## I. INTRODUCTION
Vascular anomalies are divided into two groups: tumors and vascular malformations. They constitute a polymorphic set of pathologies whose etiologies are not well elucidated. The classification of these VMTs, formerly grouped under the name angiomas remains unclear [1]. The work of Mulliken and Glowacki made it possible to distinguish vascular tumors (involving cellular proliferation) from malformations (structural abnormalities of the vessels due to a disruption of vascular morphogenesis during embryonic development). The management of VMTs requires a multidisciplinary approach involving several specialists (pediatrician, dermatologist, radiologist, vascular-surgeon, plastic surgeon, psychologist) [2].
Our objective was to report our observations on patients with tumors or vascular malformations undergoing surgery in the Thoracic and Cardiovascular Surgery Department of the Fann National University Hospital, in Dakar, Senegal.
## II. PATIENTS AND METHODS
This was a descriptive and retrospective analytical study of all cases of tumors and vascular malformations operated on between 2004 and 2022. The parameters studied were age, sex, history, clinical presentation, imaging data (ultrasound, CT angiography), surgical protocol, morbidity, and mortality. The mean follow-up time was 3 years.
## III. RESULTS
The total number of patients was 52 over the 18 years. The sex ratio was 0.5. Themean age was 24 years, with a range of 2 to 72 years. Consanguinity was found in $8\%$. Klippel-Trenauney syndrome was found in $2\%$. Trauma or recent surgery was noted in 9 patients $(17\%)$. The mean time to consultation was 8 years, ranging from 3 months to 20 years. The reason for consultation was a mass in $94\%$ of cases, pain $(37\%)$, a skinmark $(2\%)$, a sensation of trembling $(4\%)$, or a skin ulceration $(8\%)$. The physical examination revealed a mass in 47 patients. It was associated with vascular characters in 13 cases, skin ulceration in 4 cases, collateral venous circulation in 2 cases, and limbdeformity in 2 cases. The location of the lesions (Figure 1) predominated in the neck (Figure 2) and the head $(54\%)$. No multiple locations were noted. Vascular Doppler ultrasound was performed in 28 patients and found an arteriovenous malformation $(n = 11)$, an angioma $(n = 4)$, a venous malformation $(n = 2)$, a lymphangioma $(n = 2)$, a glomus tumor $(n = 2)$, a hemangioma $(n = 2)$ or a vascular mass of undetermined nature $(n = 4)$. The ultrasound data were sufficient to make the diagnosis in 12 patients $(23\%)$. CT angiography was performed in 40 patients, 24 of which $(46\%)$ were performed immediately without prior ultrasound. It revealed an arteriovenous malformation $(n = 22)$, a venous malformation $(n = 5)$, an angioma $(n = 4)$, a lymphangioma $(n = 4)$, a hemangioma $(n = 2)$, a glomus tumor $(n = 2)$ orangiosarcoma $(n = 1)$ (Figure 3). The therapeutic procedure consisted of excision $(n = 39)$, ligation of the feeding artery $(n = 15)$ or primary embolization $(n = 3)$. An additional procedure was performed in 6 patients. This consisted of elastic compression, sclerotherapy, additional ligation of the feeding artery, or embolization. The postoperative course was satisfactory in $88\%$ of cases (Figure 4). Elsewhere, they were marked by hemorrhage with hematoma formation $(4\%)$ requiring revision, suppuration of the surgical site $(6\%)$ controlled by antibiotic therapy, and severe limbischemia $(2\%)$ for which forearm amputation was performed. Recurrence was noted in $8\%$. The average time to recurrence was 2 years and varied from 1 to 5 years. No deaths were observed.
