Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder that involves a series of behavioral aspects. Individuals with ASD have atypical development in the areas of learning, communication, social interaction, detection and handling of emotions, motor coordination and concentration. They may also have difficulty thinking flexibly and dealing with changes. With the advancement of information and communication technologies, an alternative used to assist in treating these children is the brain-computer interface (BCI). In this context, this article aimed to create a mental game controlled via ICC that would enable the monitoring of brainwave behavior and promote an improvement in the cognitive performance of children with ASD. To this end, a mixed methods experimental study was carried out with a sample of 21 children aged 9 to 11 years. The study was carried out in schools in the city of Fortaleza -Brazil. The children in the Experimental Group (EG) were exposed to a game that involved memorizing images to develop and improve reasoning by creating relationships between the images and the sequence of arranged cards.
## I. INTRODUCTION
The right to education must be ensured for every child, especially those with disabilities, a group historically excluded from the educational process. Through advocacy for rights and acknowledgment of their human dignity, the disability rights movement has progressed and gained recognition in society. During these efforts, autism has emerged as a prominent focus.
Autism Spectrum Disorder (ASD), as defined by the American Psychiatric Association - APA (2014), is a neurodevelopmental disorder involving various behavioral aspects with enduring psychosocial implications. It is characterized by limitations in social interaction and communication, specific interests, and restricted behavioral patterns, as noted by Teo et al. (2021).
Casanova et al. (2021) underscore the challenges faced by individuals with autism in organizing thoughts and executing communication, leading to social isolation. They emphasize the need for support in the teaching and learning process, underscoring that knowledge can become abstract for individuals with disabilities, including those with ASD. This underscores the importance of using materials and methodologies that facilitate access to learning.
Research suggests that digital technology presents an opportunity to enhance the quality of education by providing new avenues for teaching and learning, along with innovative methodologies. Digital games, designed as innovative alternatives, indicate that these systems can become adequate resources in meeting the specific needs of individuals with ASD (COELHO NETO et al., 2017).
An alternative employed to assist in the treatment of children with ASD is the Brain-Computer Interface (BCI). It involves an external device placed on the user's head to monitor brain activities and facilitate interaction through neurofeedback (BASTOS, 2020; Marçal et al., 2023).
According to Dias (2010), neurofeedback is an operant conditioning modality to re-establish appropriate electrophysiological patterns for treating certain neurological, psychiatric, or psychological disorders. It enhances normal cognitive abilities and promotes a sense of well-being. In neurofeedback treatment, the patient's brain activity is measured using Electroencephalography (EEG), and the neural wave data can be processed and analyzed in real-time. EEG records the amplified electrical impulses responsible for the body's activities, transmitted as brain commands through neurons (BASTOS, 2020).
As an option to contemporary traditional treatments, neurofeedback therapy stands out for its innovative, non-invasive nature without using medications. Research indicates benefits such as the reorganization of the brain's functional network from regular to more random configurations, improved focus and mental concentration, highly successful results in attention, and gains in social and self-control skills (COSTA et al., 2021; Mota et al., 2023). Literature highlights the advancing use of Brain-Computer
Interfaces in clinical and diagnostic contexts, showing possibilities for educational applications (CAVALCANTE et al., 2020; MARÇAL et al., 2022).
Recently, BCIs have been integrated into fields such as education, including computer interface design, games, and research in neuroeducation (BOS et al., 2019). While brain wave analysis is highly advanced in the clinical setting, it remains underexplored in environments like the classroom (AMARAL et al., 2017; CARELLI et al., 2017; FAN et al., 2017; ARPAIA et al., 2020).
In this context, this article aims to describe the development and evaluation of a digital game controlled via BCI that allows monitoring of brain wave behavior and promotes improved cognitive performance in students with ASD: the MemoTea[^1]. It involved a multidisciplinary team of professionals, including a psycho-pedagogue, neuropsychologist, statistician, and information technology professionals.
The game's scenario focused on hygiene and health due to its significance as a public health issue that enhances individuals' autonomy in caring for their bodies, a challenge often faced by children with autism (CASANOVA et al., 2021). This theme is of utmost importance and is addressed in Brazil's National Common Curriculum Base (BNCC), which aims to explore the reasons why maintaining body hygiene habits is essential for overall health (BRASIL, 2017).
## II. METHODOLOGY
This article presents a descriptive study using an experimental mixed-methods approach (qualitative-quantitative). This approach involves collecting and analyzing qualitative and quantitative data, integrating information within an experiment or intervention that combines qualitative data collection with pre and post-test experimental interventions (CRESWELL; CRESWELL, 2021, p.189).
The study focused on students diagnosed with Autism Spectrum Disorder (ASD), enrolled in the elementary school (early years, 1st to 5th grade) of the municipal network of Fortaleza - CE. Participants were randomly and voluntarily selected, meeting the necessary criteria for participation. The study included 21 children between the ages of 9 and 11, who were divided into two groups: the experimental group $(n = 11)$ and the control group $(n = 10)$.
