Structured Abstract- Background: Infertility affects about 10 - $15\%$ of reproductive-age couples. The diagnosis and treatment of this disorder stands out as one of the most rapidly evolving area in the medicine. The majority of pelvic pathology in infertile women is frequently not well appreciated by routine pelvic examinations and the usual diagnostic procedures. The ability in visualizing the uterine cavity, fallopian tubes, ovaries and identifying the possible pathology during laparoscopy and hysteroscopy has made it an essential part of infertility evaluation and therapeutic procedures can also be done in the same sitting.
### Synopsis:
Investigation of female infertility is incomplete without a Hystero-laparoscopy, as all the exact aetiology which may be of the ovarian, tubal, uterine, peritoneal, endometriotic, cervical, causes can be known, and in addition, treatment for these causes can also be offered in the same sitting.
## I. INTRODUCTION
Infertility has always been one of the elusive symptom complex that perplexes the best gynecologists. The couple is said to be infertile if they fail to conceive after one year of unprotected and regular sexual intercourse. $^{1-2}$
It is also known as subfertility.60-80 million couples are subfertile all over the world. It is said to be primary if she fails to conceive at all and secondary if she fails to conceive after a child birth or undoubted miscarriage. It affects $10 - 15\%$ of couples in the reproductive age group. Its overall prevalence has been stable during past 50yrs however a shift in etiology and patient age has occurred[1-4].
Due to increased awareness and eagerness to have a pregnancy, couples are seeking medical help early. Focus of infertility treatment has shifted from systematic correction of each identified factor to apply most efficient therapy[6].
Of the causes of infertility, female factors contribute $40 - 50\%$, male by $30 - 40\%$, both partners- $10\%$ and unexplained $-10\%$ in the remainder. Among this female factors have pathology in either uterine, cervical, tubal, ovarian, peritoneal, endometrial tissue etc. The ability to see and manipulate the uterus, tubes, and ovaries during laparoscopy made it an essential part of infertility evaluation[2-6].
The main advantage of laparoscopy over laparotomy is, it decreases postoperative pain, shorter hospital stay and decreases mortality.
Laparoscopy is one of the most significant advances in the investigation of the infertile couple in the last six years.
It is an indispensable tool which can be considered as a definitive day care procedure for evaluation and treatment of infertility.
But hystero-laparoscopy has become the "third eye of gynaecologists in the diagnosis of infertility. Though both represent invasive procedures laparoscopy aid for studying the peritoneal, endometrial, peritubal and ovarian morphology whereas hysteroscopy gives exact picture of intrauterine pathology[7-8].
Chromopertubation at the laparoscopy also gives idea of tubal patency and also avoids false negatives obtained by HSG because of tubal spasm. While it is probably true to say that no infertility investigation is complete without endoscopic evaluation. With the introduction of this hysteroscopy and laparoscopy there is tremendous uplift as the mere diagnosis of the causes of infertility and offering management also at the same setting $^{7-8}$.
The current evidence indicates a $9\%$ prevalence of infertility, $56\%$ of couples seeking medical care. Therefore approximate prevalence of female infertility is $5 - 6\%$, as female infertility accounts for $40 - 50\%$ (of which ovulatory dysfunction $40\%$, tubal and pelvic pathology $40\%$, uterine and cervical factors $10\%$, unexplained $10\%$.
WHO estimates the overall prevalence of primary infertility is between 3.9 and $16.8\%$, affects 8-12% of couples worldwide, and $3 - 5\%$ unknown conditions.[12]
Hence present study planned to evaluate role of hystero-laparoscopy in primary and secondary infertility to identify the causes in female genital tract leading to infertility and to develop plan of therapy.
## II. METHODOLOGY
Study Design: An observational study to evaluate the infertility cases with hystero-laparoscopy in women with primary and secondary infertility in tertiary care centre.
Study Period: JUNE 2018-MAY 2019
Sample Size:
$$
N = z^{2} P Q / L^{2}
$$
$$
N = \text {sample size} Z = 1.96 \text {at} 95 \% \text {CI}
$$
P (prevalence) = 3.9% (The WHO estimates the overall prevalence of infertility in India to be between 3.9 and 16.8 per cent. To yield more sample size, lower prevalence is considered for sample size calculation)[12]
$$
Q = 100 - 3.9 = 96.1 \%
$$
$$
\mathrm{L} = 5\% \text{(Precision)}
$$
$$
N = 3. 9 4 \times 3. 9 \times 9 6. 1 / 5 \times 5
$$
N=57.56 Making it to near value sample size considered is 60.
