior segment were normal. The Adelphe eye was normal in all its components.
Parasitological diagnosis revealed first stage larvae of Oestrusovis (L1).
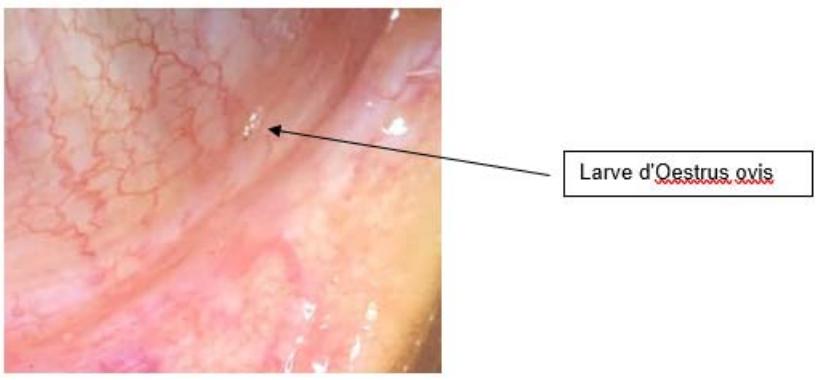 Figure 1: Macroscopic appearance of the first stage L1 Oestrusovis larva.
 Figure 2: Appearance on the fifteenth day (D15) of the treatment.
### b) Observation 2
It was a 16-year-old boy residing in an urban area received in emergency consultation for tingling sensations in the right eye, with ocular redness occurring on waking. The interrogation allowed us to find a notion of an insect bite (unidentified) in the right eye (OD), while driving a motorcycle the day before his admission to the consultation. Visual acuity was 10/10 in both eyes.
Slit lamp examination revealed conjunctival redness in the right eye, the presence of small moving bodies in appearance whitish, about 1 mm long, dispersed on the ocular surface at the level of the tarsus and in the conjunctival sac (4 in number) fleeing the light of the slit lamp (photophobic). The rest of the anterior segment examination as well as the posterior segment were normal.
The Adelphe eye was normal in all its components.
Parasitological diagnosis revealed first stage larvae of Oestrus ovis (L1).
In total we concluded to a conjunctival myiasis of the right eye.
The evolution was favorable with the disappearance of the functional signs, the reduction of the conjunctival hyperaemia, the total absence of larva on the ocular surface on D1, followed by the total disappearance of the signs and without any larva on the seventh day (D7) and on the fifteenth day (D15) and recovery without sequelae (Figure 3).
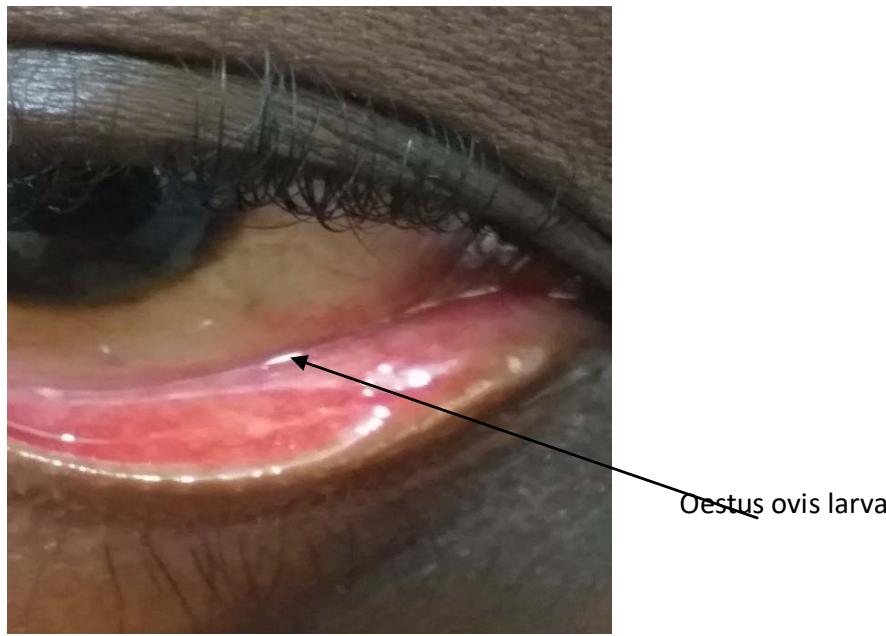 Figure 3: Macroscopic appearance of the first stage L1 Oestrusovis larva.
c) The D Description of larva of OESTRUS OVIS STAGE 1
Microscopic examination revealed that the larvaeovoid in shape with tapered ends, averaging 1mm long by 0.36mm wide with 12 segments or metamers, were comparable to the electron microscopic image of Steven JD in 1991 (Figure 4) [9].