Data collection took place from March 2023 in the Multifunctional Resource Rooms (MRR) of public schools in Fortaleza, Brazil, with autistic students enrolled in the Specialized Educational Assistance (SEA) program. Academic research authorization in the Fortaleza Municipal Network required administrative processing through the Municipal Education Secretariat (MES) and approval from the Research Ethics Committee (REC).
The research was authorized by the Municipal Secretary of Education (MSE) through the Academic Research Authorization Term, under administrative process no. P011111/2023, registered on Plataforma Brasil under substantiated opinion no. 6.024.525 (Research Ethics Committee).
As this study involves individuals, particularly minors, parental or guardian consent was obtained through the Free and Informed Consent Form (FICF), allowing the participation of the minor under their responsibility. Additionally, children signed the Free and Informed Assent Form (FIAS), both explained and provided by the researcher during the signing process.
A semi-structured interview (anamnesis) with guardians was conducted to investigate relevant aspects of the participants' lives, providing insights into their personal and clinical history. Subsequently, a neuropsychological test was administered to all participants in the experimental group $(n = 11)$ and the control group $(n = 10)$ to assess their cognitive levels.
The applied neuropsychological test was the SON-R 6-40 (LAROS et al., 2022), a non-verbal instrument for assessing general intelligence. It consists of four subtests: Categories and Situations (reasoning subtests) and Mosaics and Patterns (execution subtests). It suits individuals with hearing difficulties, language problems, developmental disorders, and immigrants. However, only the analogies, categories, and mosaics subtests were applied due to time constraints and their relevance to this study's objectives.
The BCI was validated and used exclusively with children in the experimental group $(n = 11)$. During the validation process, children engaged in the MemoTea game, focusing on memorizing images to enhance reasoning, concentration, and logical thinking.
Finally, the neuropsychological test was reapplied to all participants in both groups to analyze the results and their relationship with the use of BCI in improving cognitive abilities and personal hygiene in children with ASD. It is essential to note that neuropsychological tests were conducted with the assistance of psychology undergraduate students and a neuropsychologist.
The research took place in the multifunctional resource rooms of schools, with support from the Specialized Educational Assistance (SEA) teacher. These rooms are equipped with furniture, educational materials, and resources for specialized educational assistance (BRAZIL, 2011).
A semi-structured interview (anamnesis) with the child's guardian was conducted. The researcher explained the entire process to the participant and their legal guardian. Afterward, both the experimental group $(n = 11)$ and the control group $(n = 10)$ of children underwent a neuropsychological test at the start and conclusion of the monitoring period.
The experimental group $(n = 11)$ participated in sessions using the BCI platform twice weekly, each lasting 30 to 40 minutes. Before each session, participants received instructions on the game and the Brain-Computer Interface's functioning. The ICC was configured and calibrated for each participant at the beginning of each session. Each participant underwent an average of eight weeks of training, comprising 16 sessions each. In the end, the researcher, in collaboration with a neuropsychologist, analyzed the test data (Figure 1).