### Data Collection Technique and Tools:-
Study is conducted in all patients in our hospital who attended infertility clinic for the treatment of infertility. All patients were evaluated clinically by diagnostic tests and are given treatment accordingly. By considering exclusion and inclusion criteria sample size was taken as 60.
Written and informed consent were taken after explaining the nature and purpose of the study. Patients who were willing to participate and met the inclusion criteria were included. Data collection was done by asking the questionnaire. The relevant questionnaire has been prepared and piloted for its applicability, reliability, validity and consistency and then finalized. A detailed history was taken by preparing a questionnaire.
## III. RESULTS
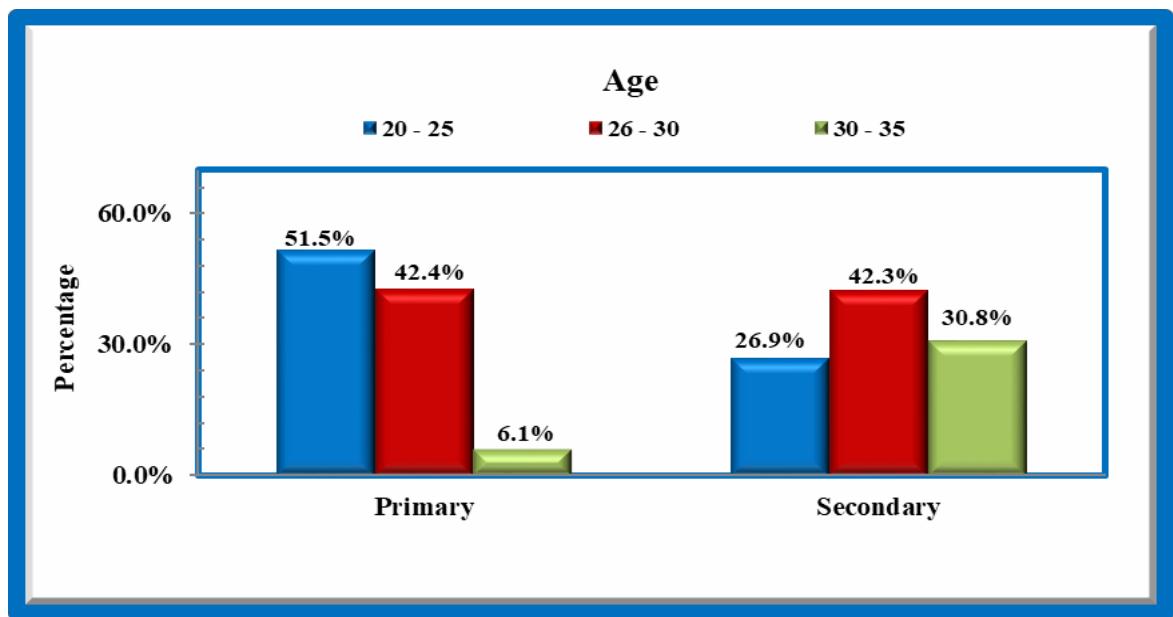
Most of $51.5\%$ women of primary infertility are in the age group 20-25 years. $42.4\%$ of primary and $42.3\%$ of secondary fall in the age group of 26-30yrs.In primary, significantly less numbers are in the age group 30-33yrs.
