A descriptor of life is a phase transition between order and chaos. Entropy is the physical property of this transition determining lifespan. Rules of maintaining entropy and a model of health and disease are presented simplifying scientific methods. Entropy is a term that is poorly understood by physicists and unfamiliar to biologists. Entropy, in a biological context, can be seen as a measure of systemic disorder, with health representing a state of maintained low entropy. The mechanism of maintaining order is the subject of this paper with emphasis on the organ of negative entropy -the lymphatic system.
## I. INTRODUCTION
Entropy is not a term commonly used in the study of biology. To be more in line with fundamental physical principles, the purpose of this paper is to advance biological concepts to include entropy. Life is seen everywhere on our planet, and we have rudimentary descriptions of life. A definition of life proposed by Macklem and Seely; is
"A self-contained, self-regulating, self-organizing, self-reproducing, interconnected, open thermodynamic network of component parts which performs work, existing in a complex regime which combines stability and adaptability in the phase transition between order and chaos, as a plant, animal, fungus, or microbe." (1)
The description between order and chaos is entropy. I personally prefer the mathematical definition by physicist Erwin Schrödinger (1944), "What Is Life? The Physical Aspect of the Living Cell".
"How would we express in terms of the statistical theory the marvelous faculty of a living organism, by which it delays the decay into thermodynamically equilibrium (death)? We said before: 'It feeds upon negative entropy', attracting, as it was a stream of negative entropy upon itself, to compensate for the entropy increase it produces by living and thus to maintain itself on a stationary and fairly low entropy level. If $D$ is a measure of disorder, its reciprocal, $l/D$, can be regarded as a direct measure of order. Since the logarithm of $I / D$ is just minus the logarithm of $D$, we can write Boltzmann's equation thus:
$$
-(entropy) = k \log (I/D)
$$
Hence the awkward expression 'negative entropy' can be replaced by a better one: entropy, taken with the negative sign, is itself a measure of order. Thus, the device by which an organism maintains itself stationery at a fairly high level of orderliness (= fairly low level of entropy) really consists continually sucking orderliness from its environment". (2)
Statistical entropy described by Boltzmann was used to explain gas molecules in a container and the thermodynamic principle of entropy was used by Carnot to explain the efficiency of steam engines. Negative entropy providing order was introduced by Schrödinger. Further development using energy to provide order has not been advanced. Biology illustrates transient reprieve from chaos. Although chaos is the direction of the universe, transient reprieve from chaos can be seen everywhere with stars being born from star destruction.
Health is maintenance of order The mechanism of maintaining order is the subject of this paper with emphasis on the organ of negative entropy - the lymphatic system. Processes providing negative entropies to maintain order are:
1. Utilize environmental energy to combat chaos (process energy sources - food)
2. Remove metabolic debris (take out the garbage)
3. Adaptation to the environment to maintain homeostasis (dry land requires salt and water management, calories sources changes – protein, fat, carbohydrate)
4. Protection from the environment, invaders, predators, identify self-versus non-self (fight to stay alive)
5. Repair broken parts by aiding stem cells to differentiate and reach their targets (repair battle wounds and replace aging cells) - Electromagnetic information management targets and replaces cells.
Disease is failure to perform the 5 processes listed. Chaos wins the battle when these processes fail, and the organism reaches maximum entropy of room temperature. The lymphatic system performs all the 5 processes and should be considered the organ of negative entropy.
## II. PROCESSES OF NEGATIVE ENTROPY WITH AN EVOLUTIONARY VIEW
The five processes can be traced with an evolutionary view. When individual cells became a community of cells, life had to obtain energy, remove metabolic byproducts, maintain homeostasis with the environment, protect the colony from foreign invaders, and assure persistence by devoting energy to reproduction (3 - 5). Insects evolved early before mammals shortly after moving from water to land habitat. These segmented species were the first to incorporate the immune system with a circulatory system. The system is an open system supplying nutrition to cells, removing metabolic debris, providing protection from environmental threats and hemocytes to repair damaged cells (6). The open circulatory system fulfills all the processes required to maintain order.
Segmentation of insects was an advantage decreasing the steps required to evolve into a complex organism (7). New species composed of similar segments had an advantage developing slightly different characteristics of individual segments to benefit the organism. In more complex organisms the evolutionary steps would be nearly impossible. Manipulation of genetic code by point mutation directed by environmental advantage is unlikely to result in a complex immune system within current time constraints. The lymphatic system, the segmented evolutionary ancestor of the insect hemolymph is incorporated into nearly all species suggesting the entire system has been shared and refined.
A proposed chimeric evolution incorporating entire systems would speed evolution explaining why so much of the genic code is shared (8). Insect hemolymph can still provide valuable insight in the study of the human lymphatic system. Humans likely share a chimeric relationship with arthropods. Considering the proposed evolution from insects, the human lymphatic system likely has segmented properties.