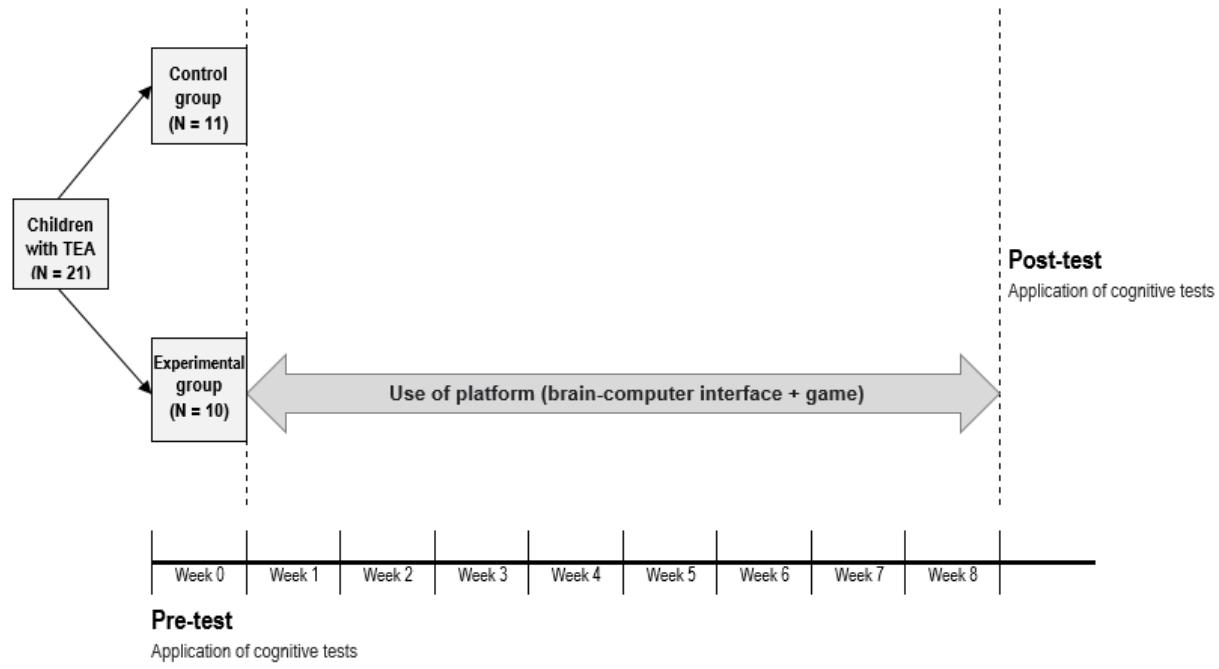 Source: Prepared by the authors (2023) Figure 1: Research Design
After the Experimental Group (EG) members participated in ICC sessions, both groups (Control Group - CG and Experimental Group - EG) underwent the neuropsychological test again. The obtained results were analyzed using Hotelling's $T^2$ parametric test (Nel and Merwe, 1986), a non-parametric ANOVA test, and two marginal tests (univariate): the Welch's parametric t-test and the non-parametric Wilcoxon test. Statistical analyses were conducted according to conventional scientific methodologies.
## III. RESULTS AND DISCUSSION
This section presents the study results, divided into three subtopics: the digital game presentation, description of skills highlighted in the neuropsychological test, and evaluation and analysis of MemoTea game impact concerning BCI use.
### a) Presentation and Usage of the Digital Game
This study focuses on 'MemoTea,' a digital memory game that explores themes related to hygiene and health. It was developed to enhance the cognitive performance of children diagnosed with Autism Spectrum Disorder (ASD) and improve their understanding of personal hygiene. Barasoul (2022) notes that memory games are widely used due to their connection to audiovisual material, fostering visual discrimination, logical thinking, identification, and association of images and words, among other aspects.
A literature review was conducted to understand the researched theme and identify the requirements for developing a digital game using BCI for children with autism. GAIA (Guide for Accessibility of Web Interfaces focused on Autism aspects) stood out, offering 28 recommendations to aid software developers and digital educators in creating websites suitable for children within the autism spectrum (BRITTO, 2016).
Schell (2019) was selected as a starting point for product development due to his relevance in the game design field. The author presents a set of questions called "lenses." For this study, the following lenses were focused on: lens #2, essential experience; lens #4, surprise; lens #7, endogenous value; lens #8, problem-solving; and lens #9, elemental tetrad. The game design was developed based on the identified requirements (see Figure 2).
#### GAME IMPACT:
Improving the concentration, memory, and logical reasoning skills of the player over time.
#### GAME CONCEPT
Objective: Achieve a higher score by finding correlated pairs of cards related to hygiene habits necessary for maintaining health.
Genre: Puzzle puzzle
#### PLAYER PROFILE
Community: Children with Autism Spectrum Disorder (ASD).
Age: 9 to 11 years
Number of players: 1
#### GAME MECHANICS
Loss condition: Lose lives when failing to match card pairs and exceeding the 20-minute time limit.
Special rule: Use concentration and blinking to select and flip the cards.
Space: Pairs of cards increasing in quantity every two levels and an image of a child with an arrow indicating the concentration state.
Challenge: Complete the 7 (seven) levels, matching correlated pairs, losing the minimum number of lives, and achieving a higher score.
#### GAME CORE
Effects: Sounds emitted when cards are matched or mismatched and when advancing to the next level.
Restrictions: Start the game only after calibration and when focused.
#### GAME INTERACTION
Controls: Use the Brain-Computer Interface (BCI) with two inputs: concentration and blinking.
Platform:PC
Settings: Open BCI Software
#### GAME FLOW
Gameplay: Geared towards children with Autism Spectrum Disorder (ASD).
Random element: 9 to 11 years
Skill challenges: Concentration, memory, and logical reasoning.
Source: Adapted from Monteiro and Adamatti (2021).