 GRAPH 2
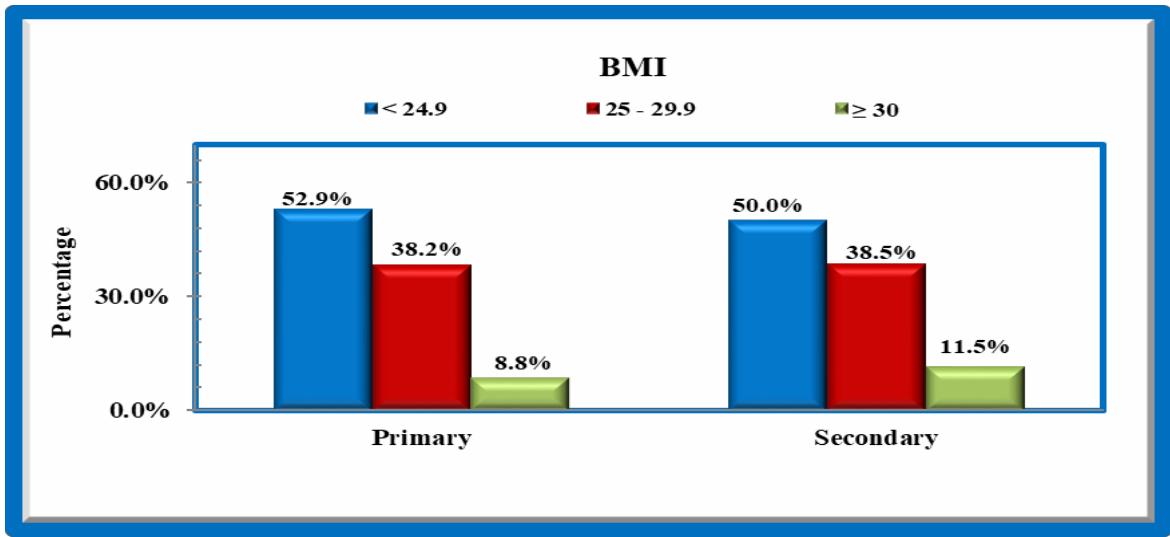
Majority are in grade 1 BMI, $52.9\%$ of primary and $50\%$ of secondary $.38.2\%$ of primary and $38.5\%$ of secondary belongs to grade 11 BMI.
 GRAPH 3
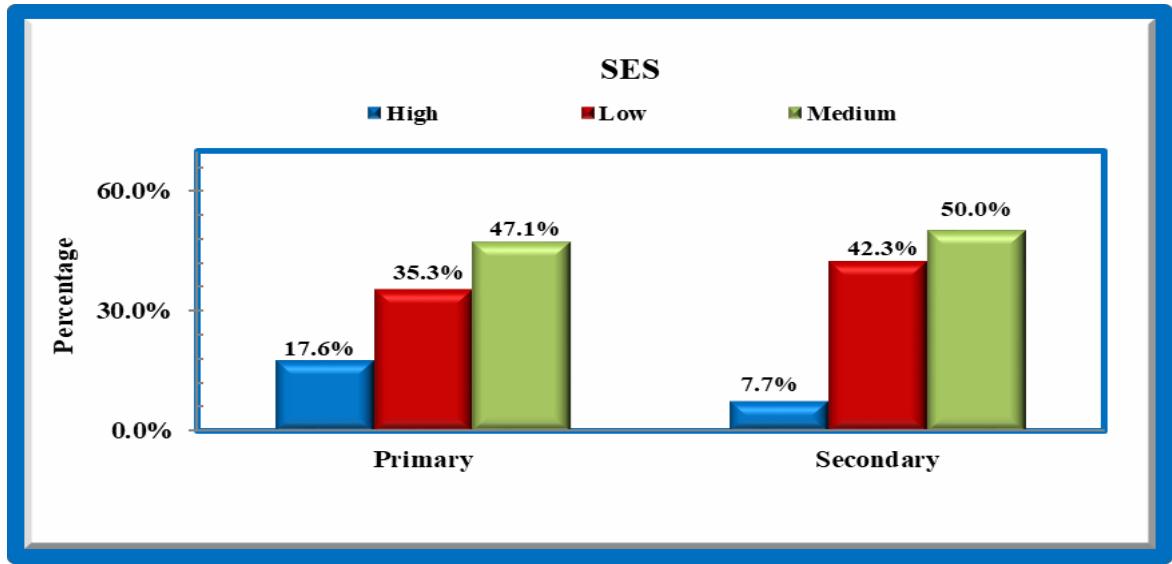
Majority belongs to middle socio economic status $47.1\%$ of primary and $50\%$ of secondary.