## III. RELEVANCE OF LYMPHATICS IN ORGAN SYSTEMS TO MAINTAIN LOW ENTROPY
The human lymphatic system is difficult to visualize limited to swollen limbs. Previously, the existence of lymphatic circulation in organs, blood vessels, and especially the brain was not appreciated. Embryology of the lymphatic system is different from arteries and veins (9). Neglecting the role of lymphatics in specific organ systems was a result of information deficit. Magnetic Resonance Imaging (MRI) viewing free water in interstitial space is an indirect measure of lymphatic function. Understanding the role of the lymphatic system in the context of reducing entropy by the 5 processes allows conjecture of their importance in health of organ systems. Enhancing lymphatic functions to lower the entropy of the individual has potential for extending biological age.
### a) Gastrointestinal System
All energy enters through the oral cavity from the environment including invaders. The unutilized energy substrate is removed by the cecum. Eating, obtaining nutrients and energy, is the most inflammatory daily process determining the microbiome. The intestinal system has a rich lymphatic network to transport these nutrients and serve as a gatekeeper preventing invaders from harming the collection of cells we call human. The gut hormones have influence on the lymphatic system (10). The lymphatic system, besides transporting nutrients, is the immune system, providing protection from environmental invaders (negative entropy). This function of immunity is also responsible for unchecked inflammation causing disease (positive entropy). Hs-CRP (high sensitivity C-Reactive Protein) is a biomarker reflecting systemic inflammation. An unhealthy microbiome activating unchecked inflammation is measured by the biomarker CRP. CRP is evolutionary conserved and is crucial to immune function (11). CRP exists in two forms, a pentameric and a monomeric form explaining how it can function in both disorder (positive entropy) and influence repair (negative entropy) (12). This biomarker has a mortality prediction. CRP depending on its form can have positive or negative influence on the lymphangion both causing and resolution of interstitial edema and inciting and resolution of inflammation.
Hypertension, a risk factor, can be related to homeostasis of environmental salt and water. The endothelium of lymphatics can store excess sodium (13,14). If this system fails intravascular volume increases blood pressure. Lymphatics are in blood vessel walls and contribute to lipid deposition, inflammation, repair. Failure of these arterial wall lymphatics will harden the arterial wall increasing pulse wave velocity, a powerful predictor of mortality and systolic hypertension.
Hormones produced by the gut have significant control of lymphangion function. Sodium-Glucose Transport Protein 2 (SGLT2) Inhibitors, glucagon-like peptide 1 (GLP-1) agonists have impacted patient care in means beyond current explanations with the most likely explanation of Lymphangiontrope an enhancement of removal of interstitial fluid and anti-inflammatory effects.
### b) Kidney
Homeostasis of fluid and electrolytes, stimulating hematopoiesis, removing metabolic byproducts are processes of reducing entropy. The kidney has a network of lymphatics maintaining tissue fluid in an organ responsible for the body's maintenance of this same fluid. Kidney swelling occurs in heart failure when pre-load increases. Kidney swelling also occurs in inflammatory states. If the lymphatics have dysfunction, kidney swelling will decrease its filtration rate with an increase in creatinine. Chronic kidney disease is associated with albuminuria representing Lymphatic dysfunction.
Sodium-Glucose Transport Protein 2 (SGLT2) Inhibitors help decongest the kidney, reduce albuminuria, and remodel the cardiovascular system (15). The gut hormones glucagon-like peptide 1 (GLP-1) agonists have positive effects on the lymphatic system (16). Both reduce the biomarker Hs-CRP and increase the function of circulating progenitor cells.
### c) Lungs
The lungs have a rich network of lymphatics due to the lungs being exposed to the environment full of potential invaders. Inflammatory markers of CRP and Procalcitonin are indicators of infection (17). Smoking introduces antigens that further increase inflammation. The chest X-ray remains the most reliable evidence for failure of lymphatics to remove interstitial edema.
### d) Heart
The heart is central in the closed circulatory system. The lymphatics of cardiac structure are poorly studied. The pathological condition of Tako Tsubo syndrome suggests the segmented disease presentation is consistent with the segmented distribution of lymphatics. The proposed mechanism is a regional reduction in the Lymphangion function with tissue accumulation of fluid. After recovery of lymphangion function the tissue edema is removed restoring cardiac function to normal. Pathophysiology remains elusive (18). The heart has metabolic demands with associated increased entropy. Lymphatics are crucial to combating chaos. The heart produces natriuretic peptides that are the most effective stimulus to lymphangion function. The heart signals peripheral lymphangion to compensate for a failure of the closed circulation by increasing the function of the open circulation.
The ultimate therapy for cardiac dysfunction is injectable Brain Natriuretic Peptide (BNP) with a neprilysin inhibitor. In fact, this therapy would aid any disease process of impaired lymphatic function due to lymphangiontrope of BNP. BNP increases the frequency and amplitude of the lymphangion (19). Injectable BNP with a neprilysin inhibitor is not a current therapy. Angiotensin receptor blocker with a neprilysin inhibitor is an approved therapy but relies on the patients intrinsic BNP. If the intrinsic BNP is not a functional therapy (BNP resistance) the therapy may fail.
### e) Blood Vessels
Endothelium, the lining of blood vessels has the greatest representation of cell type in the human body. Risk factors reduce the number of circulating endothelial progenitor cells. Lymphatics are also composed of endothelial cells and supply a rich network to the blood vessels as noted above in hypertensive subsection. The system helps repair endothelium by transporting progenitor cells and removing senescent cells. Lymphatics also transport lipids and inflammatory cells. Atherosclerotic progression and regression are governed by this system under the influence of environmental diet and inflammation. Health is maintenance of good endothelial function supplied by the organ of negative entropy the Lymphatic system.