Figure 2: Game Design
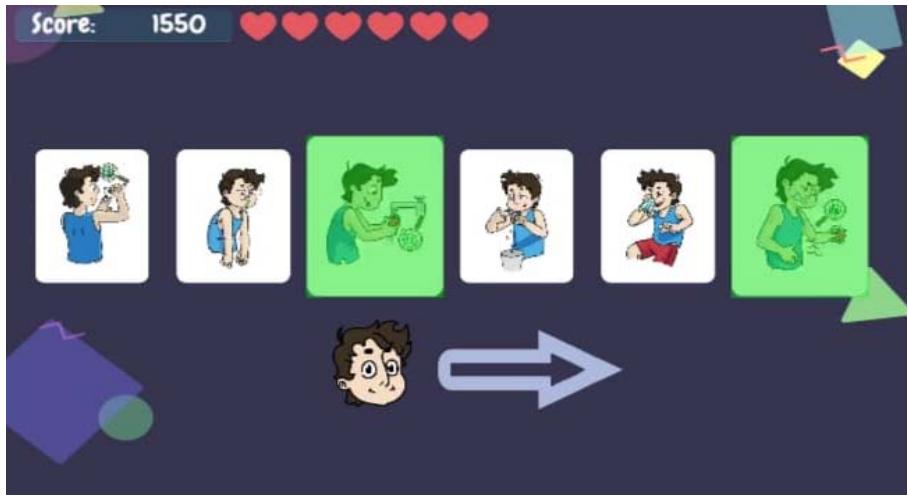
The game's objective is to match pairs containing illustrations of hygiene and health situations, such as a card showing risks of disease-causing agents (child with dirty and bare feet, toothless child, etc.)
paired with an image of the related hygiene habit (child wearing shoes, brushing teeth, etc.), as illustrated in Figure 3.
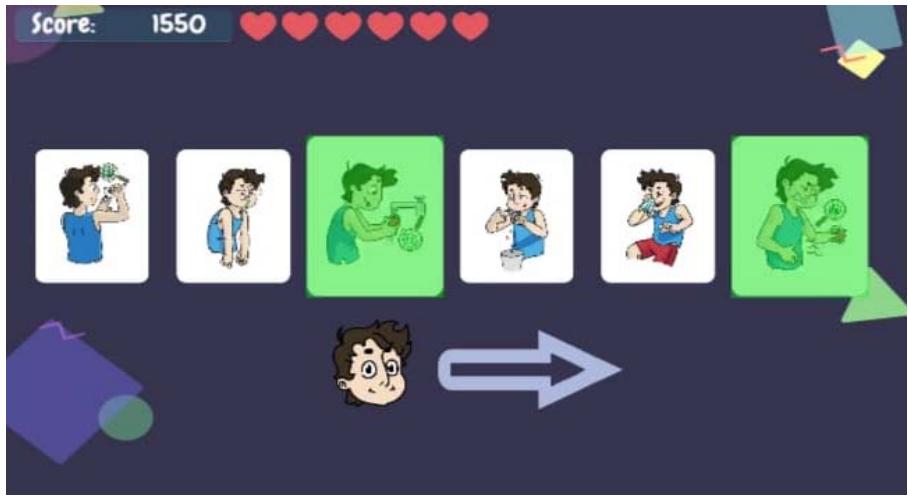 Figure 3: MemoTea Game
Source: Prepared by the authors (2023)
MemoTea consists of seven stages. The user initiates by moving an indicator through concentration captured via BCI. As the student concentrates, the indicator shifts between the game cards. When the indicator is on the desired card, the user should blink, sending a command to reveal the chosen card. Figure 4 displays a student playing MemoTea.
 Source: Prepared by the authors (2023). Figure 4: MemoTea Game Interface For each correct pair, the student earns points, and for each mistake, they lose "lives," indicated at the top of the screen. Concentration is essential for gameplay, monitored by a filled arrow in red. If the student loses concentration, the game pauses, resuming only when concentration is regained. All data, including errors and correct answers, concentration and distraction, scores, and game duration are stored.
The difficulty of the stages increases based on the number of cards. The first stage starts with two pairs, and the final stage has four pairs. At the end, participants can view their scores. The data collection system records the EEG data obtained by the BCI, allowing the entire session to be replayed.
Regarding field observations of student participation, there was significant interest and motivation in the activities. Initially, some individuals found it challenging to understand the correlation between pairs, even with explanations. However, as the game progressed, they understood and completed all stages. Most participants finished sessions before the allotted time (20 minutes), averaging between 15 and 18 minutes.
During sessions, differences were noticed among students despite all having an ASD diagnosis. Two students dropped out in the early sessions. They had to be replaced: one due to discomfort with the gel used on electrodes placed on the prefrontal part of the head and the other due to discomfort with the concentration indicator arrow.
### b) Evaluation and Analysis of Results and their Relationship with BCI Use
The study included 21 individuals diagnosed with ASD, aged between 9 and 11 years (Mean=10.16; Standard Deviation=0.77), with 11 individuals (Mean=10.33; Standard Deviation=0.60) allocated to the experimental group (EG) and ten individuals (Mean=9.98; Standard Deviation=0.92) to the control group (CG). The individual application test was composed of three subtests: Analogies (36 items divided into three series of 12); Mosaics (26 items divided into two series of 13); and Categories (36 items divided into three series of 12). The total IQ, representing overall cognitive functioning, was obtained from these subtests.
