


I. INTRODUCTION
Obesity is a roaring global concern with a sprouting predominance in children (Ogden, Carroll, Kit, & Flegal, 2014), adolescents, and older people on the earth, especially in a developing country. The number of obese people also has expanded day by day in an epidemic manner throughout the last decade. It was accounted that the prevalence rate of obesity and central obesity varies from to and , respectively according to ICMR-INDIAB study 2015, (Ahirwar & Mondal, 2019). Obesity is characterized by the exorbitant gathering of fat, especially adipose tissues, which can adversely influence well-being by expanding the expression of pro-inflammatory markers (Huang, Zhang, & Chen, 2016). Due to the accumulation of excessive adipocytes, various health consequences such as increased heart disease, hypertension, diabetes, inactivity, inflammation, genetic alteration, stroke, and cancer (Aronne, 2001) occur. Some of these medical comorbidities are associated with adverse cognitive effects (Biessels, Deary, & Ryan, 2008). There is a strong correlation between obesity and neurodegenerative diseases, suggesting that obesity might affect the central nervous system, causing neurodegeneration and cognitive decline, as well as causing brain damage (Ashrafian, Harling, Darzi, & Athanasiou, 2013). Neurodegenerative disease (ND) is a significant reason for inability, morbidity, and diminished personal satisfaction, establishing the basis for of human death internationally (Erkkinen, Kim, & Geschwind, 2018). Investigations have shown that individuals who experience the ill effects of midlife obesity (estimated by BMI) have an expanded danger to building Alzheimer's Disease (AD) and Parkinson's Disease (PD) (Profenno, Porsteinsson, & Faraone, 2010). The role of obesity in memory and cognitive decline has been reviewed in this article.
II. EFFECT OF OBESITY ON BRAIN STRUCTURE AND COGNITIVE CAPACITY
a) Brain Structure
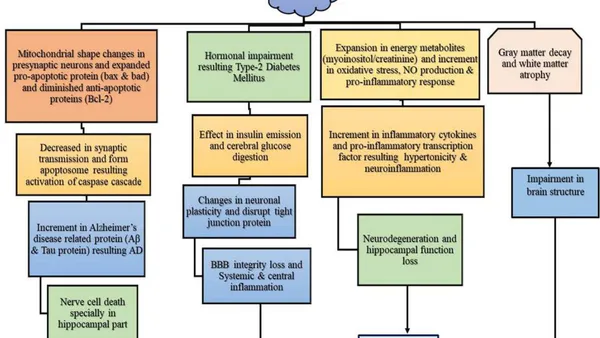
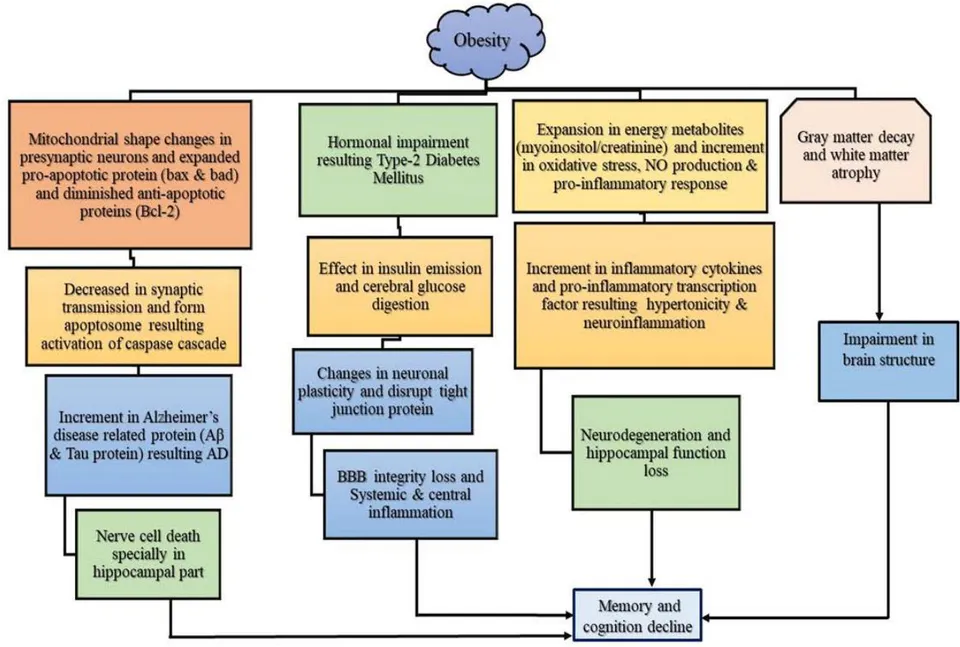
Structure alteration in neural architecture due to obesity has been recently reported. For instance, raised BMI is connected to diminished cerebrum volume (Ward, Carlsson, Trivedi, Sager, & Johnson, 2005), the autonomy of age, and morbidity (Gunstad et al., 2008). Expanded BMI is connected with gray matter decay in some specific parts of the brain (Shefer, Marcus, & Stern, 2013), and decreased uprightness of white matter of the brain (Verstynen et al., 2012). Middle-age must be the most critical period for brain aging and at that time, vulnerability to obesity is particularly acute compared with later life (Ronan et al., 2016), and the starting of middle-age, there has been identified white matter atrophy (Fotenos, Snyder, Girton, Morris, & Buckner, 2005) in the brain. Recently, Thompson et al. (2020) conducted a meta-analysis where the connection between obesity and brain structure of 6420 members was studied. Obesity has been shown to be associated with brain structure abnormalities, including a lowered temporal-frontal thickness. Cortical thinning of the brain might be related to decreased microstructural integrity in white matter tracts in obese teenagers (Yau et al., 2014). Further, obesity decreases practical movement in cortical regions that are associated with episodic memory (hippocampus, dorsolateral prefrontal cortex, and angular gyrus) (Cheke, Bonnici, Clayton, & Simons, 