### f) Brain
High metabolic activity supported by high blood flow and increased oxygen extraction make the brain a highly entropic organ. The amount of negative entropy used to maintain a memory over many years is high and maintenance of memory is poorly understood. Some of the systems which help maintain low entropy are the blood brain barrier to limit foreign invaders, a rinsing supply of cerebral spinal fluid and a lymphatic system to remove the metabolic products (20). Sleep is necessary to enhance lymphatic function. During sleep the brain shrinks in size, increasing lymphatic flow and cerebral spinal flow. Sleep allows reordering of brain function (21). The lymphatic also helps repair cellular senescence by progenitor transport. The Lymphatics role in brain diseases was discussed in a paper Lymphatics: Future Perspectives Unrealized Potential (22). Those concepts are repeated with an entropic view and further propose novel therapies for brain diseases including schizophrenia, depression, anxiety, and Down's Syndrome. All these conditions have biomarker evidence of increased inflammation and therefore reduced lymphatic function (23-29).
## i. Down's Syndrome
Down's syndrome trisomy 23 is a congenital condition. The chromosomal addition, 47 total, increases the entropy of these patients resulting in shortened life spans. In addition to chromosomal entropy these patients are born with increased inflammation as evidenced by elevated Hs-CRP, increased at birth remaining elevated throughout lifespan and contribute to early mortality. The higher the biomarker of Hs-CRP the greater the intellectual deficits (30). Inflammation increases the entropy of the brain by reduced lymphatic removal of waste products. Down's Syndrome represents lymphatic dysfunction of the brain inhibited by CRP with failure to eliminate byproducts of brain metabolism increasing the entropy of the brain. Schizophrenia, depression, anxiety, also have an elevated biomarker of CRP and again the mechanism of brain dysfunction is proposed as lymphatic dysfunction. If therapy can be administered that reduces inflammation and reduces the biomarker Hs-CRP, lymphatic function will improve with preservation of learning, intelligence, and improvement of well-being. There are ethical concerns treating infants with their inability to give consent. The therapies for infants will need to be low risk therapies to justify their use to prove this hypothesis. Therapies for mental illness in adults can be more easily tested with therapies known to reduce CRP.
## ii. Brain Remodeling versus Neurotransmitter Theory
Until recently, the lymphatic system was not recognized. Over the last 120 years receptors and proteins known as neurotransmitters have been discovered (31). This knowledge ushered in pharmacological therapies for brain diseases. The disconnect in the therapeutic response of the neurotransmitter theory is the time frame needed for recovery, estimated to be 6 to 8 weeks. If it was truly a deficit of neurotransmitters the ailment would only take hours to correct. Improvement over 6 to 8 weeks suggest remodeling of brain structure is required. Serotonin, Dopamine, Histamine increase the amplitude and frequency of the Lymphangion (19,32). The suspected benefit of these neurotransmitter drugs is the negative entropy provided by improvement of lymphatic function and brain remodeling.
### g) Biomarkers of Lymphatic Failure
Failure to maintain order in any of the organ systems will result in increasing entropies with a reduction in lifespan. Table 1 summarizes organ systems dysfunction due to lymphatic failure by risk factors and biomarkers. Albuminuria, Hypertension, elevating creatinine, infiltrates on chest x-ray, rising Brain Natriuretic Hormone BNP, reflect failure to manage interstitial fluid. Hs-CRP, Cystatin C, Procalcitonin reflect aberration in the inflammatory system. Circulating progenitor cells, troponin are markers of repair and destruction respectively. The lymphangion is a source of troponin in addition to the heart (33,34). The source of troponin in serious medical conditions is likely from the lymphangion and not the heart. The lymphatic system functions in taking out the garbage, managing inflammation and repair fulfilling the 5 processes. Elevated troponin representing dysfunction of the organ of negative entropy has dire outcomes.
Table 1: Organ Biomarkers/Risk Factors of Lymphatic Dysfunction
<table><tr><td>Organ</td><td>Biomarker/Risk Factor</td></tr><tr><td>Gastrointestinal</td><td>Hs-CRP
Hypertension</td></tr><tr><td>Kidney</td><td>Albuminuria
Creatinine
Cystatin C</td></tr><tr><td>Lungs</td><td>Chest X-Ray
CRP
Procalcitonin</td></tr><tr><td>Heart</td><td>Natriuretic peptides
Troponin</td></tr><tr><td>Blood Vessels</td><td>Circulating Progenitor cells</td></tr><tr><td>Brain</td><td>Hs-CRP</td></tr></table>
## IV. NEGATIVE ENTROPY - A SHIFT TO BIOLOGICAL REPAIR-THERAPEUTIC OPTIONS PROPOSED
A shift in biological therapeutics toward modification of inflammation is actively under development after a very slow beginning. An additional shift to repair mechanisms in biology is still only a glimmer of hope. Both therapeutics are necessary to prolong disease free aging. Repairing organs and the entire organism is necessary to maintain a low entropic state. It is estimated the cell turnover rate is 330 billion cells per day (35). Failure of repair will increase entropy and shorten lifespan. Currently, therapies to enhance repair are nonexistent. Negative entropy requires both repair of senile and damaged cells and controlling inflammation; responsible for removing those cells and paradoxically killing cells under other circumstances. Again, the lymphatic system's role in both processes emphasize the statement lymphatics are the organ of negative entropy.