Everyone participated in three subtests (Analogies, Mosaics, and Categories) at the beginning of the experiment. The results of the subtests for the same individual may exhibit a correlation structure. Therefore, two multivariate tests were conducted to assess whether individuals behaved similarly in the initial administration of the subtests across groups, as per the results presented in Table 1.
The test was the parametric Hotelling's $T^2$ test, and the second was the non-parametric ANOVA-type test (Burchett et al., 2017). Two marginal (univariate) tests were conducted to assess the difference between EG and CG for each of the subtests and for the total IQ. These tests included the parametric Welch's t-test and the non-parametric Wilcoxon test. Both a parametric and a non-parametric test were considered to enhance the robustness of the study, as the sample sizes are not significant.
Table 1: P-values of Multivariate Tests for Independent Samples
<table><tr><td>Multivariate Tests for Independent samples</td><td>P-value</td></tr><tr><td>Hotelling's T2 Test</td><td>0.435</td></tr><tr><td>Non-parametric Anova tupe test</td><td>0.234</td></tr></table>
The null hypothesis for each of the two multivariate tests is: There is no difference between the groups when the tests are evaluated jointly, and the alternative hypothesis is: There is a difference between the groups when the tests are evaluated jointly. Considering that the p-values presented in Table 1 were more significant than 0.05, we can state that the null hypothesis should not be rejected, and the groups can be considered similar. To better understand the performance results in each subtest, marginal tests are presented in Table 2.
Table 2: Descriptive Statistics for Subtests and Total IQ in the Groups
<table><tr><td rowspan="2">Subtests</td><td colspan="3">EG (n=11)</td><td colspan="3">CG (n=10)</td><td rowspan="2">Difference</td><td colspan="2">P-value</td></tr><tr><td>average</td><td>DP</td><td>Amplitude</td><td>average</td><td>DP</td><td>Amplitude</td><td>Welch</td><td>Wilcoxon</td></tr><tr><td>Analogies</td><td>11.36</td><td>4.67</td><td>4 - 18</td><td>10.30</td><td>4.24</td><td>4 - 18</td><td>1.06</td><td>0.645</td><td>0.591</td></tr><tr><td>Mosaics</td><td>11.55</td><td>4.37</td><td>1 - 17</td><td>8.20</td><td>4.71</td><td>2 - 15</td><td>3.35</td><td>0.138</td><td>0.109</td></tr><tr><td>Categories</td><td>12.55</td><td>7.67</td><td>3 - 30</td><td>10.30</td><td>6.40</td><td>7 - 28</td><td>2.25</td><td>0.188</td><td>0.474</td></tr><tr><td>IQ</td><td>95.45</td><td>15.90</td><td>63 - 119</td><td>89.90</td><td>14.24</td><td>71 - 111</td><td>5.55</td><td>0.417</td><td>0.409</td></tr></table>
The null hypothesis in the eight marginal tests (one Welch test for each subtest and one Wilcoxon test for each subtest) is: There is no significant difference between the results of the subtests among the groups, and the alternative hypothesis is: There is a considerable difference between the results of the subtests among the groups. Considering that the p-values presented in Table 2 were all greater than 0.05, we can state that the null hypothesis should not be rejected, and the groups can be considered similar in each subtest.
It is observed that there is a slight performance variation in the experimental group, as indicated by the data in Table 2. However, this slight variation is insignificant as both test p-values are greater than
0.05 for each subtest, demonstrating no statistical significance between the groups.
After completing the sessions, the subtests Analogies, Mosaics, and Categories were readministered. The first statistical test applied to compare the results in the SON R-40 tests before and after sessions with the game was the paired Hotelling's T2 test (RENCHER, 2003). It is observed that the $T^2$ yielded satisfactory results, proving to be conservative under the proposed conditions, as demonstrated in Table 3, presenting p-values lower than the nominal value (0.05) for the general case (without group distinction) and for the experimental group, with a p-value exceeding 0.05 in the control group.
Table 3: P-values of Hotelling's ${\mathrm{T}}^{2}$ Tests for Paired Multivariate Data
<table><tr><td>Group</td><td>Hotelling's T2test for paired samples (p-value)</td></tr><tr><td>General (n=21)</td><td>0.005</td></tr><tr><td>Experimental Group (n=11)</td><td>0.004</td></tr><tr><td>Control Group (n=10)</td><td>0.194</td></tr></table>
A significant difference in the mean scores of the test application was observed, as indicated in Table 3, when comparing the control group and the experimental group. This also contributed to a change in the overall group mean (CG + EG). The results of 0.005 (general group) and 0.004 (experimental group) concretely express this improvement in performance. It is worth noting that the control group exhibits no discernible change in test performance.