2017). Obesity also causes an increase in the amount of glycerol, hormones, cytokines, and pro-inflammatory substances involved in developing insulin resistance (Al-Goblan, Al-Alfi, & Khan, 2014). The hippocampus might be especially helpless against the adverse consequences of abnormal glucose tolerance and insulin resistance comparative with other cerebrum districts, a suggestion supported by neurological, structural research associating type 2 diabetes and impaired glucose tolerance (IGT) with hippocampal atrophy (Bruehl et al., 2009; Gold & Shadlen, 2007; Korf, White, Scheltens, & Launer, 2006). Expanded development of harmful glycation end product results in hyperglycemia and type 2 diabetes (Roriz-Filho et al., 2009), this could result in hippocampal volume loss, especially given that the hippocampus is profoundly defenseless against other metabolic affronts (McEwen, 1997; Stranahan et al., 2008). Hippocampus has a high co-restriction of insulin and cortisol receptors (Jacobson & Sapolsky, 1991). It has been guessed that persistently raised corticosteroids related to type 2 diabetes could modify synaptic plasticity and explicit neurogenesis in the hippocampus (Magariños & McEwen, 2000). The conceivable clarification could be that peripheral insulin resistance results in expanded hepatic lipid production, especially in ceramides, a product from unsaturated fats and sphingosine and is known to have lipid solvent properties(Tong & de la Monte, 2009). A few studies have shown that ceramide promotes brain insulin resistance through an impaired brain insulin pathway (Arboleda, Morales, Benitez, & Arboleda, 2009), and results in neurodegeneration as a consequence (Arboleda et al., 2009; Sartorius et al., 2014; Tong & de la Monte, 2009). Even though there was no proof that ceramide straightforwardly results in blood-brain barrier disturbance, it is conceivable that a lot of ceramides under obese conditions might be one of the dangerous elements to cause the interruption of the blood-brain barrier. In this way, the blood-brain barrier can be crossed (Fig. 1).
b) Cognitive and memory impairment
After different longitudinal and cross-sectional investigations, researchers considered that obesity in early adulthood or middle age could extend one's risk of later-life cognitive inability. People who had higher BMI in midlife displayed shortages in an assortment of mental spaces, including long-and short memory, psychomotor speed, verbal capacity, and spatial capacity, this led to more fast destruction of cognition (Hassing, Dahl, Pedersen, & Johansson, 2010). An increased BMI, as well as increased energy metabolites (Roriz-Filho et al., 2009), result in worse memory performance by causing hypertonicity and neuroinflammation (Gonzales et al., 2012). Numerous studies have shown that the "Western diet", which is high in saturated fats and simple sugars, impairs learning and memory in people who are obese (Beilharz,
Maniam, & Morris, 2015; Loprinzi, Frith, Edwards, Sng, & Ashpole, 2018). It is associated with decreased neurogenesis and increased inflammatory responses. As it is also shown, diet plays a vital role in such memory impairments, as opposed to being caused by adipose changes, and the brain's working memory and negative outcome learning capacity are hampered due to adaptations in the dopamine system due to obesity-induced overeating. (Coppin, Nolan-Poupart, Jones-Gotman, & Small, 2014).
