## I. INTRODUCTION
### a) Background
Blood pressure refers to the pressure inside the arteries. Hypertension means that the blood is exerting more pressure than in normal. Over time, this weakens and damages blood vessel walls. Hypertension may also cause thickening of the artery walls, resulting in narrowing and eventual blockage of the vessel. In atherosclerosis, the pressure of pumping blood could 'hose off' debris from damaged artery walls. $^{1}$
Smoking has been shown to raise blood pressure by vasoconstriction and accelerated heart rate as acute effect. Different groups have reported that no association existed between smoking habit and blood pressure. One group found that blood pressure of smokers was lower than that of non-smokers or that smoking raises blood pressure.
However, in one study, smokers were found to have stage 1 hypertension as against of non smoker, 38 percent of smokers and 44 percent of non-smoker were pre-hypertensive (subjects with systolic blood pressure $120 - 139\mathrm{mm / Hg}$ and diastolic blood pressure $80 - 89\mathrm{mm / Hg}$ )[6]. The nicotine in cigarettes and the lack of oxygen to the body's tissues causes blood vessels to thin. Smoking makes the body unable to circulate blood properly, which in turn causes high blood pressure. The carbon monoxide from smoking cigarettes causes cholesterol deposits to form on the arterial walls. Blood clots become more likely because of the nicotine.[7]
Nicotine raises blood pressure by constricting blood vessels. This occurs because the oxygen in blood decreases and because nicotine directly stimulates the production of a hormone, epinephrine (also known as adrenaline), in the adrenal gland. Epinephrine raises blood pressure by constricting blood vessels.[8]
Worldwide, approximately 1 billion people addicted to cigarette. In developed countries $35\%$ of men and $22\%$ of women smoke, while in developing countries $50\%$ of men $9\%$ of women are smokers. $^{10}$ In 2003, the smoking prevalence in our country, among adult was $54.8\%$ in males and $16.6\%$ in females. The prevalence of smoking in age group 18-29,30-39,40-49 is respectively 36.3, 64.2, $70.8\%$. $^{11}$
Every year a man smokes a pack a day, he shortens his life by almost 2 months. Even 1 stick of cigarette can reduce life span of a man about 11 minutes.[12] Data from large prospective studies of population in several countries have shown that cigarette smoking men have 70 percent higher overall death rates than non-smokers. The effect of mortality is proportionately greatest in younger age group.[13]
Smokeless tobacco use is a significant part of the overall world tobacco problem. Unlike cigarettes and other forms of tobacco, smokeless tobacco is consumed without combustion (without burning). Instead, it is placed in contact with mucous membranes in the mouth or nose, through which nicotine is absorbed into the body. The use of nasal snuff is returning. Different forms of snuff, such as loose or packed snuff, are used by placing in the mouth. Tobacco may also be prepared in blocks and flakes for chewing. In North America, smokeless tobacco use typically consists of the oral use of snuff (moist or dry). In Central, South and Southeast Asia, smokeless tobacco is usually chewed with another substance, such as ash, lime, cotton, sesame or betel quid (a mixture of nut, lime, and leaves).[14-16] Smokeless tobacco is a harmful tobacco product that contains over 3,000 chemicals, 7 including 28 known carcinogens (cancer-causing agents).[17] Smokeless tobacco affects the cardiovascular system and is associated with heart disease, stroke and high blood pressure.[18-27]
Like cigarettes, smokeless tobacco contains nicotine, and nicotine affects the heart. It is not surprising, then, that studies have found that smokeless tobacco increases heart rate and blood pressure,[19,23-27] and puts users at increased risk for stroke, coronary heart disease, peripheral vascular disease (that is, diseases of the arteries and veins) and cardiovascular death.[18,20,22] However, it should be noted that some studies have shown no relation between smokeless tobacco use and stroke or cardiovascular mortality.[28,29] Further rigorous studies are needed to determine more clearly the cardiovascular risks potentially associated with smokeless tobacco use.[30,31]
During last decade the garment sector gave Bangladesh and her workers an image boost, both in South Asia and the rest of the world. Currently, Bangladesh exports 35 types of garment products to about 31 countries around the world. It is seen that RMG export earning is very significant and continue to increase. Bangladesh maintained its position as the sixth largest exporter of apparel to the United States during 1994-97. It was the largest exporter of T shirts and shirts to the European Union in 1992 and 1993.[78]
Results of several studies have shown that for a long time, garment workers' health has been viewed within a narrow prospective. However, this has been largely overlooked both by researchers and policymakers. Health and productivity is highly correlated. The better the health of a worker the higher is productivity. Thus, good health is of much importance to them. But in most cases policymakers and researchers are not aware of how workers health is affected by their work. This awareness is important.