Following the implementation of the multivariate paired test, two separate paired tests were carried out to evaluate cognitive improvements between the initial and subsequent test administrations within the Experimental Group (EG), Control Group (CG), and the overall groups, considering each subtest and the total IQ. These tests include the parametric Welch's t-test for paired samples and the non-parametric Wilcoxon test for paired samples. Additionally, the effect size of the
The mean differences was calculated using Cohen's d for paired samples. The effect size of mean differences for paired data was calculated using the formula for Cohen's d by Gibbons et al.(1993), incorporating the correction proposed by Borenstein et al.(2009). According to Cohen(1988), the effect size values should be interpreted as follows:$0.0 < |d| \leq 0.20 =$very weak effect;$0.20 < |d| \leq 0.50 =$weak effect;$0.50 < |d| \leq 0.80 =$moderate effect;$|d| \geq 0.80 =$strong effect.
effect; $0.20 < d| \leq 0.50 =$ weak effect; $0.50 < d| \leq 0.80 =$ moderate effect; $|d| \geq 0.80 =$ strong effect.
Table 4 presents these numbers based on two hypotheses: a) null hypothesis, where no difference occurred in values between administrations, and b) alternative hypothesis, where the difference was positive, indicating cognitive gain.
Table 4: Descriptive Statistics and P-values of Wilcoxon and Welch Paired Tests
<table><tr><td rowspan="2">Group</td><td rowspan="2">Subtestes</td><td colspan="2">Average</td><td colspan="3">Differenc (Post - Pre)</td><td colspan="2">p-value (paired samples)</td><td rowspan="2">Cohen's d (paired samples)</td></tr><tr><td>Pre</td><td>Post</td><td>Average</td><td>DP</td><td>Ampli</td><td>Wilcoxon</td><td>Welch</td></tr><tr><td rowspan="4">General (n=21)</td><td>Analogies</td><td>10.86</td><td>13.14</td><td>2.29</td><td>3.12</td><td>-2 9</td><td>0.0023</td><td>0.0016</td><td>0.4796 (weak)</td></tr><tr><td>Mosaics</td><td>9.95</td><td>10.14</td><td>0.19</td><td>2.42</td><td>-6 3</td><td>0.2438</td><td>0.3611</td><td>0.0412 (v. w.)</td></tr><tr><td>Categories</td><td>11.48</td><td>13.43</td><td>1.95</td><td>4.54</td><td>-10 10</td><td>0.0159</td><td>0.0315</td><td>0.2818 (weak)</td></tr><tr><td>IQ</td><td>92.81</td><td>99.10</td><td>6.29</td><td>7.52</td><td>-10 26</td><td>0.0008</td><td>0.0005</td><td>0.3827 (weak)</td></tr><tr><td rowspan="4">EG (n=11)</td><td>Analogies</td><td>11.36</td><td>14.82</td><td>3.45</td><td>2.70</td><td>0 9</td><td>0.0045</td><td>0.0008</td><td>0.6835 (mode)</td></tr><tr><td>Mosaics</td><td>11.55</td><td>11.18</td><td>-0.36</td><td>2.01</td><td>-3 3</td><td>0.7253</td><td>0.7187</td><td>-0.0837 (v. w.)</td></tr><tr><td>Categories</td><td>12.55</td><td>15.09</td><td>2.55</td><td>3.96</td><td>-3 9</td><td>0.0370</td><td>0.0294</td><td>0.3164 (weak)</td></tr><tr><td>IQ</td><td>95.45</td><td>103.73</td><td>8.27</td><td>7.48</td><td>-2 26</td><td>0.0029</td><td>0.0022</td><td>0.4048 (weak)</td></tr><tr><td rowspan="4">CG (n=10)</td><td>Analogies</td><td>10.30</td><td>11.30</td><td>1.00</td><td>3.16</td><td>-2 9</td><td>0.2607</td><td>0.1717</td><td>0.2370 (weak)</td></tr><tr><td>Mosaics</td><td>8.20</td><td>9.00</td><td>0.80</td><td>2.78</td><td>-6 3</td><td>0.1147</td><td>0.1933</td><td>0.1736 (v. w.)</td></tr><tr><td>Categories</td><td>10.30</td><td>11.60</td><td>1.30</td><td>5.25</td><td>-10 10</td><td>0.1195</td><td>0.2269</td><td>0.2254 (weak)</td></tr><tr><td>IQ</td><td>89.90</td><td>94.00</td><td>4.10</td><td>7.29</td><td>-10 13</td><td>0.0479</td><td>0.0546</td><td>0.2986 (weak)</td></tr></table>
Considering the data from the table above, we observe agreement between the paired Welch t-test and Wilcoxon test, indicating cognitive gain. However, it did not occur significantly, as the values remained below the threshold of $p = 0.05$. There is only one item in which Cohen's d showed a "moderate effect". This item corresponds to the Analogies subtest, representing the best performance result following the application of the sessions.