Positive lymphangiontrope is an invented term defined as an increase in the amplitude and frequency of the lymphangion secondary to an intervention. The intervention may be pharmacological, mechanical or electromagnetic. Pharmacologic study in animals has been in mesenteric vessels and is summarized by Russel (32). There is also some confusion in these interventions since there seems to be occasional opposite responses of the lymphangion and the conductance ducts. The lymphangion is a work horse operating at the tissue level. The ducts tone will affect diastolic flow and is sensitive to the preload of the closed circulatory system. Examination of therapeutic options will be limited to increasing lymphangion function and ignoring the effect on conductance vessels. Lymphangiontrope should also be measured by the efficiency of directing progenitor cells and management of inflammatory responses.
Positive lymphangiontrope, negative entropy, can be inferred from studies in rat mesenteric vessels with visual measures of lymphangion amplitude and frequency and transport of cells. Older rats have a reduction in lymphangiontrope (36), suggesting the increasing entropy of aging is due to decreasing lymphangiontrope. Activation of T cells, B Cells, cytokines, and antibody management are an additional function of the lymphatic system. The sum of these processes is very complex. The results of these processes can be integrated into mortality outcomes. Clinical trials with a reduction in mortality represent the process of negative entropy implying a favorable impact by lymphatics role in inflammation and repair.
All the moving parts of the lymphatic system are difficult to study but can be seen as lifespan. In disease states clinical trials demonstrate a mortality benefit increasing lifespan. Studies with interventions in healthy adults for the purpose of extending life are few. Risk factors in a healthy population predicting future disease states reducing lifespan have been studied. Biologic age is reduced by risk factors, poor lifestyle, adverse biomarkers of inflammation and repair (37). Figure 1 used with permission shows the odds ratios ranked in order of importance of relative all-cause mortality. The lower the ratio, the shorter the lifespan, the greater the positive entropy of the biomarker. The odds ratios from their sources had appropriate confidence intervals and were statistically significant. A reduction in biological age reflects increasing entropy. Medications and interventions moderating risk factors have mortality benefit suggesting the intervention had negative entropy.
Fig. 1: Contributions to Biologic Age with permission Houck P. The Era of Risk Factors Should End; the Era of Biologic Age Should Begin. Hearts. 2025; 6(1):2. https://doi.org/10.3390/hearts6010002 The lower the odds ratio the greater the impact of entropy due to biomarkers and comorbidities
Contributors to Increased Biologic Age
Years of Life Lost to Modifiable Risk
Order of Importance
<table><tr><td>Bio Marker/Risk Factor</td><td>Odds Ratio
All-Cause Mortality</td></tr><tr><td>Pulse Wave Velocity</td><td>.16</td></tr><tr><td>Glucose Intolerance</td><td>.3</td></tr><tr><td>Six-Minute Walk distance</td><td>>414 to <290
1.0 to.37</td></tr><tr><td>Smoking</td><td>.47</td></tr><tr><td>Hypertension</td><td>.57</td></tr><tr><td>Circulating Stem Cells</td><td>.61</td></tr><tr><td>Waist Circumference</td><td>.60-men
.64-women</td></tr><tr><td>ECG Findings</td><td></td></tr><tr><td>RAE</td><td>.67</td></tr><tr><td>LAE</td><td>.63</td></tr><tr><td>LVH</td><td>.53</td></tr><tr><td>Hs-CRP ≥2.0</td><td>.7</td></tr><tr><td>Frailty</td><td>.84-men
.88-women</td></tr><tr><td>Number of Co-Morbidities</td><td>.89-men
1.0-women</td></tr><tr><td>Coronary Artery Calcium >400</td><td>.9</td></tr><tr><td>Short Sleep <7</td><td>.9</td></tr><tr><td>Cholesterol</td><td>.9</td></tr></table>
## V. MODEL OF HEALTH AND DISEASE
Inflammation and repair are represented by Hs-CRP and circulating progenitor cells. The biomarkers of elevated Hs-CRP and reduced circulating progenitor cells have an odd ratio of.7 and.61 respectively from Figure 1. Both biomarkers are also dependent on risk factors. Both biomarkers reflect inflammation and repair and are a predictor of reduction in lifespan. The other biomarkers of a reduced lifespan are seen in Figure 1. can also be related to inflammation and failure to repair or remodel. Smoking, hypertension, metabolic syndrome of diabetes, and waist circumference is linked to stress on the lymphatic system.