### b) Justification of the Study
Smoking is harmful for health is well known. Smoking causes death is printed over the cigarette packet as caution note. In Bangladesh, anti-smoking law was launched by government in June 2005. In spite of the anti-smoking law, smoking is a common problem in Bangladesh and also a major health problem associated with morbidity and mortality. Active smoker are not only harming their health but also making a fatal threat towards the innocent people by exposing them to passive cigarette smoking.[46]
Smokeless tobacco, also called spit tobacco, chewing tobacco, chew, chaw, dip, plug, and probably a few other things, comes in two forms: snuff and chewing tobacco. Regardless of the differences between smokeless tobacco products, they all contain nicotine, a highly addictive chemical, and cause equivalent nicotine levels in the blood as smoking cigarettes. Smokeless tobacco products are as addictive as cigarettes and can cause the same type of dependence, which makes quitting smokeless tobacco very difficult. Furthermore, nicotine may factor into coronary artery disease, peripheral vascular disease, hypertension, peptic ulcer disease, and foetal effects.[50]
A considerable number of garment factories have been established in our country, providing opportunity for employment from different corners of the country mainly from lower socio-economic groups. Workers of the garments factory have their own routine style of living, belief, channel of command and supervision. A research in respect of health status of the workers in this new discipline will provide us knowledge about health of the specific group of workers.[77]
So the present study was to find out the prevalence of hypertension on tobacco users. The findings, discussions and recommendations of this study will form a basis for dissemination of knowledge on the subject and area of ignorance will stimulate further research for socio-economic development through production of healthy workers. It will help to collect and disseminate data (Health information) to Govt., NGO's, Public Health Institute, Research Organization, etc. It will give information to develop health care policy and guideline, define priority intervention area of health. And also recognize health care service and plan public health strategies.
Several studies in other countries have shown the hazardous effect of smoking and smokeless tobacco as change of blood pressure. But there is not any study found in Bangladesh on this issue. So the present study will be done to see the prevalence of hypertension among tobacco users.
### c) Operational Definitions of Terms
- Age: Calculated in year, up to one character after decimal (1 year means 1.0 to 1.9 year) from date of birth mentioned by the patients.
- Educational Status:
Illiterate: It includes all the men who could not read or write and only could read or write and only could sign their name.
Primary: It includes all the men who had read up to or completed the class from one to five.
Secondary: It includes all the men who had read up to or completed the class from six to S.S.C.
Higher education: It includes all the men who at least completed their bachelor degree.
- Tobacco: Any product of tobacco leaf of any origin, may be in the form of Cigarettes, Pipes. Hukka.
- Smokeless tobacco: Tobacco preparations without producing smoke. smokeless tobacco chewing, tobacco leaf with betel quid ('Pan').
- Frequency of smoking: For cigarettes and bidi (biri) the frequency of tobacco smoking is noted from number of sticks smoked per day. In case of hukka the frequency is noted from how many times one smokes per day.
- Smokeless Tobacco Users: In the present study, smokeless tobacco users are that subjects who have used any form of smokeless tobacco product for last 5 years or more.
- Smoker: In this study, smokers are those subjects, who smoke cigarette, ten or more per day, regularly for last five years or more.
- Blood Pressure Parameters: In this study, BP parameters are mainly systolic (110—140 mm Hg) and diastolic (60—90 mm Hg) blood pressure.
- Hypertension: High blood pressure is said to be present if it is persistently at or above $140 / 90 \mathrm{mmHg}$.
- Hypotension: Hypotension is generally considered to be systolic blood pressure less than $90 \mathrm{~mmHg}$ or diastolic less than $60 \mathrm{~mmHg}$.