 GRAPH 4
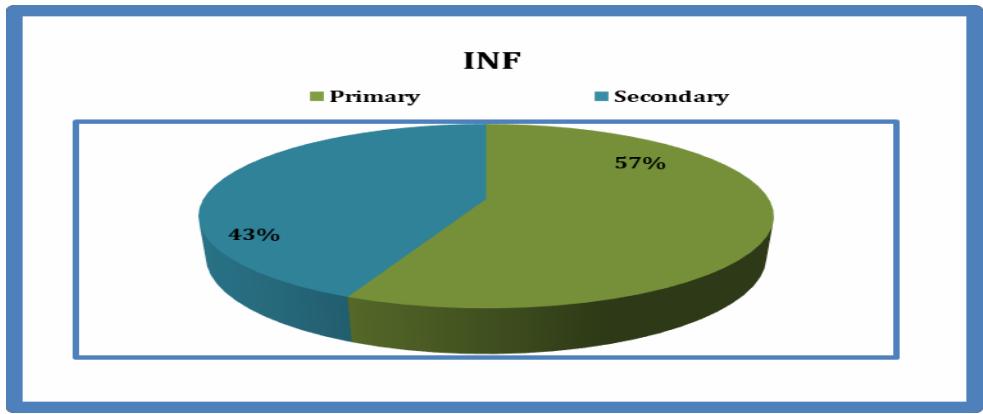
57% cases have primary infertility and 43% cases have secondary infertility.
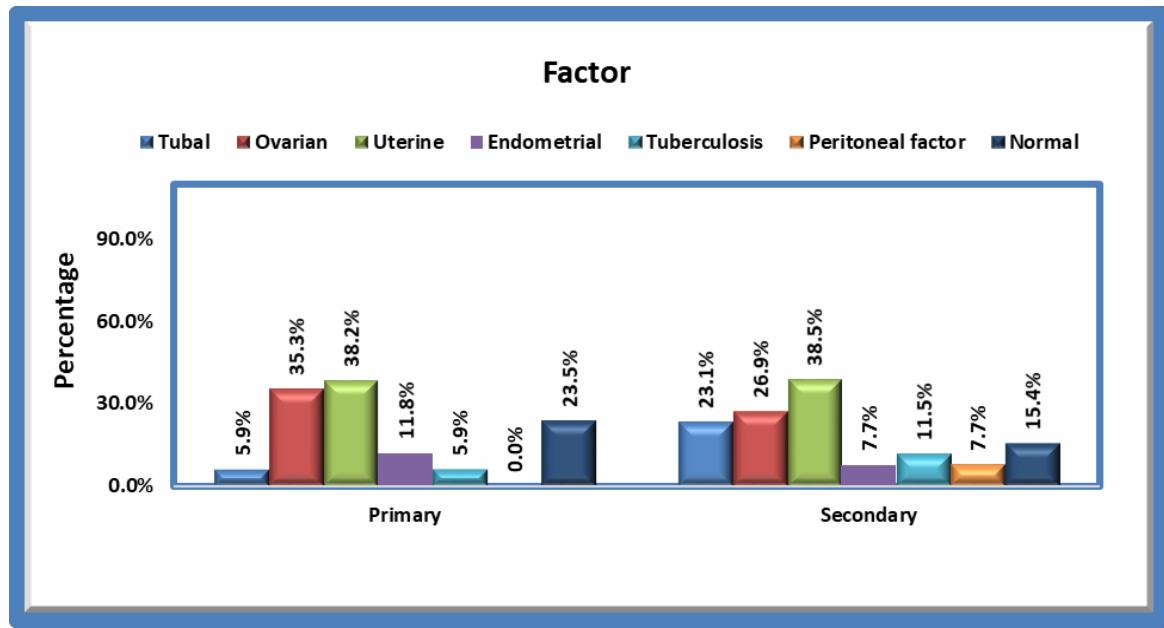 GRAPH 5 In $23.5\%$ cases of primary and $15.4\%$ cases of secondary infertility there is no obvious pathology. Tubal pathology is seen in $5.9\%$ and $23.1\%$ cases of primary and secondary, ovarian pathology is seen in $35.3\%$ and $26.9\%$ cases of primary and secondary. Uterine pathology contributes to $38.2\%$ and $38.5\%$ of primary and secondary infertility. Endometriosis $11.8\%$ and $7.7\%$ respectively, tuberculosis to about $5.9\%$ and $11.5\%$ of primary and secondary, peritoneal factors $7.7\%$ in secondary infertility.