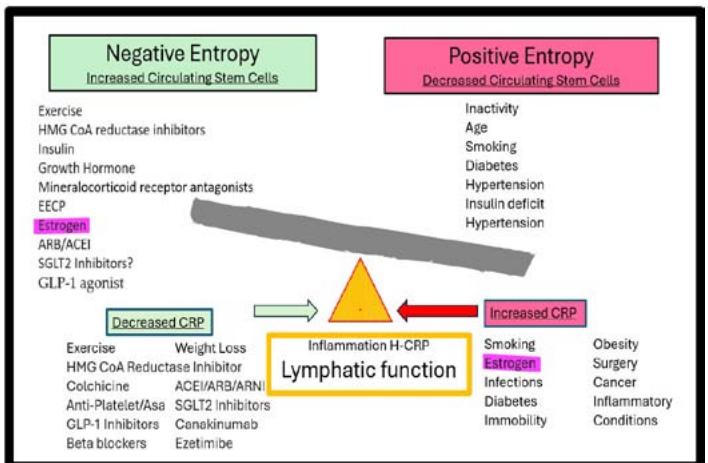
A model of health and disease was previously presented (38). This model considers health when regeneration and degeneration are balanced by the moving fulcrum controlled by inflammation. The model demonstrates the importance of the immune system in both proliferative diseases such as cancer and degenerative diseases such as age and mental illness. Diabetes I is a degenerative disease due to insulin deficit, whereas Diabetes II is aproliferative disease due to insulin excess. The fulcrum is controlled by lymphatic function. Lymphatics also participates in circulating progenitor cells. Figure 2 is a further refined model emphasizing positive and negative entropy with interventions that modify progenitor cells and inflammation in both positive and negative manners. Medication intervention reducing all-cause mortality by modifying Hs-CRP and circulating progenitor cells is seen in Table 2. The odds ratios from the reference have appropriate confidence intervals and were statistically significant. Some of the interventions are listed under both circulating stem cells and a reduction in Hs-CRP and are noted by italics.
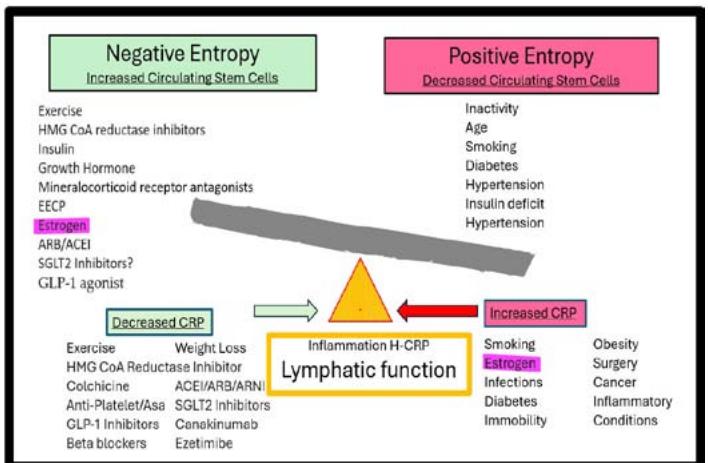
Fig. 2: Model of Health and Disease Balancing Positive and Negative Entropy by Lymphatic Function
Table 2: Odds Ratio of All-Cause Mortality of Medications Modifying Inflammation (Hs-CRP) and Repair (Circulating Progenitor Cells)
<table><tr><td>Inflammation/Repair Biomarkers</td><td>Modifying Medications Interventions</td><td>Absolute Mortality Odds Ratio</td><td>Reference</td></tr><tr><td rowspan="8">Circulating Progenitor Cells</td><td>Exercise</td><td>.68</td><td>(39)</td></tr><tr><td>HMG CoA reductase inhibitors</td><td>.86</td><td>(40)</td></tr><tr><td>Mineralocorticoid receptor antagonists</td><td>.82</td><td>(41)</td></tr><tr><td>Estrogen under 60 over 60</td><td>.61</td><td>(42)</td></tr><tr><td>ARB/ACEI</td><td>1.03</td><td>(42)</td></tr><tr><td>SGLT2 Inhibitors?</td><td>.98</td><td>(43)</td></tr><tr><td>GLP-1 Agonist</td><td>.75</td><td>(44)</td></tr><tr><td>Exercise</td><td>.88</td><td>(45)</td></tr><tr><td rowspan="11">Hs-CRP
Continued below</td><td>Weight Loss</td><td>.68</td><td>(39)</td></tr><tr><td>Statin</td><td>.85</td><td>(46)</td></tr><tr><td>Colchicine</td><td>.86</td><td>(40)</td></tr><tr><td>ACEI/ARB</td><td>1</td><td>(47)</td></tr><tr><td>ARNI</td><td>.98</td><td>(43)</td></tr><tr><td>SGLT2 Inhibitors</td><td>.66</td><td>(48)</td></tr><tr><td>GLP-1 Agonist</td><td>.75</td><td>(44)</td></tr><tr><td>Mineralocorticoid receptor antagonists</td><td>.88</td><td>(45)</td></tr><tr><td>Canakinumab</td><td>.82</td><td>(41)</td></tr><tr><td>Ezetimibe post MI</td><td>.66</td><td>(49)</td></tr><tr><td>Ezetimibe post MI</td><td>.77</td><td>(50)</td></tr></table>
## VI. DISCUSSION
Messages from Figure 1, 2, and Table 2 reveal lack of exercise will decrease circulating stem cells and increase the inflammatory state. As the distance of six-minute walk decreases, frailty increases, obesity and metabolic syndrome become further manifestations increasing Hs-CRP. The lack of exercise as measured by the six-minute walk is a powerful predictor of short-term survival. From Table 2. The odds ratio of total absolute mortality for exercise is.68, the best of all the interventions. Exercise is clearly needed for enhancing lifespan and improving lymphatic function. Diseases of the brain a failure of lymphatic function should be treated with exercise as a primary modality.