### d) Research Question
What is the epidemiological profile of hypertension on smokers and smokeless tobacco users among the male garment workers in Dhaka city of Bangladesh?
## II. REVIEW OF RELATED LITERATURE
The readymade garment (RMG) is a key sector of Bangladesh economy. The garment industry of Bangladesh has been expanding rapidly since late 1970. During 1977-78 only about one lakh taka was earned by exporting garment, while the figure raised to taka one core by 1980. In 1989-90 the industry earned 624.16 million dollars. The export earning was 3781.94 million dollars during 1997-98 i.e. about 73.28 percent of the total export earnings. Jute was once the main export earner for Bangladesh, accounting for 75 percent of the total earnings in 1978; garments have however increasingly replaced this. Garment is now the largest export earner in Bangladesh. But only 25-30 percent of garment export is value-added, since the fabrics and accessories are imported under a back to back arrangement.[79] As a formal export-oriented industry, the manufacturing of garments emerged as a tiny scale in Dhaka city in 19766-77. By 1983, only 47 garment manufacturing units were established. The number of garment industries doubled in the mid-1980s with an influx of foreign investments. By 1987, the garment industry was the leading export sector. New garment factories were set up in Dhaka, and in other cities like Chittagong and Khulna. The total number of garment industries rose to 2500 units in 1996, employing some one million workers. The Bangladesh garment industry has now flourished as one of the major exporters of ready-made garments in the world market.[80]
In 1996, Bangladesh exported garments worth US\(2.5 billion to the US and other export markets. The US has almost half of the export market for garments and the rest are made up of Germany, France, Italy, UK, Netherlands, Canada and so on.[80]
The garments of Bangladesh are increasingly becoming visible in the markets of developed countries. For example, Bangladesh was the $9^{\text{th}}$ supplier in 1998 to the US market having a market share of 3 percent. For the cotton garments, Bangladesh was the $4^{\text{th}}$ supplier having a market share of 5 percent. Beside the US,
Bangladesh also supplies ready-made garments to the European Community (EC) market and Canada.[81]
Garment industry not only accounts for the lion share of export earnings of the country, but also accounts of the employment. In terms of employment the garment industry was the fourth largest employing sector in 1998. According to BGMEA about 1,500,000 workers were employed in about 2800 garment industries.[81]
Zahir and Majumder on their study regarding the incidence of illness found that 54 percent of the workers had fairly good health before undertaking employment in the garment factory. But this figure came down only 12 percent after they joined the garment factory. Work day's loss due to an illness a yardstick to measure the extent of adverse health impact of wage employment on garment workers. About 46 percent of workers had to take leave for some unavoidable reasons of which illness is one of dominant case.[82]
Hypertension may be primary, which may develop as a result of environmental or genetic causes, or secondary, which has multiple aetiologies, including renal, vascular, and endocrine causes. Primary or essential hypertension accounts for $90 - 95\%$ of adult cases, and a small percentage of patients $(2 - 10\%)$ have a secondary cause.[88]
Hypertension develops secondary to environmental factors, as well as multiple genes, whose inheritance appears to be complex.[83-84] Furthermore, obesity, diabetes, and heart disease also have genetic components and contribute to hypertension. Epidemiological studies using twin data and data from Framingham Heart Study families reveal that blood pressure has a substantial heritable component, ranging from $33 - 57\%$.[85,86,87]
