## I. INTRODUCTION
E Pidermoid cysts in the gluteal region are rare benign tumors that can develop from epithelial cells of the skin. They generally have a good prognosis and are often discovered incidentally. However, their symptomatology can vary depending on their size and location. Although they can appear any where on the body, they are rare in the gluteal region. Diagnosis is based primarily on clinical examination, but ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI) are the most commonly used imaging modalities to characterize these cysts and assess their locoregional extension. Definitive diagnosis based on histology and immunohistochemistry.
Epidermoid cysts are rare and represent less than $1\%$ of all skin tumors. They occur most commonly on the head, neck, and trunk and are rare in the gluteal region. They occur more frequently in young and middle-aged adults, with a slight predominance in women. In a review of review of 432 cases of epidermoid cysts, only seven cases were reported in the gluteal region (1)
## II. CASE REPORT
We report the case of a 63-year-old woman, without any notable pathological history, who presented for one year with a bulging right gluteal mass that was progressively increasing in size. This mass was palpable to the firm touch, sensitive to the contact and was bleeding. It was located in the right lower gluteal quadrant and fixed relative to the gluteal muscle (Figure 1). Helical imaging was performed after intravenous contrast injection, revealing a large hypodense tissue mass occupying the right gluteal region, measuring $12 \times 8.1 \, \text{cm}$ with no other secondary locations (Figure 2).

 Figure 1: Preoperative image of a giant right gluteal mass
Surgical excision was proposed to the patient, who accepted the procedure. A carcinological resection was performed (Figure 3). Histopathological examination on section revealed a mammariescystic formation, the wall of which is made of stratified, keratinized epithelium delimiting a cavity where degradation products of desquamated epithelial cells accumulate in the form of an amorphous material, rich in keratin and cholesterol (Figure 4).

Figure 2: Computed tomography scan showing gross mass of the region Gluteal
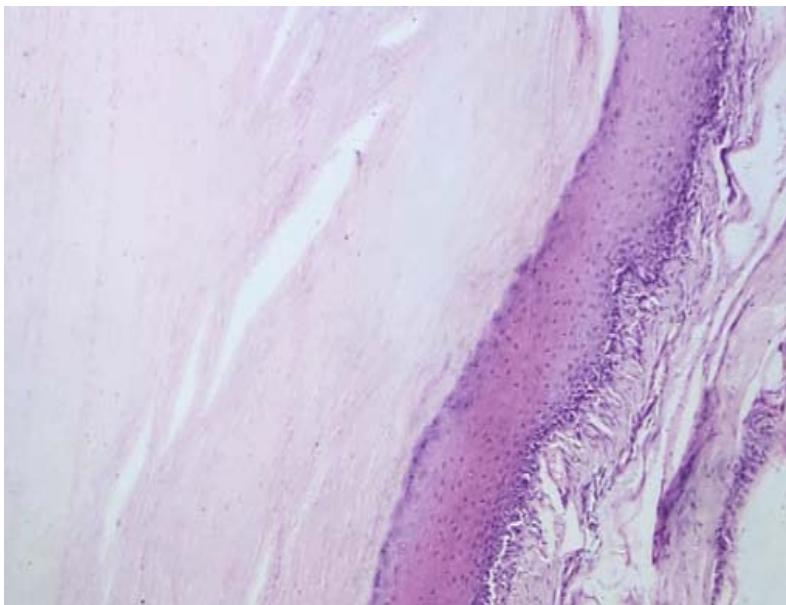 Figure 3: Image showing the surgical specimen of the right gluteal region Figure 4: Pathological specimen demonstrated a mammaries cystic formation with a stratified, keratinized epithelium in the wal. (coloration HE Gx100)
## III. DISCUSSION
The circumstances of discovery may vary for an epidermoid cyst of the buttock. Their growth is very slow and symptoms occurlate (2). Symptoms vary depending on the tumor location (3). In this particular case, the patient presented with a painful mass in the right but tock, which led to imaging to evaluate the cause of the pain. Possible clinical presentations include a painful mass, pain on palpation, and discomfort with walking or physical activities (4).
The diagnosis of epidermoid cyst of the right buttock can be established by imaging, such as ultrasound or computed tomography (CT). In this case, CT was used to confirm the diagnosis and locoregional extension. On CT, the epidermoid cyst typically presents as an iso or hypodense, heterogeneous, irregularly contoured mass without any contrast and without perilesionaledema (5). The diagnosis confirmed by MRI and in particular by their hyper signal on diffusion sequences. Diffusion sequences are essential to confirm the diagnosis on MRI (6). The evolution of gluteal epidermoid cysts is very slow. They are usually monitored by regular MRI. Surgical treatment is proposed if symptoms are present. If symptoms are moderate and the risk of surgery is considered significant, surveillance may be preferred initially (7). The recommended surgical procedure for an epidermoid cyst of the buttock depends on several factors, such as the size and location of the lesion, as well as the experience and preference of the surgeon. The treatment of choice for squamous cysts total resection of the tumor including the cyst capsule that produces the cyst contents (8). But sometimes, total resection is not possible because of the location of the cyst and its close relationship with critical nerve or vascular structures. In this case, part of the capsule is left in place with a high risk of recurrence (9).
The diagnosis is essentially established by histopathological examination, which objectifies the tumor as a "pearly" tumor because of its pearly white color and nipped appearance (10). The differential diagnosis is essentially with its rarer dermoid cyst counterpart, which usually does not have the milky white appearance so characteristic of its epidermoid counterpart. It is more variable, more heterogeneous, due to the diversity of the Several studies have examined the outcomes of surgical excision for epidermoid cysts of the buttock, with high success rates and low recurrence rates (11). One study reported a $98\%$ success rate for surgical excision of epidermoid cysts of the buttock, with a recurrence rate of only $1\%$ (12). Another study reported a success rate of $95.8\%$ with a mean follow-up of 31 months (13).