HMG
CoA
Reductase
Inhibitors,
Mineralocorticoid receptor antagonists, SGLT2 Inhibitors, GLP-1 Agonist, also are listed as agents that reduce Hs-CRP and increase circulating stem cells with improvement of lifespan. These agents are favorable to the lymphatic system and should be considered in brain diseases and other diseases of reduced repair and inflammation regardless of a medical condition warranting their use. This statement is bold reflecting a change of direction in medical therapeutics from observation, trial and error to utilization of predictive models to repair a malfunction. The use of these medications is to treat the organ of negative entropy - the lymphatic system to maintain good health.
Estrogen, highlighted by red outline in figure 2 is confusing, having properties of both positive and negative entropy increasing progenitor cells and increasing Hs-CRP making it vascular friendly and prothrombotic proinflammatory. Clinical trials failed to elucidate a female advantage due to the use of fixed dose estrogen. For the purposes of reproduction, immunity is shifted during changes in cyclic estrogen. The shift is necessary to immunosuppress the mother to accept the father's antigens. T helper cell 1 (Th1) is shifted to T helper cell 2 (Th2) altering the Th1/Th2 balance (51). This shift favors vascular repair explaining the paradox. Previous clinical trials in estrogen failed to elucidate the female advantage due to fixed dose estrogen. It is time to reinvestigate the female advantage using variable dose estrogen in the perimenopausal period measuring Hs-CRP and circulating progenitor cells in addition to clinical measures.
### a) Negative Entropy
Entropy is the second law of thermodynamics – if the system is irreversible the entropy of the system and the environment increases. Statistical entropy described by Boltzmann is a refinement but is limited due to the complexity of systems. The mathematical description represents disorder in all possible states. It can be used to predict gas laws. Debate over the concept of negative entropy raged during the time of Schrödinger and continues. Negative entropy represents the energy of a system to maintain or become more orderly. Two cells becoming one requires energy (negative entropy) and can be calculated. After performing a step in a biological system, the next step may have multiple possible outcomes. If the next pathway is critical there will be carrier protein or energy source directing to a successful outcome representing negative entropy (52, 53). The entropy of a human considers all the parts and how the parts can be arranged. The number of parts is the primary driver of entropy. The virome and microbiome, far out way the number of cells in the human body. These tiny inhabitants of the human body by numbers can cause chaos. The evidence is in pandemics. The study of the virome and microbiome should have priority due to their ability to increase entropy. Systems to reduce entropy are necessary to maintain order and extend lifespan.
Entropy can be a positive force seen in favorable mutations selecting environmental winners - evolution or can be devastating causing disease and fatal consequences. Entropy can misfold proteins, produce aberrant proteins with disease caused by resistance. Drug discovery can be more efficient considering statistical entropy. Improving the organ of negative entropy can extend lifespan.
### b) Desired Outcomes Generated by Entropy and the Lymphatic System
- B.1: Appreciate lifespan is determined by negative entropy provided by the lymphatic system.
- B.2: The brain is a highly entropic organ maintaining order with the lymphatic system.
- B.3: Brain diseases should be treated by enhancing lymphatic function, especially exercise.
- B.4: Down's Syndrome has a biomarker of therapy Hs-CRP. Interventions during infancy and perhaps prenatal reducing Hs-CRP should be explored – consider BNP.
- B.5: Drug development should routinely study lymphangiontrope in rat mesenteric vessels, measure drug affect by Hs-CRP and their effect on circulating progenitor cells.
- B.6: Women's health advantage should study variable dose estrogen.
- B.7: A simple model of health and disease described as progenitor cells balanced by the lymphatic system can describe complex biology and offer solutions that are obscured by complexity. A simple program can result in complex behavior (54).
- B.8: Injectable BNP with a neprilysin inhibitor should be studied for lymphatic dysfunction, heart failure, and especially brain diseases including Down's syndrome.
- B.9: The relationship of the virome and microbiome to Hs-CRP and circulating progenitor cells should be studied.
## VII. CONCLUSION
Entropy, a fundamental concept in physics and chemistry, is not utilized in the study of biology. Biology must obey the rules of entropy and for a period can maintain order. The method of maintaining order can be modeled by circulating progenitor cells and inflammation controlled by Hs-CRP. The lymphatic system supplies thisorder. Pleiotropic properties of medications can be ascribed to lymphatic function of negative entropy. Interventions providing negative entropies with longer lifespans, include exercise, HMG CoA Reductase Inhibitors, Mineralocorticoid receptor antagonists, SGLT2 Inhibitors, GLP-1 Agonist. In the future, search for therapeutic options should include measurement of lymphangiontrope, Hs-CRP, and circulating progenitor cells.