Smoking is a process of dry distillation during which the nicotine is partially destroyed at the burning tip of the cigarette or cigar. Part of the nicotine is vaporized, some of the vapour being condensed in the cooler proximal part of the cigarette. The smoke inhaled through a cigarette, for instance, is called the main stream, and that rising from the burning tip between puffs is called the side stream.[32] The literary meaning of 'Ciker' is 'smoking'. Cigero has been derived from 'Ciker' and this cigero is modified into cigarette in France. The word cigarette was derived from Spanish word "cigar" — a rolled tobacco leaf. Cigarette is the most popular and commonest form of tobacco consumption throughout the world.[33]
Tobacco smoking is the act of smoking tobacco products especially cigarettes and cigars.[34] Passive smoking is inhalation of environmental second hand tobacco smoke. Involuntary or second hand smoke occurs when the exhaled and ambient smoke from a person's cigarettes is inhaled by other people.[35] Nonsmoker means a person who never smoked cigarette as any kind of tobacco products.[36] Smoking cessation is who stopped smoking. It is possible to reduce the risk by reducing the frequency of smoking.[34]
The word 'tobacco' has originated from the word 'tube' or a cylindrical pipe, made out of a rectangular piece of a leaf used for packing tobacco for the purpose of inhaling its smoke conveniently. Tobacco, a rapidly growing leafs plant was originally cultivated in the primitive colonies of America from time immemorial. Tobacco was not known to the old world till the first quarter of the 16th century. The entry of the tobacco plant into the old world is linked with the expedition of Columbus to America. When he landed in America in 1642, he was offered dried tobacco leave. The use of tobacco leaf to create and satisfy nicotine addiction was introduced to Columbus by Native Americans and spread rapidly to Europe.[37] In 1612 the British colony at Jamestown, Virginia, began growing wild tobacco and exporting it to England. They soon switched to common tobacco in West Indies and Europe. The Arawak people smoked tobacco through a tube they called a Tobago, from which the name tobacco originated. In about 1864 an Ohio farmer happened upon a chlorophyll deficient strain of tobacco called white burley, which become a main ingredient at American blended tobaccos.[38]
Currently, there are an estimated 1.3 billion smokers in the world. The death toll from tobacco consumption is now 4.9 million people a year; if present consumption patterns continue, the number of deaths will increase to 10 million by the year 2020, $70\%$ of which will occur in developing countries.[39]
There are various forms of smoking such as tobacco, cannabis, hashish and cocaine. Main sources of tobacco use in Bangladesh are cigarette, biri, hukka, chew tobacco, pan-masala etc. Among these cigarette is the second highest prevalence. Biris are especially popular by the rural and lower income groups.[40]
Bangladesh is one of the high tobacco consuming countries. Tobacco is mainly smoked in the form of Cigarette, Biri, cigar, pipe, hukka in our country. In addition to high smoking rate, Bangladesh people use smokeless tobacco, such as zarda, sada pata, panmasala, and gui.[39]
About 130 million people in Bangladesh are tobacco smokers which cost them 13.43 billion taka per year. A study in Jaydebpur revealed that $71\%$ male & $20\%$ female do smoke regularly. Out of them $42\%$ was suffering from various diseases, $41\%$ among them are respiratory related illness.[41]
Tobacco is one of the main agricultural products of Bangladesh and ranks fourth after jute, sugarcane and tea.[42] According to WHO report on Bangladesh, agriculture in 1993,[44] 192 hectares were harvested for tobacco. $0.5\%$ of all arable land is used for tobacco growing. In 1992, Bangladesh produced about 75,000 million manufactured cigarettes and biris (about $1.3\%$ of world total). Industries in 1993, about 131,000 people were employed full time in tobacco leaf processing and tobacco manufacturing, wholesaling and retailing occupations. About 2, 04,500 people are engaged full time in farming tobacco.[43]
In 2003, the smoking prevalence in Bangladesh, among adults was $54.8\%$ in males and $16.6\%$ in females. The prevalence of smoking in age group 18-29, 30-39, 40-49 is respectively 36.3, 64.2, and $70.8\%$.