## IV. CONCLUSION
Epidermoid cyst of the buttock is a rare benign tumor, whose diagnosis established by imaging and confirmed by histopathological examination. Epidermoid cysts are treated surgically, with complete resection of the tumor and its capsule, if possible. Follow-up is necessary to monitor for recurrence, although this is rare. Surgeries have a high success rate and are considered the treatment of choice for squamous cysts of the buttock.
### Consent
Written informed consent was obtained from the patient for publication of this case and for the accompanying images.
### Ethical Approval
As per international standard or university standard written ethical approval has been collected and preserved by the author(s).
1. Choon Soo Kim, Young Cheon Na, Chi Sun Yun, Woo Hoe Huh, and Bo Ra Lim: Epidermoid cyst: A single-center review of 432 cases. Arch Craniofac Surg. 2020 Jun; 21(3): 171-175.
- single-center review of 432 cases Arch Craniofac Surg. 2020 Jun; 21(3): 171-175.
2. Denison CM, Ward VL. Epidermal inclusion cysts of the breast: Three lesions with calcifications. Radiology. 1997; 204: 493-496.
3. Fujimoto T, Murakami K, Kashimada A. Large epidermoid cyst involving the ischiorectal fossa: MR Demonstration. Clin Imaging. 1993; 17: 146-148.
4. Handa U, Chhabra S. Epidermal inclusion cyst: Cytomorphological features and differential diagnosis. Diagn Cytopathol. 2008; 36: 861-863.
5. Momeni MG, Anavim A. Giant epidermal inclusion cyst of buttock. Skeletal Radiol. 2006; 35: 864-866.
6. Shibata T, Hatori M. Magnetic resonance imaging features of epidermoid cyst in the extremities. Arch Orthop Trauma Surg. 2003; 123: 239-241.
7. Patel K, Bhuiyu T. Epidermal inclusion cyst of phalanx: A case report and review of the literature. Skeletal Radiol. 2006; 35: 861-863.
8. Weedon D. Weedon's skin pathology. 3rd Edition. Elsevier;
2010. pp. 442-446.
9. Hong SH, Chung HW. MRI findings of subcutaneous epidermal cysts: Emphasis on the presence of rupture. Am. J. Rotengenol. 2006; 186: 961-966.
10. Bauer BS, Lewis VL., Jr. Carcinoma arising in sebaceous and epidermoid cysts. Ann Plast Surg. 1980; 5: 222-226.
11. Lin CY, Jwo SC. Squamous cell carcinoma arising in an epidermal inclusion cyst. Chang Gung Med J. 2002; 25: 279-282.
12. Pandya KA, Radke F. Benign skin lesions: Lipomas, epidermal inclusion cysts, muscle and nerve biopsies. Surg Clin North Am. 2009; 89: 677-687. [PubMed] [PubMed] [Google Scholar]
13. Tokunaga M, Toya M, Endo Y, Fujisawa A, Tanioka M, Kato M, Miyachi Y: A case of an undifferentiated squamous cell carcinoma arising from an epidermal cyst. Case Rep Dermatol Med. 2013, 2013: 469516. 10.1155/2013/469516
Generating HTML Viewer...
References
13 Cites in Article
Choon Soo,Kim,Young Cheon Na,Chi Sun Yun,1 Woo Hoe,Bo Huh,Lim (2020). Epidermoid cyst: A single-center review of 432 cases.
C Denison,V Ward,S Lester,P Dipiro,D Smith,J Meyer,T Frenna (1997). Epidermal inclusion cysts of the breast: three lesions with calcifications..
T Fujimoto,K Murakami,A Kashimada (1993). Large epidermoid cyst involving the ischiorectal fossa: MR Demonstration.
Uma Handa,Seema Chhabra,Harsh Mohan (2008). Epidermal inclusion cyst: Cytomorphological features and differential diagnosis.
M Momeni,A Anavim (2006). Giant epidermal inclusion cyst of buttock.
Tsunehiro Shibata,Masahito Hatori,Takashi Satoh,Shigeru Ehara,Shoichi Kokubun (2003). Magnetic resonance imaging features of epidermoid cyst in the extremities.
Keyur Patel,Tawfiqul Bhuiya,Sheng Chen,Samuel Kenan,Leonard Kahn (2006). Epidermal inclusion cyst of phalanx: a case report and review of the literature.
D Weedon (2010). Weedon's skin pathology.
Sung Hong,Hye Chung,Ja-Young Choi,Young Koh,Jung-Ah Choi,Heung Kang (2006). MRI Findings of Subcutaneous Epidermal Cysts: Emphasis on the Presence of Rupture.
B Bauer,V Lewis,Jr (1980). Carcinoma arising in sebaceous and epidermoid cysts.
C Lin,S Jwo (2002). Squamous cell carcinoma arising in an epidermal inclusion cyst.
M Tokunaga,M Toya,Y Endo,A Fujisawa,M Tanioka,M Kato,Y Miyachi (2013). A case of an undifferentiated squamous cell carcinoma arising from an epidermal cyst.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Yousra Ouhammou. 2026. \u201cDiagnostic and Therapeutic Approach to Epidermoid Cysts in the Gluteal Region: A Rare Case and Review of the Literature\u201d. Global Journal of Medical Research - F: Diseases GJMR-F Volume 23 (GJMR Volume 23 Issue F5): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.