BBB is mainly made up of endothelial cells. However, obesity is a cause of endothelial brokenness, adding to BBB deterioration through some mechanisms (Wardlaw et al., 2013). This results obesity-related cognitive impairments, initiates neuroinflammation and neurodegeneration. Disturbance in the tight junction of endothelium breakdown the BBB (Zlokovic, 2008) proposes that obesity might trigger tight junction interruption prompting BBB breakdown. The disruption of BBB by lipid-like substances results in microglial activation, decreased endothelial tight junction and protein articulation (Shigemoto-Mogami, Hoshikawa, & Sato, 2018; Sumi et al., 2010), ultimately leading to persistence neuroinflammation (Dalvi et al., 2017; Thaler et al., 2012) and cognitive dysfunction (Kahn & Flier, 2000). In like manner, (Bocarsly et al., 2015) announced that obesity prompted decreases in dendritic spines and led to cognitive decline. It has been shown from different findings that obesity is associated with systemic and central inflammation (Gregor & Hotamisligil, 2011; Miller & Spencer, 2014) and is always hindering memory and cognition by stimulating the production of pro-inflammatory cytokines and adipokines that lead to insulin resistance (Su et al., 2017). De Souza and partners found that high-fat diets or obesity raises the pro-inflammatory cytokines and the pro-inflammatory transcription factor NF B in the hypothalamus (De Souza et al., 2005). The hippocampus, a significant area in cognitive preparing, learning, and memory, might be especially defenseless against inflammation in obesity, with raised TNF- and ionized calcium-binding connector particle 1 (Iba1; microglial marker) (Jeon et al., 2012). Hence, this concluded that systemic inflammation and obesity have been recognized as the leading cause of cerebral white matter injuries and cognitive brokenness (T Den Heijer et al., 2005; Viscogliosi, Donfrancesco, Palmieri, & Giampaoli, 2017). In addition, higher plasma levels of interleukin (IL)-12 and 6 are connected to diminished speed in handling data and a quicker pace of cognitive decay (Marioni et al., 2010; Schram et al., 2007; Trollor et al., 2012). Hypertension expands one's danger of being diagnosed to have mild cognitive impairment (MCI) (Reitz, Tang, Manly, Mayeux, & Luchsinger, 2007). It predicts the degree of weakness seen in these people (Goldstein, Levey, & Steenland, 2013). Obesity-induced hypertension in midlife is conversely identified with execution on an assortment of cognitive tests, for example, those verbal surveying memory and executive function during obesity (M. Elias, Elias, Sullivan, Wolf, & D'agostino, 2003; Launer, Masaki, Petrovitch, Foley, & Havlik, 1995). Past research has shown that mitochondria assume a crucial part in cerebrum synaptic transmission and age-related intellectual capacity (A. Cheng, Hou, & Mattson, 2010; Hara et al., 2014; Mattson, Gleichmann, & Cheng, 2008; Raefsky & Mattson, 2017). That study suggested that changes in the shape of mitochondria in presynaptic neurons affected synaptic transmission. Additionally, apoptosomes are formed that activate the caspase cascades and subsequently trigger cell death(Cain, Bratton, & Cohen, 2002). Research has shown increased level of pro-apoptotic proteins (Bax and Bad) in brain tissue from rodents with insulin resistance caused by mitochondrial impairment, along with reduced levels of anti-apoptotic proteins (Bcl-2) (Nuzzo et al., 2015; Sa-Nguanmoo et al., 2017; Sa-Nguanmoo et al., 2016). An increment in pro-apoptotic proteins can prompt cytochrome C release, bringing about cerebrum apoptosis (Gómez-Crisóstomo, López-Marure, Zapata, Zazueta, & Martínez-Abundis, 2013). Also, apoptotic-mediated neuronal passing has been known to be one fundamental component for intellectual weakness and other neurodegenerative infections and cognitive loss (Ghavami et al., 2014).