Unburned tobacco contains nicotine. When it is burned the resultant smoke contains, in addition to nicotine, carbon monoxide and 4000 other compounds that results from volatilization. The smoke is composed of a fine aerosol, with particle size distribution predominantly in the range to deposit in the airways and alveolar surface of the lungs. Which contains a large number of toxic constituents and carcinogen compounds.[45]
Smoking harms nearly every organ of the body; causing many diseases and reducing the health of smokers in general. The adverse health effects from cigarette smoking account for an estimated 438,000 deaths, or nearly 1 of every 5 deaths, each year in the United States. More deaths are caused each year by tobacco use than by all deaths from human immunodeficiency virus, illegal drug use, alcohol use, motor vehicle injuries, suicides, and murders combined.[46,47]
Smoking has several health effects such as coronary heart disease, abdominal aortic aneurysm, bronchitis, lung cancer, cancer of pharynx, cancer of oral cavity.[89, 90] Also smoking has many adverse reproductive and early childhood effects, including increased risk for—Infertility, Preterm delivery, Stillbirth, Low birth weight, Sudden infant death syndrome (SIDS).[91]
Smokeless tobacco has been around for a long time. Native people of North and South America chewed tobacco, and snorting and chewing snuff was popular in Europe and Scandinavia (the word "snuff" comes from the Scandinavian word "snus").[48]
A comparison is often made between the smokeless tobacco products in Sweden and those in the U.S. However, smokeless tobacco products sold in Sweden are manufactured according to Sweden's laws governing food and must meet additional industry established quality indicators (known as the Gothiatek System [50]) involving ingredients and measurements for harmful elements such as tobacco specific nitrosamines (TSNAs) and other toxins and carcinogens. Products that have been subjected to this process have been found to be lower in TSNA levels (e.g., some Swedish brands have been found to possess only 2 percent of the TSNA levels of their U.S. counterparts) and maintain these low levels over time. In contrast, products sold in the U.S. have no uniform manufacturing code, are not regulated, and contain significantly higher levels of carcinogenic substances, including TSNAs, which, unlike their Swedish counterparts, have been found to increase over time.[52] As a result, U.S. smokeless tobacco products have been found to pose serious health risks and are a known cause of cancer.[53] On the other end of the spectrum, in India, Pakistan, Bangladesh, Sri Lanka, Myanmar, Thailand, the Lao People's Republic, Cambodia, the Philippines, and Palau, smokeless tobacco products such as betel quid with tobacco, areca nut with tobacco, or gutka had significantly higher rates of oral, pharyngeal, and oesophageal cancers. People who chewed betel quid with tobacco also showed higher prevalence of leukoplakia.[54]
Studies are inconclusive as to how significantly smokeless tobacco affects users' cardiovascular systems, but it has been studied that it may have more nicotine than cigarettes. One study states that, "Although the evidence is not conclusive, the adverse cardiovascular effects of smokeless tobacco use are less than those caused by smoking but are more than those found in non-users."[55] Other studies also indicate that smokeless tobacco related cardiovascular risks are lower than that of smoked tobacco.[56, 57] One study states that smokeless tobacco use has a "positive effect on cardiovascular risk factors in young physically fit men."[58] However, it is important to note that one Indian study from the state of Rajasthan states, "There is a significantly greater prevalence of multiple cardiovascular risk factors [sic] obesity, resting tachycardia, hypertension, high total and LDL cholesterol, and low HDL cholesterol, and electrocardiographic changes in tobacco users, chewing or smoking, as compared-to tobacco non-users. Chewing tobacco is associated with similar cardiovascular risk as smoking."[59] This finding may bear on the possibility that smokeless tobacco in India is produced differently than in Western countries. Due to contrasting results in studies, many conclude that further research should be done on the cardiovascular risks of smokeless tobacco.[60, 61]
Smokeless tobacco contains nicotine, which is the primary reinforcing agent. According to European Union policy, Scandinavian or some American smokeless tobaccos are at least $90\%$ less hazardous than cigarette smoking.[62] However, the habit is still addictive.
Taxation and restriction of smoking is causing more smokeless tobacco use as "substitution." There are active public health debates regarding risk-reduction for smokers and the reconsideration of smokeless tobacco risks. "There is a substantial body of informed and independent opinion that sees the value of harm reduction strategies based on smokeless tobacco."[63] Most of these studies are supported by the makers of smokeless tobacco.