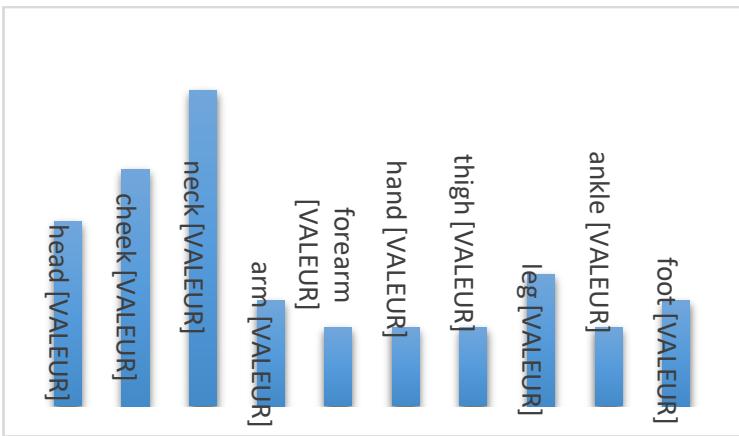
 Figure 1: Topography of Lesions
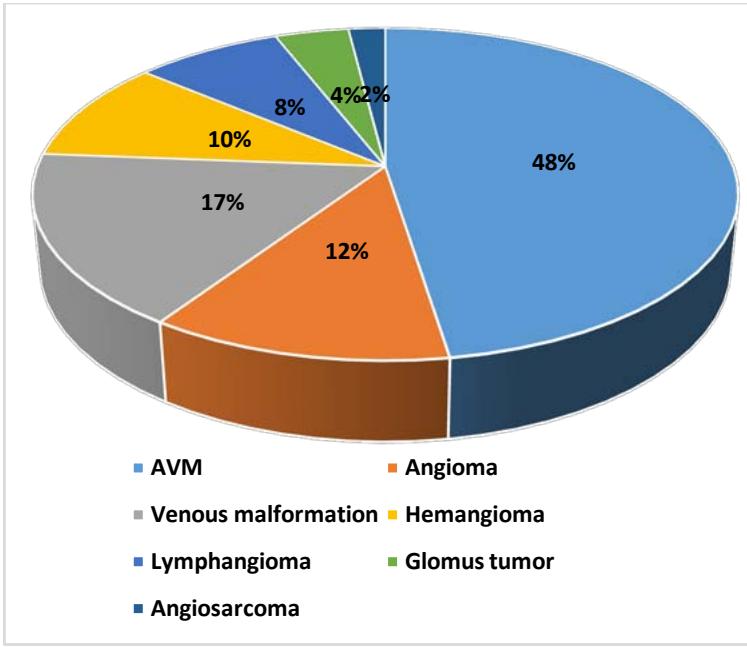 Figure 3: Ultrasound Data Combined with CT Angiography
 Figure 2: Cervical AVM with Large Draining Vein
 Figure 4: Before and After Surgical Excision of a Labial AVM
## IV. DISCUSSION
Until 1970, the term angioma referred to all vascular anomalies. It was not until 1996 that the classification established by Mulliken and Glowacki in 1982 was validated by the ISSVA (International Society for the Study of Vascular Anomalies), thus making it possible to separate malformations from vascular tumors [2]. Depending on the vessel involved, there is an arterial, venous, or lymphatic anomaly. A vascular tumor is a proliferation of endothelial cells, while a vascular malformation results from an anomaly in the embryogenesis of the vessels, leading to wall alterations [3]. One in three children is born with a vascular spot, red, blue, or purple, which for the most part will disappear. One in a hundred children will retain this vascular anomaly, which will warrant medical advice [4]. The average age of our patients was 24 years. This result is different from those found in other literature where the average age varied between 3 and 5 years [5,6] for vascular tumors and 15 years for vascular malformations [7]. This age difference is explained by the fact that in our country, patients tend to consult late. But also, for most surgical series like ours, the age of the surgical indication is retained and the latter is pushed back as much as possible. The female predominance reported in the literature is found in our
patients [7,8,9]. This female predominance could be explained by the fact that mothers of female infants consult more because of the aesthetic impact of the condition [10]. For both tumors and vascular malformations, we found a hereditary character. Couriveau in a retrospective study reports that vascular malformations are transmitted in an autosomal dominant manner [11]. Vascular anomalies can be latent for a long time, and their development can be triggered by factors such as trauma, surgery, or puberty, which was observed in $17\%$ of our patients.
The main reason for consultation for vascular anomalies is the observation of a mass, posing a cosmetic problem or a source of social embarrassment. Sometimes, it is an ulceration, often linked to a delay in consultation. This was the case in $94\%$ of our patients. Vascular tumors and malformations are ubiquitous. Cervicocephalic locations are the most common as found in our study $(53\%)$ and those of several Western or African authors such as Belzunce $(50\%)$, Diarra $(50\%)$, and Casanova $(75\%)$ [7,8,12].
The size of vascular anomalies varies, ranging from a few millimeters to several centimeters. However, according to Casanova, hemangiomas smaller than 3 cm are the most frequent and extensive forms are the rarest [12]. Certain vascular anomalies such as arteriovenous malformations (AVMs) can be revealed by rarer complications. Heartfailure in a healthy heart revealing an AVM has been described by Sow [13].
Diagnosing certain vascular tumors such as hemangiomas is essentially clinical, the contribution of medical imaging remains essential in other cases. Ultrasound is the first-lineimaging modality. It is noninvasive, reproducible and inexpensive. It allows diagnosis in themajority of cases, but it remains operator-dependent. Twelve patients $(23\%)$ were operated on based on Doppler ultrasound. CT angiography is indicated in cases where ultrasound does not allow a decision. It provides additional information, particularly for AVMs, by outlining the feeding and drainage vessels, as well as the topography of the nidus. Johnson recommends starting with an MRI for the diagnosis of vascular malformations in general and arteriovenous malformations in particular [14]. He argued that MRI would allow treatment planning by characterizing the flow rates and the number of vessels involved in the malformation. In addition, it is a technique that visualizes soft tissues well and reduces radiation, especially in young subjects requiring followup. The criticism he reported for Doppler ultrasound was that it could not accurately study deep lesions near bone structures or lesions containing air. Inour series, all patients benefited from either Doppler ultrasound, CT angiography, or both, in cases where Doppler ultrasound was not helpful. MRI was not performed in anycase because it is an expensive examination, sometimes unavailable, and the twoprevious examinations were sufficient for a positive diagnosis.