 GRAPH 6
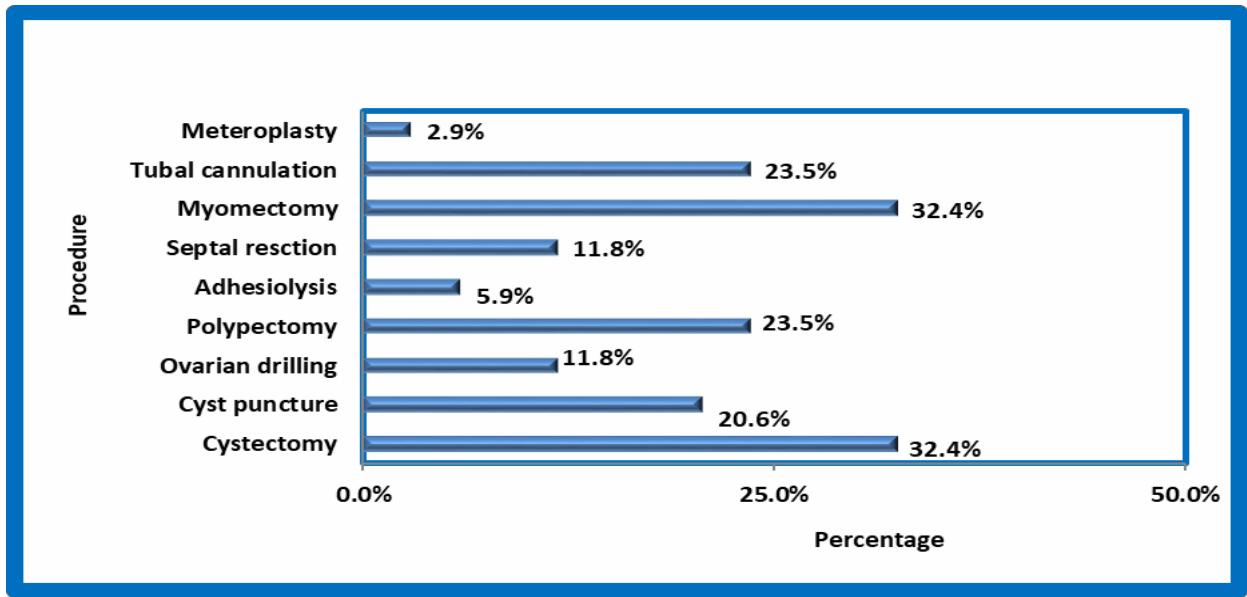
Distribution of cases according to procedure hysteroscopy and laparoscopy.
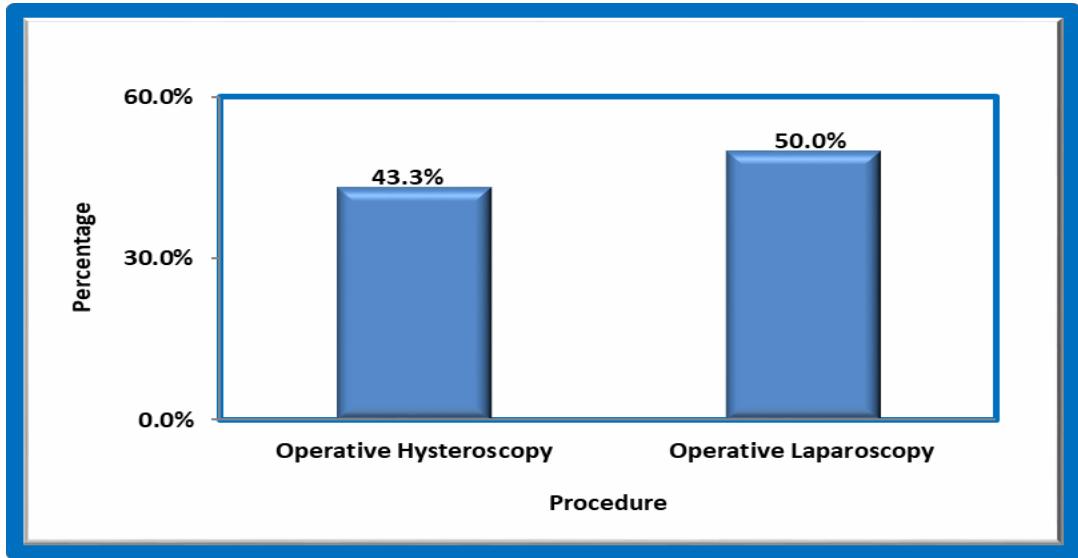 GRAPH 7
Operative Hysteroscopy is done in $43.3\%$ cases which constitute $23.5\%$ polypectomy, $5.9\%$ adhesiolysis, $11.8\%$ of septal resection, $32.4\%$ myomectomy, $23.5\%$ tubal cannulation.