III. OBESITY AND DEMENTIA
As populaces age, intellectual problems, including dementias, become more normal. The most common form of dementia is Alzheimer's disease (AD), representing somewhere in the range of half and of all dementias. Ongoing efficient reviews and metaexaminations uncover an unpredictable connection between obesity and the possibility of dementias (Anstey, Cherbuin, Budge, & Young, 2011; Beydoun et al., 2011; Gorospe & Dave, 2007). The conviction of dementia being a solitary memory-related confusion of Alzheimer's disease (AD) has tremendously congested. The present comprehension of dementia is a complete loss of memory with diminished mental and scholarly execution because of damaged synapses. The current existing research on BMI and AD is conflicting and consolidating the consequences of many investigations that exhibited a lot of conflicting data. A meta-examination done on 16 articles covering 15 planned investigations showed that underweight, overweight, and obesity in midlife is related to an expanded danger of dementia when contrasted with having normal weight or BMI. Having a raised BMI in midlife altogether expands the danger of dementia perhaps because of expanded inflammation, higher cytokine, and hormone created by fat tissues (Skoog & Gustafson, 2003). Having an expanded BMI can likewise be related to countless morbidities, for example, insulin opposition prompting diabetes, elevated cholesterol, hypertension, and cardiovascular infection (Naderali, Ratcliffe, & Dale, 2009). The vascular impacts may likewise play a part in advancing a quickly developing disease of late-life, Alzheimer's pathology. Additionally, the variables mentioned above and the higher BMI is link with the changes in cerebrum structure, white matter changes, blood-brain obstruction aggravations, and the age-related administrative changes in protein, carbohydrate, and lipid digestion that might trigger dementia pathology. The persistent overconsumption of food sources wealthy in carbohydrates and lipids in obesity can influence insulin emission and fundamentally affects cerebral glucose digestion. The normal intracellular components in type 2 Diabetes Mellitus and AD incorporate variant redox guidelines, oxidative pressure, and dynamic incendiary cycles bringing about disabled insulin emission and signaling pathways(Verdile et al., 2015). Studies have shown that central insulin organization may be powerful in helping people with Alzheimer's to perform cognitively (Claxton et al., 2015; Freiherr et al., 2013; Haj-Ali, Mohaddes, & Babri, 2009).Further evidence suggests insulin may influence AD-related proteins (e.g., APP and tau) and contribute to the progression of AD pathology and cognitive impairment (Ferreira, Clarke, Bomfim, & De Felice, 2014; Steculorum, Solas, & Brüning, 2014; Umegaki, 2014). The T2DM has a particularly damaging effect on the hippocampus - a part of the brain crucial for memory and learning functions (Bruehl et al., 2009; Tom den Heijer et al., 2003; Gold & Shadlen, 2007; Korf et al., 2006). Though diabetes is not just a danger factor for mild cognitive impairment (MCI) and Alzheimer's disorder yet in addition to some other kinds of dementia (G. Cheng, Huang, Deng, & Wang, 2012). Obesity can likewise initiate endothelial brokenness and cause cerebral hypoperfusion and improve the creation of -amyloid that will general, diminish endothelial capacity further, making an endless loop prompting pathogenic changes of AD. This endothelial brokenness is because of a diminished combination and activities of nitric oxide (NO) from the endothelium and expanding the development of oxidative pressure. Increasing levels of deviated dimethylarginine inhibit NO synthase activity, resulting in cerebral hypoperfusion and mental and neurodegenerative changes in AD (Toda, Ayajiki, & Okamura, 2014). In addition to the and Tau proteins causing AD, many factors are also a contributing factor to this disease (Alves, Correia, Miguel, Alegria, & Bugalho, 2012) including mitochondrial impairments, ROS generation, oxidative damage, proinflammatory responses, energy utilization impairments, and failure in various neurotransmission systems(Cai, Zhao, & Ratka, 2011; Ferrer et al., 2012). The gut-brain axis, also known as the gut-microbiota interaction, has also been suggested to be important in the utilization of high fat diets and other imbalanced eating plans that hinder perception (Solas, Milagro, Ramírez, & Martínez, 2017). Notably, cognitive execution and markers of cerebrum decay like whole brain and hippocampal volumes are amazing indicators of intellectual decrease and dementia in everyone (Amiya et al., 2005; M. F. Elias et al., 2000; Jack et al., 2005). In this manner, obesity-related degradation might intensify the danger for dementia and a cognitive decrease by synergistically associating with the maturing system. Predictable with this idea, higher BMI is associated with cerebrum degradation in patients determined to have AD (Abilés et al., 2010). Besides, there is proof that midlife obesity is related to an expanded pace of aggregate and hippocampal brain degradation and cognitive decrease ten years after the fact (Debette et al., 2011) and finally, cases of neurodegenerative disease. AD and PD are two main neurodegenerative diseases characterized by
the accumulation of abnormal protein in the brain, results in a neuronal loss (Gaeta & Hider, 2005) and causes cognitive impairment.
IV. SUMMARY AND CONCLUSION
As a result of the systematic frame introduced in this review, we can now understand how obesity leads to brain changes that can result in cognitive impairment. As In addition to inflammation, hyperinsulinemia/insulin resistance, interruption of oxidative stress, and neurodegenerative diseases, obesity has been associated with cognitive impairment. It can therefore be concluded that obesity-induced structural changes in the brain, impaired mitochondrial function, insulin resistance and blood-brain barrier are major contributors to memory impairment.
Abbreviations: AD (Alzheimer's Disease), PD (Parkinson's Disease), ND (neurodegenerative disease), BMI (basal metabolic rate), BBB (blood-brain barrier), T2DM (Type 2 diabetes mellitus), MCI (mild cognitive impairment), NF (nuclear factor ), TNF- (Tumour Necrosis Factor- ), IL-12 (interleukin-12), (amyloid ).