The therapeutic arsenal is broad with specific indications for each form. Therapeutic abstinence with surveillance is adopted in cases of hemangiomas by many teams [15,16]. This attitude is explained by their potential for spontaneous regression. Ceballo describes a spontaneous regression of $30\%$ of hemangiomas in 3 years, $50\%$ in 5 years and $70\%$ in 7 years [17]. Alazard in a study on 44 lymphatic malformations found a spontaneous regression in $15\%$ of cases [18]. Medical treatment with Bisoprolol is proposed as a first-line treatment for complex infantile hemangiomas. Other drugs such as corticosteroids, antimitotics (vincristine) can be used. Surgery in VMT is most often indicated after failure of well-conducted medical treatment or in case of major functional or vital risk for the patient [19]. In our series, primary excision was the main procedure for all anomalies combined, followed by primary ligation of the feeding artery for AVMs. Primary embolization was performed in 3 patients.
Complications can occur postoperatively. Diop describes hemorrhagic accidents and peripheral facial paralysis during MAV treatment of the face[19]. Mortality is zero in our series as in most surgical series [20,21].
## V. CONCLUSION
MVDs are diverse and varied, sometimes little understood. They exhibit clinical, anatomical, and progressive polymorphism. They are mostly benign, with a few rarecases of malignancy described. While in the majority of cases, diagnosis is primarily clinical, medical imaging remains essential in cases of doubt. The prognosis of certain complex anomalies can be poor. Classifications are thus established to facilitate the choice of the most appropriate treatment for each type of VMD.
Management by a multidisciplinary team consisting of a dermatologist, radiologist, vascular surgeon and plastic surgeon help reassure parents and ensure optimal treatment.
Generating HTML Viewer...
References
18 Cites in Article
M Wassef,R Vanwijck,P Clapuyt,L Boon,G Magalon (2006). Tumeurs et malformations vasculaires, classification anatomopathologique et imagerie.
K Zwicker,J Powell,C Cummings (2022). Vascular anomalies in childhood: when to treat patients and when to refer them to a specialized resource.
S Guero (2007). Vascular tumours and malformations of the limbs.
R Vanwijck,G Magalon (2006). Les anomalies vasculaires. Introduction.
N Dégardin-Capon,V Martinot-Duquennoy,P Patenotre,G-M Brevière,F Piette,P Pellerin (2006). Le traitement chirurgical précoce des hémangiomes cutanés.
C Kayak,N Yaris,M Kutluk (2001). Management of cutaneous hemangiomas: a retrospective analysis of 1109 casesand comparison of conventional dose prednisolone with high-dose methylprednisolone therapy.
A Belzunce,M Casellas (2004). Complications in the evolution of hemangiomas and vascular malformations.
I Cigden,J Marcus (1999). Sturge-Weber syndrome: report of an unusual cutaneous distribution.
D Casanova,F Norat,J Bardot,G Magalon (2006). Les hémangiomes cutanés : aspects cliniques.
N Sow,M Leye,I Bass (2018). Heart failure in a normal heart revealing a complex arteriovenous malformation of the lower limb in a child: a case report and review of the literature.
J Johnson,P Cogswell,M Mcknsick,L Binkovitz,S Riederer,P Young (2014). Pretreatment imaging of peripheral vascular malformations.
A Bruckner,I Frieden (2006). Infantile haemangioma.
G Lorette,M Piram,D Herbreteau,P Lermusiaux (2004). Le syndrome de Sturge-Weber-Krabbe.
C Ceballos,J Ramundo (2005). Management of infants with ulcerated hemangiomas.
B Salazard,J Londner,D Casanova,J Bardot,G Magalon (2006). Les malformations lymphatiques : aspects cliniques et évolution.
M Diop,Dieng,Gaye Sow,N,Ciss Ba,P (2018). Arteriovenous Malformations: Clinical Aspects and Surgical Results.
Byung-Boong Lee,Y Do,Wayne Yakes,D Kim,Raul Mattassi,W Hyon (2004). Management of arteriovenous malformations: a multidisciplinary approach.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Ndeye Fatou Sow. 2026. \u201cEpidemiological, Clinical, and Therapeutic Aspects of Tumors and Vascular Malformations in Senegal: About 52 Cases\u201d. Global Journal of Medical Research - F: Diseases GJMR-F Volume 25 (GJMR Volume 25 Issue F1).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