Smokeless tobacco is addictive and harmful. Some tobacco control strategists nonetheless believe that encouraging a shift toward smokeless tobacco use can be an effective harm reduction approach on the basis that these products may reduce total tobacco-caused death and disease despite exposing users to potentially harmful constituents.[66] WHO's Scientific Advisory Committee on Tobacco Products Regulation raises a cautionary note in this regard. In the committee's assessment, current evidence does not indicate that use of any smokeless tobacco is free of health risks. They conclude that there is no evidence to support any claims that suggest smokeless tobacco is free of health risks.[67] The relationship between smokeless tobacco use and smoking is difficult to ascertain. Though some studies find that smokeless tobacco use is more likely to precede smoking,[68, 69] it is more commonly found that smoking precedes smokeless tobacco use.[70]
Although some people may use snuff to quit smoking, a study showed that U.S. men more commonly switch from snuff use to smoking. There is evidence that snuff may serve as a supplemental source of nicotine for some male current smokers. Nearly half of men who used snuff on some days were current smokers, and those who currently smoked only on some days were more likely than never smokers to be current snuff users. Male smokers who used snuff every day smoked, on average, fewer cigarettes per day, again suggesting that snuff may serve as a supplementary source of nicotine. Also, smokers who also use snuff are more likely than non-users of snuff to try to quit smoking but tend to be less successful.[68] Given these uncertainties, other strategists take the view that, regardless of the specific levels of harm caused by smokeless tobacco products, their overall inherent risks do not support smokeless tobacco as a viable harm reduction strategy. The major concern about promoting one tobacco product as less harmful than another is that it may undermine efforts to achieve total tobacco-product cessation or may foster smoking initiation among people who otherwise would not have started.[68]
Dentists and dental hygienists are trained to detect oral lesions and periodontal problems that are related to tobacco use. It is thus appropriate for them to help prevent the initiation of tobacco use by children and adolescents through the use of positive anti-tobacco messages. Over the past decade, tobacco cessation strategies have been modified for practical use in dental settings. A study reviewed several brief interventions by dental professionals to encourage the cessation of smokeless tobacco use: oral cancer screening, cessation advice, self-help materials, and brief cessation counselling by a dental hygienist. This study found that oral screening and brief cessation counselling by dental professionals in the dental office or in athletic facilities were effective in promoting cessation of smokeless tobacco use. Furthermore, a 2006 review showed that behavioural interventions conducted by oral health professionals improved rates of cessation of smokeless tobacco use. Incorporating oral assessments and behavioural interventions in dental practices may encourage cessation of smokeless tobacco use.[71]