Future Directions
This paper presents simple rules and a simple model to explain health and disease. These concepts can be accelerated by proving the model. After appropriate validation of the model, it can be used in many scenarios to treat diseases that have no current recommendations. An initial plan of study would be to include measurement of progenitor cells, Hs-CRP inflammatory changes, and animal models to detect changes of lymphangiontrope by intervention. Understanding the model will lead to repair therapies which will decrease entropy and extend lifespan.
Funding: No funding
Author contributions:
Conceptualization: PDH
Writing - original draft: PDH
Writing - review & editing: PDH
Data and materials availability: All data are available in the main text
Generating HTML Viewer...
References
54 Cites in Article
Peter Macklem,Andrew Seely (2010). Towards a Definition of Life.
Eleanor Hollywood,Marie Hyland,Muluken Basa (1943). Identifying integrated family support approaches for families living in the International Protection Accommodation Services (IPAS) system in Ireland.
Richard Michod (2007). Evolution of individuality during the transition from unicellular to multicellular life.
James Valentine (1978). The Evolution of Multicellular Plants and Animals.
Yan Yan,Julián Hillyer (2020). The immune and circulatory systems are functionally integrated across insect evolution.
C Reiber,I Mcgaw (2009). A review of the "open" and "closed" circulatory systems: new terminology for complex invertebrate circulatory systems in light of current findings.
A Chipman,G Edgecombe (1912). Developing an integrated understanding of the evolution of arthropod segmentation using fossils and evo-devo.
R Rogers,D Hartl (2012). Chimeric genes as a source of rapid evolution in Drosophila melanogaster.
P Som,M Francois (2017). The Current Concepts of the Embryology of the Lymphatic System.
M Zhuang,X Zhang,J Cai (2024). Microbiota-gut-brain axis: interplay between microbiota, barrier function and lymphatic system.
James Mcfadyen,Johannes Zeller,Lawrence Potempa,Geoffrey Pietersz,Steffen Eisenhardt,Karlheinz Peter (2020). C-Reactive Protein and Its Structural Isoforms: An Evolutionary Conserved Marker and Central Player in Inflammatory Diseases and Beyond.
Ibraheem Rajab,Peter Hart,Lawrence Potempa (2020). How C-Reactive Protein Structural Isoforms With Distinctive Bioactivities Affect Disease Progression.
Hoon Choi,Hyeong Park,Sung Ha (2015). Salt Sensitivity and Hypertension: A Paradigm Shift from Kidney Malfunction to Vascular Endothelial Dysfunction.
T Stougiannou,K Christodoulou,T Koufakis,F Mitropoulos,D Mikroulis,C Mazer,D Karangelis (2024). The impact of neurovascular, blood-brain barrier, and glymphatic dysfunction in neurodegenerative and metabolic diseases.
Jennaya Christensen,Glenn Yamakawa,Sandy Shultz,Richelle Mychasiuk (2019). Is the glymphatic system the missing link between sleep impairments and neurological disorders? Examining the implications and uncertainties.
P Póvoa,L Coelho,J Cidade,A Ceccato,A Morris,J Salluh,V Nobre,S Nseir,I Martin-Loeches,T Lisboa,P Ramirez (2024). Biomarkers in pulmonary infections: a clinical approach.
P Houck,H Dandapantula,E Hardegree,J Massey (2020). Why We Fail at Heart Failure: Lymphatic Insufficiency Is Disregarded.
M Braun,J Iliff (2020). The impact of neurovascular, blood-brain barrier, and glymphatic dysfunction in neurodegenerative and metabolic diseases.
Jennaya Christensen,Glenn Yamakawa,Sandy Shultz,Richelle Mychasiuk (2020). Is the glymphatic system the missing link between sleep impairments and neurological disorders? Examining the implications and uncertainties.
Philip Houck,Hari Dandapantula,Janet Massey (2023). Lymphatics: Future Perspectives Unrealized Potential.
Nathan Lewis,Jamie Knight (2021). Longitudinal associations between C-reactive protein and cognitive performance in normative cognitive ageing and dementia.
Laura Orsolini,Fabiola Sarchione,Federica Vellante,Michele Fornaro,Ilaria Matarazzo,Giovanni Martinotti,Alessandro Valchera,Marco Di Nicola,Alessandro Carano,Massimo Di Giannantonio,Giampaolo Perna,Luigi Olivieri,Domenico De Berardis (2018). Protein-C Reactive as Biomarker Predictor of Schizophrenia Phases of Illness? A Systematic Review.
T Liukkonen,P Räsänen,J Jokelainen,M Leinonen,M-R Järvelin,V Meyer-Rochow,M Timonen (2011). The association between anxiety and C-reactive protein (CRP) levels: Results from the Northern Finland 1966 Birth Cohort Study.
M Cepeda,Paul Stang,Rupa Makadia (2016). Depression Is Associated With High Levels of C-Reactive Protein and Low Levels of Fractional Exhaled Nitric Oxide.
A Macdonald,D Adamis,A Treloar,F Martin (2006). C-reactive protein levels predict the incidence of delirium and recovery from it.
R Chancel,J Lopez-Castroman,E Baca-Garcia,R Mateos Alvarez,P Courtet,I Conejero (2024). Biomarkers of Bipolar Disorder in Late Life: An Evidence-Based Systematic Review.