Operative laparoscopy done in $50\%$ cases which constitute $32.4\%$ cystectomy, $11.8\%$ ovarian drilling, and cyst puncture of $20.6\%$.
## IV. DISCUSSION
Infertility is generally defined as one year of unprotected intercourse without conception. Approximately $85 - 90\%$ of healthy couples conceive within one year. Infertility therefore affects approximately $10 - 15\%$ of couples.
Laparoscopy is considered as the gold standard for diagnosing tubal and peritoneal disease. It is trans peritoneal endoscopic technique that provides direct visualization of pelvis and complete view of cul de sac, pelvic side walls and all the pelvic viscera. Hysteroscopy is a procedure that involves the insertion of an endoscope through the cervical canal into the uterine cavity and distension media to allow for visualization.
Hystero-laparoscopy is minimally invasive technique reaching new horizons in management of infertile patients. Direct visualization with optical magnification has an added advantage of diagnosing pathologies which cannot be picked up in ultrasound and other radiological tests.
The Study is conducted at Muslim maternity hospital who attended the infertility department from: JUNE 2018 - MAY 2019.
Age: In the current study majority of infertile women are in the age group of 20- 30yrs. Primary infertility majority are in 20-25yrs (51.5%) and secondary infertility majority are in 26-30yrs (42.3%). According to Gufareen et al (2010) $55\%$ had primary in the age group of 20-25yrs, $60\%$ had secondary in 26-33yrs which is nearly similar to current study.
Socioeconomic Status: In the current study most of primary infertile women $47.1\%$ belong to middle socio economic status, most of secondary infertile women belong to both low and middle socio economic status $42.3\%$ and $50.0\%$ respectively. Only $17.6\%$ of primary infertile and $7.7\%$ of secondary infertile women belong to high socio economic status. According to Nadia et al (2011) $65\%$ of primary and $40\%$ of secondary belong to low to middle socio economic status which is similar to current study.
Type of Infertility: In the current study primary infertility is $57\%$ and secondary infertility is $43\%$ which is almost similar to studies done by Erhong Zhang1et. al $^{12}$ (2014) $53.8\%$ women had primary infertility and $46.2\%$ had secondary infertility, jamshoro et al (2010) $64\%$ in primary and $36\%$ in secondary and Nadia et al(2011) $63\%$ in primary $37\%$ in secondary.
Tubal Factors: Hysteroscopy and laparoscopy are the two methods for evaluation and treatment of tubal pathology and are complementary to each other.
In the current study, hydrosalpinx is $2.9\%$ in primary and $7.7\%$ in secondary, which is similar to the studies done by Saima et al (2010), $4\%$ in primary and $16\%$ in secondary infertile women, whereas lead pipe and kinked tubes are $2.9\%$ in primary and $7.7\%$ in secondary which is similar to the studies done by jamshoro et al (2010) $3\%$ in primary and $16.7\%$ in secondary infertile women and many tubal blocks were demonstrated on sono hysterosalpingography, but the tubal patency was demonstrated on laparoscopic chromo perturbation by the release of tubal spasm and minor blocks which were cleared by selective tubal cannulation and tubal patency was established, Also, edematous tubes are seen only in secondary infertility $7.7\%$ and also there are absent tubes due to previous surgeries which is about $15.4\%$.
Ovarian Factors: In the current study, polycystic ovarian syndrome contribute to $24\%$ and $20\%$ in primary and secondary infertility which is similar when compared to the study of Saima et al (2010) $28\%$ in primary and $12\%$ in secondary.