In a 2004 review of several studies examining cessation of smokeless tobacco use, there was no indication of benefits of using pharmacotherapy including bupropion, a nicotine patch, or nicotine gum. However, it was suggested that larger trials investigating pharmacotherapy are needed. Research in the area of smokeless tobacco cessation is limited but seems to suggest that a combination of therapies offers the greatest hope for success.[72]
Considering that smokeless tobacco products still contain varying levels and types of carcinogens $^{73}$
and cause other types of health risks compared to cigarettes, the only way to reduce an individual tobacco users health risks to the maximum extent possible is to quit using tobacco entirely with evidence-based treatments that have been scientifically documented to help people quit using tobacco (e.g., nicotine gum and patch, telephone-based behavioural counselling/ quit lines).[74] Smokeless tobacco use during youth can lead to a lifetime of addiction to smokeless tobacco or, frequently, to cigarettes, as the nicotine addiction created by smokeless use ultimately leads to habitual smoking.[75] Evidence shows that adolescent boys who use smokeless tobacco products have a higher risk of becoming cigarette smokers within four years.[76]
### a) Conceptual framework
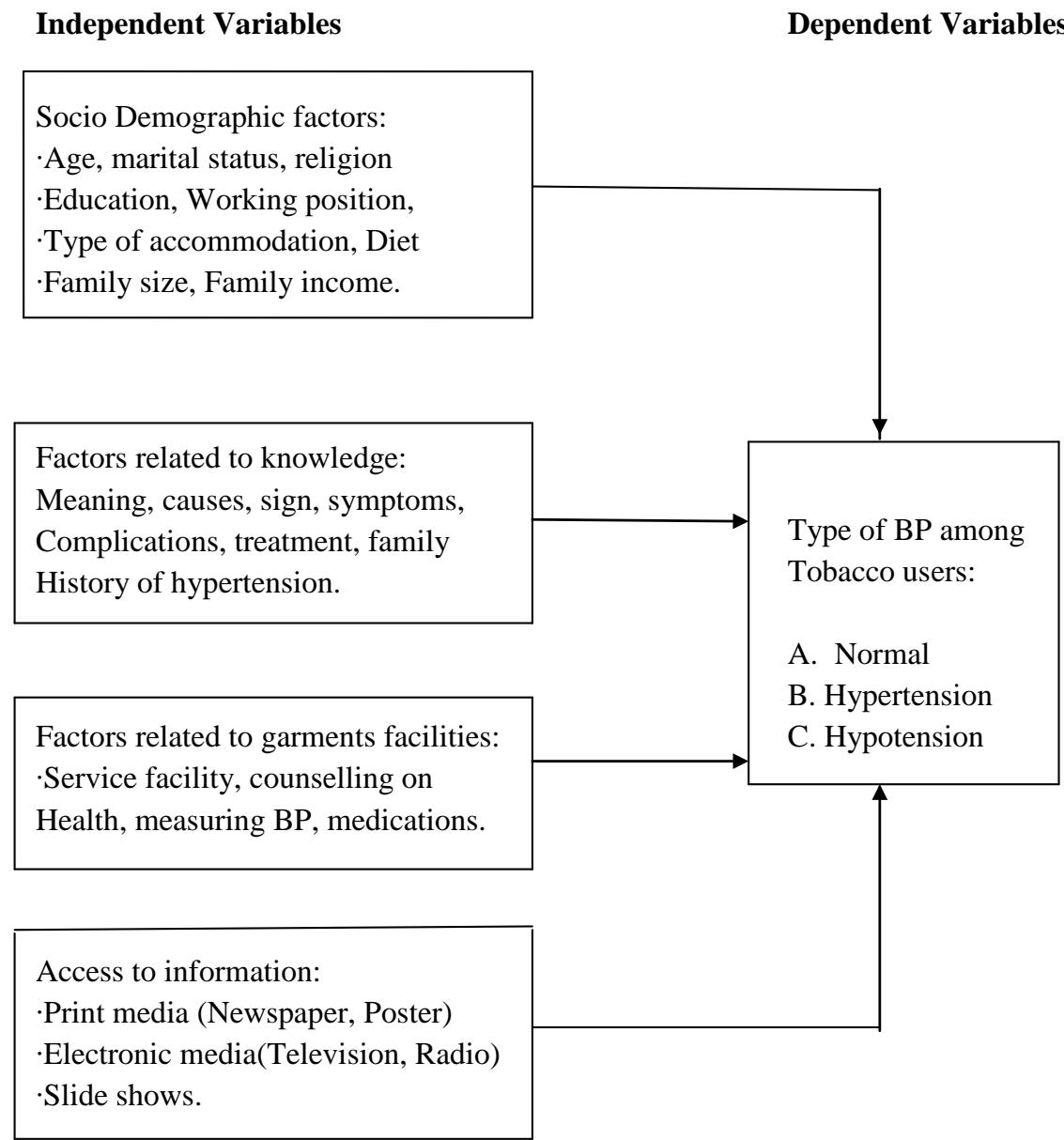
#### General Objective
To explore epidemiological profile of hypertension on the smokers and smokeless tobacco users of male garment workers in Dhaka city of Bangladesh.
#### Specific Objectives
1. To describe the socio demographic factors among the smokers and smokeless tobacco users of male garment workers in Dhaka city of Bangladesh.
2. To assess the level of knowledge on hypertension of male garment workers.
3. To assess the educational needs to improve their awareness of hypertension on male garment workers.
4. To explore the parameters of hypertension among the male garment workers.
5. To assess the access to information on male garment workers.
#### Study Design
It was done descriptive type of cross-sectional study among the male garment workers.
#### Study Area
The study was carried out in Level I clinic, Civil Engineers' Tower, Standard Group, Kalshi, Mirpur-11, Dhaka.
The reason for selecting this place was:
Easy communication
Assurance of all positive help and co-operation by the authority.
A good number of study subjects were available at a time.
### Study period
The study was done within the time period of September to October 2013.
#### Study Population
The respondents of the study were the smoker and smokeless tobacco users.