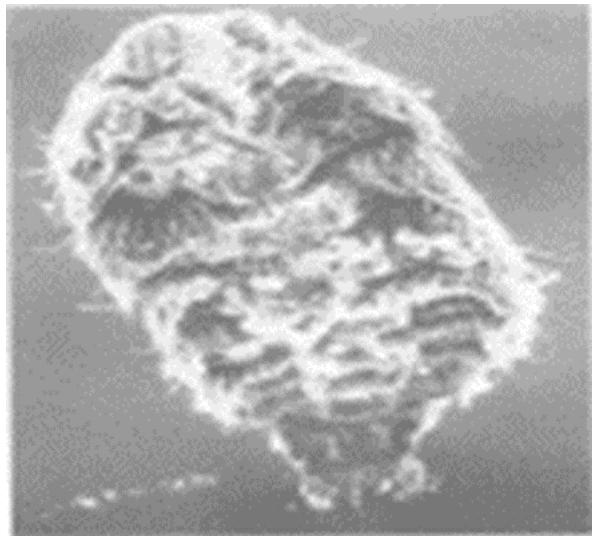 Fig. 4: Larva of oestrus ovis: ventral side [electron microscopy image (x120) Showing the cat's claw hooks curved and arranged in 2 groups] Source: Steven JD et al Br J Ophthalmol 1991(75) [9]
The cephalic end corresponding to the first metamer bears 2 strong mouth hooks, black, sclerotic curved, having the shape of hornsconsistent with the morphological description of Oestrus ovis larvaeL1 in the literature JD (Figure 5).
 Fig. 5: Oestus ovis larva: cephalic end [electron microscopy image (x340) showing the 2 hooks curved in the shape of a horn]. Source: Steven JD et al Br J Ophthalmol 1991(75) [9]
## III. DISCUSSIONS
Myiasis is a pathology due to the presence of fly larvae in the human body. External conjunctival ophthalmomyias represent the most frequent form of ophthalmomyases[1].It is a rare cosmopolitan disease [1],[10] usually observed in rural areas where animals are found grazing [11,]. Butobservations of external human oculomyias occurring outside the breeding environment have been described[5],[12]; [13]. One of our observations lives in a suburban area with the notion of sheep farming in the family but the second observation lives in an urban area.
They are due to the accidental presence in the human conjunctival sac of larvae of insects belonging to the order Diptera and the family Oestridae.[1], [3]. They are non-biting flies and the 2 species most often found in conjunctival myiasis are Oestrus ovis and more rarely Rhinoestrus purpureus[1] [3]. Oestrus ovis is asmall gray fly $10\mathrm{mm}$ longwhose larval development necessarily takes place on intermediate hosts such as sheep and goats[1] [2].
Viviparous females of Oestrus ovis deposit first instar (L1) larvae directly into the nasal orifices of sheep and goats. The L1s actively penetrate through the nasal orifices and colonize the turbinates and the septum where they develop. Once located in the ethmoid, L1 molts into stage 2 (L2) larvae. L2 then ascend from the nasal cavity to the frontal sinuses where they molt to become instar 3 (L3) larvae. Subsequently, L3s are expelled from the host's nasal cavity by sneezing via nasal mucus which then contaminates the soils. Then L3 pupates within 12-24 h. Finally, when external conditions are favorable, the pupa molts into an adult fly in 30 to 34 days [10]. AT accidentally, females of Oestrusovis deposit first instar (L1) larvae directly on the human conjunctiva [1];[10] causing estrosion by larval deposition in the eye[11] [4], less frequently in the ears, nose or throat[4]. This is the case of our 2 observations.
Evolution in humans is self-limited, the larvae do not develop beyond the first instar [1] [4].
The circumstances of discovery are most often a notion of shock to the eye, followed by a sensation of a foreign body [1]; [13], as was the case in our observations.
On the other hand, Meusnier et al [5] reported an observation with no history or notion of trauma on a non-atopic site presenting with left ocular pruritus of suddenonset.