In this specific subtest (Analogies), the result is significant as it addresses areas of fluid intelligence development. In other words, there is notable progress in the cognitive processes of participants in the experimental group, which is the focus of the Brain-Computer Interface (BCI) intervention. The Analogies subtest addresses aspects related to abstract reasoning, including the ability to pay attention (observe), organize (process information), and plan (execute) actions. In the case of this subtest, participants identify the transformation process in a pair of figures and carry out the proposed transformation.
The other considered satisfactory result, even though it is not explicitly shown in the table when considering Cohen's d, pertains to the results of the Categories subtest: the mean value jumped from 12.55 to 15.09 after the intervention with the game and the BCI. This item also addresses reasoning ability, monitoring, and inhibition of inappropriate responses. It is worth noting that inevitably, aspects related to cognitive development are intertwined with socio-emotional aspects. An enhanced cognitive response or development implies an improvement in the development of emotional skills for children with ASD.
The presented results align with the primary aspects addressed in the MemoTea game, particularly concentration and logical reasoning (Analogies and Categories subtests). This is evident in the noticeable improvement in overall IQ performance, which increased from 95.45 to 103.73 in the experimental group (EG). The presented game aims to stimulate the concentration process by linking the child's perception of what is being asked in the game to their prompt response, such as "blink to select a card; concentrate on passing the card." These aspects are related to the development of fluid intelligence—the ability to identify and solve problems without prior knowledge. The game, therefore, incorporates elements related to reasoning and action execution: attention (perception of what is happening), concentration (the ability to focus, control impulses, and monitor—given as a possible response to a specific problem), and logical reasoning (the ability to associate images and shapes with previously seen items, also aiming to work on memorization).
The use of Brain-Computer Interface (BCI), mainly targeting the prefrontal cortex, aligns with the improvement in the performance of children in the experimental group—given that this brain region is one of the most affected in individuals diagnosed with Autism Spectrum Disorder (ASD) (Gomes et al., 2014). This clarifies the difficulties these individuals encounter in the brain's executive functions, although not all these functions are exclusively confined to this brain area.
Conversely, the less significant improvement in overall IQ can be attributed to Mosaics subtest results being notably lower. This justification is warranted as the subtest focuses on aspects related to spatial vision, a dimension not covered in this study.
## IV. CONCLUSION
This article presented the development and validation of a system to enhance cognitive performance by using a brain-computer interface-controlled digital memory game with 21 children with Autism Spectrum Disorder (ASD). Neuropsychological tests administered both before and after the use of the system (Game + BCI) revealed noteworthy cognitive improvements in the experimental group. Improvements were noted in concentration, logical reasoning, memorization, problem-solving, and increased self-confidence.
Furthermore, concerning the theme of hygiene and health, teachers reported observing some positive changes in students' behavior in the experimental group, such as acquiring the habit of handwashing or not removing footwear in the school environment.
It is worth noting that these improvements were observed and substantiated after only 16 sessions. Hence, there is a belief that extending the application of this solution (Game + Brain-Computer Interface) over a longer duration could potentially amplify cognitive benefits in this population.
Additionally, some improvements were noted that could be implemented in future tests, including the use of different games to help maintain students' interest and motivation, expanding the sample size to reinforce the confirmation of benefits achieved, conducting training in a more suitable physical environment to avoid external interferences, and employing procedures to minimize participant fatigue.
[^1]: The game was titled MemoTea, combining the Portuguese word 'MEMORIA' (in English, 'memory') and 'TEA' - Transtorno do Espectro Autista (in English, Autistic Spectrum Disorder). _(p.2)_
Generating HTML Viewer...
References
32 Cites in Article
Carlos Amaral,Marco Simões,Susana Mouga,João Andrade,Miguel Castelo-Branco (2017). A novel Brain Computer Interface for classification of social joint attention in autism and comparison of 3 experimental setups: A feasibility study.
Tito Sena (2014). Manual Diagnóstico e Estatístico de Transtornos Mentais - DSM-5, estatísticas e ciências humanas: inflexões sobre normalizações e normatizações.
Pasquale Arpaia,Carmela Bravaccio,Giuseppina Corrado,Luigi Duraccio,Nicola Moccaldi,Silvia Rossi (2020). Robotic Autism Rehabilitation by Wearable Brain-Computer Interface and Augmented Reality.
L Barbosa (2021). Contribuições das Neurociências à Educação.
R Bernier,G Dawson,J Nigg (2021). O que a ciência nos diz sobre o transtorno do espectro autista: fazendo as escolhas certas para o seu filho.
Andreia Bos,Milton Zaro,Lucas Prestes,Michelle Pizzato,Dario Azevedo,Flavio Avila,Marcelo Batista (2019). Student’s attention: The use of Brain Waves Sensors in Interactive Videos.
(2017). Base nacional comum curricular: educação é a base.
Brasil (2012). Institui a política nacional de proteção dos direitos da pessoa com Transtorno do Espectro Autista.