#### Eligible Criteria
### a) Inclusion Criteria
Participants who meet the criteria were included in the study:
1. Adult male smokers.
2. Adult male smokeless tobacco users.
3. Smokers smoking ten or more cigarettes per day for more than 5 years.
4. Smokeless tobacco users using any form of smokeless tobacco for more
a. than 5 Years
5. Age: Over 18 years
6. Sex: Male
### b) Exclusion Criteria
Participants that were excluded from the study:
1. Person who could not give history properly.
2. Unwilling to take part in study after the verbal consent process.
3. Those that was not co-operative.
Sample Size Determination:
The sample size was determined by following formula
$$
n = \frac {z ^ {2} p q}{d ^ {2}}
$$
Where, n = the desired sample size which would help to measure the different indicators
z = the standard normal deviate, usually set at 1.96 at $5\%$ level which corresponds to $95\%$ confidence level.
The assumed target proportion is $p$ to have a particular characteristics and $q = 1 - p$, Here $p = 0.5$
Putting the values in the above equation the sample size $n$ is estimates as
$$
3. 8 4 \times 0. 5 \times 0. 5
$$
$$
0. 0 5 ^ {2}
$$
$$
n=384 (targeted sample size)
$$
#### Sample Size
The present study has been designed to measure blood pressure among adult male smoker and smokeless tobacco users. For the academic purpose and time limitation 105 patients of over 18 years were selected from outdoor medicine units of level-I clinic from Standard Group's garment, Dhaka.
### Sampling Technique
Purposive sampling (all smoker and smokeless tobacco user attended at outdoor medicine units of Level-I clinic of Standard Groups Kalshi factory.).
The patients were grouped as follows:
Group A: Consisted of 30 adult smokeless tobacco users.
Group B: Consisted of 75 adult -smokers.
#### Data Collection Tool
- Semi-structured Questionnaire and check list.
- Semi-structured questionnaire was used as a tool for collection of data.
#### Data Collection Technique
The self-report technique was adopted as the data collection technique. The research ethical committee of Public Health Department, North South
University giving ethical clearance of the study that followed by permission of Managing Director and Chief Medical Officer of Standard Group. The data collection should be carried out from $15^{\text{th}}$ September to $15^{\text{th}}$ October, 2013. Total 105 individuals participated in the research and none of them withdrew their consent from the study.
Questionnaire was translated into Bengali language for data collection by face to face interview. Blood pressure measurement was carried out by researcher himself with the help of check list.
#### Data Processing
After collection data should be cleared, coded and categorized. Then the Master Tabulation Sheet should prepare after proper checking, verifying and editing as per specific objective and key variables.
#### Data Analysis
Statistical analyses of the results should be obtained by using window based computer software devised with Statistical Packages for Social Sciences (SPSS-15). During analysis frequency distribution of variables should worked out and produced in tabular form. Results of statistical analysis between the groups would be calculated by using unpaire 't' test.
#### Ethical Consideration
- Ethical clearance
- Permission of Managing Director and Chief Medical Officer of Standard Group.
- Consent of the individual patients
- Privacy and confidentiality
- Data only used for this research.
#### Limitations of the Study
Despite all efforts there should be some limitations of the study. Community based study unusually bear some limitations. The limitations are as follows:
a) Only men are included. So the estimated values of variables in this study of male smokers and smokeless tobacco users cannot be generalized to females.
b) The sample size is small. So the result obtained from the study may not be generalized.
c) The study place is an outdoor of level-I clinic. So the result may be different from the indoor department. The validity of the result is applicable in this particular situation.
d) The study should be based only on interview records; no scope of observational checks is there. So there may not be sound reflection.
#### Expected Outcomes
This study will estimate status of hypertension in smoker and smokeless tobacco user and will reveal the influencing of blood pressure among the garment workers. Thus it may help to reduce the effect of hypertension on smoker and smokeless tobacco user in future and they will lead a healthy life.
Generating HTML Viewer...
Funding
No external funding was declared for this work.
Conflict of Interest
The authors declare no conflict of interest.
Ethical Approval
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Britto. 2026. \u201cEpidemiological Profile of Hypertension on Smokers and Smokeless Tobacco Users Among the Male Garment Workers in Dhaka City of Bangladesh\u201d. Global Journal of Medical Research - K: Interdisciplinary GJMR-K Volume 24 (GJMR Volume 24 Issue K3): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.