Ye Tu,Yan Fang,Guohui Li,Fei Xiong,Feng Gao (2024). Glymphatic System Dysfunction Underlying Schizophrenia Is Associated With Cognitive Impairment.
S Manti,M Cutrupi,C Cuppari,E Ferro,V Dipasquale,G Di Rosa,R Chimenz,M La Rosa,A Valenti,V Salpietro (2018). Inflammatory biomarkers and intellectual disability in patients with Down syndrome.
Francisco López-Muñoz,Cecilio Alamo (2009). Historical evolution of the neurotransmission concept.
Peter Russell,Jiwon Hong,Natalie Trevaskis,John Windsor,Niels Martin,Anthony Phillips (2022). Lymphatic contractile function: a comprehensive review of drug effects and potential clinical application.
Mariappan Muthuchamy,Anatoliy Gashev,Niven Boswell,Nancy Dawson,David Zawieja (2003). Molecular and functional analyses of the contractile apparatus in lymphatic muscle.
Joshua Scallan,Scott Zawieja,Jorge Castorena‐gonzalez,Michael Davis (2016). Lymphatic pumping: mechanics, mechanisms and malfunction.
Ron Sender,Ron Milo (2021). The distribution of cellular turnover in the human body.
Anatoliy Gashev,David Zawieja (2010). Hydrodynamic regulation of lymphatic transport and the impact of aging.
Philip Houck (2025). The Era of Risk Factors Should End; the Era of Biologic Age Should Begin.
Philip Houck,Jose De Oliveira (2013). Applying laws of biology to diabetes with emphasis on metabolic syndrome.
William Kraus,Kenneth Powell,William Haskell,Kathleen Janz,Wayne Campbell,John Jakicic,Richard Troiano,Kyle Sprow,Andrea Torres,Katrina Piercy (2018). Physical Activity, All-Cause and Cardiovascular Mortality, and Cardiovascular Disease.
Roger Chou,T Dana,I Blazina,M Daeges,T Jeanne (2016). Error in USPSTF Report on Statin Use.
Chang Geng,Yu-Cheng Mao,Su-Fen Qi,Kai Song,Hong-Fei Wang,Zi-Yan Zhang,Qing-Bao Tian (2023). Mineralocorticoid receptor antagonists for chronic heart failure: a meta-analysis focusing on the number needed to treat.
Shelley Salpeter,Judith Walsh,Elizabeth Greyber,Thomas Ormiston,Edwin Salpeter (2004). Mortality associated with hormone replacement therapy in younger and older women.
Edmond Li,Balraj Heran,James Wright (2014). Angiotensin converting enzyme (ACE) inhibitors versus angiotensin receptor blockers for primary hypertension.
Henrik Svanström,George Mkoma,Anders Hviid,Björn Pasternak (2024). SGLT-2 inhibitors and mortality among patients with heart failure with reduced ejection fraction: linked database study.
Søren Kristensen,Rasmus Rørth,Pardeep Jhund,Kieran Docherty,Naveed Sattar,David Preiss,Lars Køber,Mark Petrie,John Mcmurray (2019). Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials.
S Kritchevsky,K Beavers,M Miller,M Shea,D Houston,D Kitzman,B Nicklas (2015). Intentional weight loss and all-cause mortality: a meta-analysis of randomized clinical trials.
Ibadete Bytyçi,Gani Bajraktari,Peter Penson,Michael Henein,Maciej Banach (2022). Efficacy and safety of colchicine in patients with coronary artery disease: A systematic review and meta‐analysis of randomized controlled trials.
George Sokos,Amresh Raina (2020). <p>Understanding the early mortality benefit observed in the PARADIGM-HF trial: considerations for the management of heart failure with sacubitril/valsartan</p>.
P Ridker,P Libby,J Macfadyen,T Thuren,C Ballantyne,F Fonseca,W Koenig,H Shimokawa,B Everett,R Glynn (2018). Modulation of the interleukin-6 signalling pathway and incidence rates of atherosclerotic events and all-cause mortality: analyses from the Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (CANTOS).
V Kytö,A Tornio (2024). Ezetimibe use and mortality after myocardial infarction: A nationwide cohort study.
P Kidd (2003). Th1/Th2 Balance.
P Houck (2014). Should negative entropy be included in the fundamental laws of biology?.
Philip Houck (2020). Making Drug Discovery More Efficient Applying Statistical Entropy to Biology.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Philip Houck. 2026. \u201cEntropy and the Lymphatic System, a New Model with Therapeutic Potential\u201d. Global Journal of Medical Research - B: Pharma, Drug Discovery, Toxicology & Medicine GJMR-B Volume 25 (GJMR Volume 25 Issue B1): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
A descriptor of life is a phase transition between order and chaos. Entropy is the physical property of this transition determining lifespan. Rules of maintaining entropy and a model of health and disease are presented simplifying scientific methods. Entropy is a term that is poorly understood by physicists and unfamiliar to biologists. Entropy, in a biological context, can be seen as a measure of systemic disorder, with health representing a state of maintained low entropy. The mechanism of maintaining order is the subject of this paper with emphasis on the organ of negative entropy -the lymphatic system.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.