Talita Britto,Ednaldo Pizzolato (2016). GAIA: uma proposta de um guia de recomendações de acessibilidade de interfaces Web com foco em aspectos do Autismo.
L Carelli,F Solca,A Faini,P Meriggi,D Sangalli,P Cipresso,. Poletti,B (2017). Braincomputer interface for clinical purposes: cognitive assessment and rehabilitation.
S Casanova,K Franco,G Abrahão,V Lione,D Cavalcante,S Gomes (2021). Material didático adaptado para o ensino de Higiene e Saúde: Jogo da Memória Saudável para alunos com Transtorno do Espectro Autista (TEA).
R Costa (2023). Neurociência e aprendizagem.
J Creswell,J Creswell (2021). Projeto de pesquisa-: Métodos qualitativo, quantitativo e misto.
N Da Costa,E Marçal,M De Carvalho,T Barbosa (2021). Uso de interfaces cérebro-computador em crianças com TDAH: Uma revisão sistemática.
T De Araújo Cavalcante,J Soares,A Paiva,I Maia,P Benitez,A Soares (2020). Eye tracking como estratégia educacional inclusiva: avaliação com estudantes com autismo.
T De Araújo Alves,J Laros (2017). Adequação do SON-R 6-40 para pessoas com deficiência intelectual.
J Fan,J Wade,D Bian,A Key,Z Warren,L Mion,N Sarkar (2015). A Step towards EEG-based brain computer interface for autism intervention.
Jacob Laros,Gabriel Almeida,Felipe Valentini,Renata Lima (2015). Dimensionalidade e evidências de validade convergente do SON-R 6-40.
E Marçal,N Da Costa,C Menezes,A Júnior,L Sanders,K Queiroz,L Mota (2022). Neurofeedback e interface cérebro-computador: desenvolvimento e avaliação de um jogo voltado para o auxílio na detecção de TDAH.
E Marçal,M De Carvalho Barros (2023). Parecer A de “Search Engine Optimization como ferramenta estratégica na gestão da informação: primeiras perspectivas”.
Luana Mota,Carlos Menezes,Nayara Da Costa,Yanna Torres,Edgar Marçal (2023). Attention deficit disorder with hyperactivity: comparative analysis of executive functions between genres based on neurofeedback training.
Giulia Monteiro,Diana Adamatti (2021). Desenvolvimento de um Jogo Sério controlado por Neurofeedback para auxílio no tratamento de pessoas com TDAH.
Tatiana Mecca,Renata Lima,Jacob Laros,Elizeu Macedo,Rosane Lowenthal (2020). Autism Spectrum Disorders: Assessment of cognitive abilities using the non-verbal SON-R 6-40.
D Nel,C Van Der Merwe (1986). A solution to the multivariate Behrens-Fisher problem.
J Neto,M Blanco,M Guedes,C De Barbosa (2017). Autismo e Tecnologia: um mapeamento sobre as tecnologias para auxiliar o processo de aprendizagem.
Taila Pinheiro (2019). Os efeitos do treinamento de dupla tarefa na marcha e equilíbrio em pacientes com AVC: revisão sistemática.
E Non-Invasive Introduction to Non-Invasive EEG-Based Brain-Computer Interfaces for Assistive Technologies.
J Piaget,N Petit (1986). Seis estudios de psicología.
A Ojeda,J Laros (2021). SON-R 6-40: Dimensionalidade e Validade Convergente com a CMMS, TONI-3 e CPM.
M Relvas (2009). Fundamentos biológicos da educação: despertando inteligências e afetividade no processo de aprendizagem.
A Rencher (2005). A review of "methods of multivariate analysis.
Jesse Schell (2008). Tenth Anniversary: The Art of Game Design.
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Subject: Global Journal of Human-Social Science - G: Linguistics & Education
Authors:
Izabel Cristina Fernandes de Oliveira, Edgar Marçal, Carlos Eduardo de Souza Menezes, Rafael Bráz Azevedo Farias, Meline Mesquita de Carvalho (PhD/Dr. count: 0)
Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder that involves a series of behavioral aspects. Individuals with ASD have atypical development in the areas of learning, communication, social interaction, detection and handling of emotions, motor coordination and concentration. They may also have difficulty thinking flexibly and dealing with changes. With the advancement of information and communication technologies, an alternative used to assist in treating these children is the brain-computer interface (BCI). In this context, this article aimed to create a mental game controlled via ICC that would enable the monitoring of brainwave behavior and promote an improvement in the cognitive performance of children with ASD. To this end, a mixed methods experimental study was carried out with a sample of 21 children aged 9 to 11 years. The study was carried out in schools in the city of Fortaleza -Brazil. The children in the Experimental Group (EG) were exposed to a game that involved memorizing images to develop and improve reasoning by creating relationships between the images and the sequence of arranged cards.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.