Clinically, conjunctival myiasis is manifested by superficial external forms (External Ocular Myiasis) classically associated with irritation, photophobia and pain, or deep internal forms (Internal Ocular Myiasis) potentially associated with blindness.[10], [14].
Our observations were conjunctival myiasis, associating a sensation of foreign bodies with irritation, photophobia, pain in one of our observations and conjunctival hyperemia.
In the case reported by Meusnier et al [5], the clinical signs were unilateral diffuse conjunctival hyperaemia associated with subpalpebral edema without chemosis or photophobia, whereas Narjisse et al found a foreign body sensation with pruritus and tearing in their observation [12].
Diagnosis based on the detection of larvae on slit lamp examination, approximately 1 mm long, highly motile, which flee light to hide in the inner or outer corner of the eye. These larvae are white, translucent and ringed with a small head with a black anterior part (corresponding to the black hooks) [11] [10], [1], as was the case with our observations confirmed by the report from the parasitology department.
The treatment of human estrosis is based on the extraction of the larvae. For external ocular myiasis the extraction of the larvae is done manually and preferably under local anesthesia in order to immobilize them, because the larvae flee the light[5];[12]as was the case with our observations. Local antiseptics and antibiotics can be combined to avoid superinfection [5]; [10], as well as anti-inflammatory eye drops to treat inflammation [1]; [13]. We administered after the extraction of all the larvae ciprofloxacin eye drops for our first observation and rifamycin eye drops for our second observation.
The evolution of this pathology is most often benign and very rarely becomes complicated in a deep form. The serious forms are due to the ocular penetration of the larvae which can migrate into the vitreous, under the retina or in the choroid [1], [3], [5].
This intraocular migration of the larvae can be responsible for serious ocular lesions, a very significant inflammatory reaction in the form of panuveitis which can lead to blindness [7],[4], [12][15].and even orbital which resulted in the exenteration of the affected eye [16].
Prompt diagnosis and complete extraction can prevent these complications [5].<sup>[12]</sup>. Our observations had complete healing without any complications.
## IV. CONCLUSION
Conjunctival myiasis characterized by the accidental presence of fly larvae requires adequate and early treatment. Thus we can avoid the evolution towards the severe complications of internal ophthalmomyasis which can be potentially blinding. Hence the importance of a rapid ophthalmological consultation in the face of any sign of conjunctival irritation and the wearing of protective glasses when riding a motorcycle.
Generating HTML Viewer...
References
16 Cites in Article
J Diallo (2013). OOestrus ovis external phthalmomyiasis: about 2 cases observed in BOBO DIOULASSO (BOURKINA FASO).
F Rodhain,C Perez (1985). Myiasigenic diptera.
S Anane,L Ben Hssine (2010). La myiase conjonctivale humaine à Oestrus ovis dans le sud tunisien.
P Brisou,G Menard (2000). External ophthalmomyiasis caused by Oestrus ovis on a Var beach.
J Yilma,P Dorchies (1991). Epidemiology of Oestrus ovis in southwest France.
R Khoumiri,L Gaboune,A Sayouti,N Benfdil,B Ouaggag,B Jellab,T Baha,A Moutaouakil (2008). Ophtalmomyiase interne : à propos de deux cas.
Dorchies Ph (1977). Comparative pathophysiology of Oestrus ovis (Linné 1761) myiasis in humans and animals.
J Stevens,Ace Mccartney,R Howes (1991). Oestrus ovis ophthalmomyiasis acquired in the UK: case report and scanning electron microscopic study..
L Basmaciyan (2018). Oestrus ovis external ophthalmomyiasis: a case report in Burgundy France.
D Saadouli,Ben Mansour,K,S Feki,H Mlaouhia (2021). Review of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Global Congress 2025.
Narjisse Taouri,Alae Bouaychi,Ouafae Cherkaoui (2020). Ophtalmomyiase humaine extene: à propos d’un cas.
N Ouattassi,|| Laaribi,|| Alsubari,F Asri,|| Reda,|| Oubaaz (2018). External Ophthalmomyase In Urban Environments In Morocco.
Bms Venkatesh,P Bhavani (2021). External ophthalmomyiasis by Oestrus ovis larvae: A Rare Case Report.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
BA Kadiatou. 2026. \u201cConjunctival Myiasis: Two Cases at the Kati Health Center\u201d. Global Journal of Medical Research - F: Diseases GJMR-F Volume 23 (GJMR Volume 23 Issue F5): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