Uterine Factors: Developmental uterine anomalies have long been associated with pregnancy loss and obstetric complications, but the ability to conceive is generally not affected. In the current study anomalous uterus is $4\%$ in primary which is less when compared to study of Vidya et al (2011) where it is $14\%$ in primary. Anomalous uterus in total contribute to $8.8\%$ of infertility which is similar to Boricha et al (2011) $11\%$ but less compared to Sajida et al $^{13}$ (2009) $13\%$. In my study most common of anomalous uterus is septate uterus. In modern operative hysteroscopic techniques, septal resection was done in my hospital and everywhere nowadays. Other than septate uterus, other uterine anomalies were arcuate uterus and didelphus uterus. Other causes such as ashermanns syndrome, fibroids and polyps are also found.
Endometriosis: In the current study, endometriosis contributed to $11.8\%$ of infertility which is similar to Sarkar et al. (2008) and Javid et al. (2009) $15\%$ but less when compared with the studies done by Boricha et al. (2011) and Sajida et al. (2009) where they estimated as $22\%$ and $20\%$ respectively.
Peritoneal Causes: In the current study peritoneal factors contribute to $7.7\%$ in secondary which is less compared to the studies done by Jamsharoo et al. estimated $22.2\%$, Nausheen et al. (2010) estimated $22.2\%$. Saima et al. (2010) estimated $16\%$.
In Re-Evaluation: of already treated cases, many factors were seen by diagnostic hystero-laparoscopy among which stenosed cervical os and abnormally directed cervical canal were found in a few cases, which were treated by dilatation of the os and uterine factors were septate uterus, endometrial polyps and the narrow uterine cavity, which were managed accordingly by septoplasty, polypectomy and metroplasty respectively. On laparoscopy, other causes were pelvic tuberculosis, pelvic disease and endometriosis. Tubal factors were tubal blocks, adhesions and inflamed tubes, which were managed accordingly.
Management: In the current study operative hysteroscopy was performed in $43.3\%$, operative laparoscopy was performed in $50\%$, which is similar to the studies done by Boudrak et al. (2008) they performed $27.3\%$ and $70\%$ of operative hysteroscopy and laparoscopy respectively, also tubal surgeries were done in $23.5\%$ of cases, ovarian drilling in $11.8\%$, excision of cyst in $32.4\%$, cyst puncture in $20.6\%$, polypectomy in $23.5\%$, adhesiolysis in $5.9\%$, septal resection in $11.8\%$, myomectomy in $32.8\%$. Boudhraak et al $^{4}$. (2008) studies shows that adhesiolysis $(27.2\%)$, excision of cyst $(17.2\%)$, ovarian drilling $(17.8\%)$ and tubal surgeries $(37\%)$ which is similar to current study except for tubal surgeries. Boricha et al (2011) studies shows that adhesiolysis in $13.63\%$, cystectomy in $13.63\%$, cyst puncture in $22.72\%$, ovarian drilling in $40\%$. Cases that were diagnosed to have tubal pathology due to Kochs, PID or tubal blocks secondary to extensive endometriosis were directly advised for ART procedure.
## V. CONCLUSION
In the investigation of cases of infertility, normal semen analysis of husband, routine traditional investigation of tubal patency, and endometrial biopsy, ovulation study, cervical factor study, are not the end points. The investigation is incomplete without an evaluation of the exact cause of infertility.
The traditional tests of tubal patency may be false negative due to tubal spasm, which were overcome in chromopertubation test in laparoscopy, which not only gives additional information about the exact site of block and the pathology behind, but also serves the purpose of treatment by doing adhesiolysis.
Laparoscopy also gives the exact picture of the morphology of the ovaries and the periovarian adhesions, at the same time has a role of treatment in the form of multiple drillings of the polycystic ovaries, endometriotic spots cauterization, adhesiolysis and evidence of ovulation can be confirmed by the presence of corpus luteum.
Laparoscopy also gives the picture of the abnormalities of uterus, about the peritoneum, and about endometriosis, which can be treated in the same sitting by electrocautery.
Hysteroscopy gives a good picture of the intracervical and intrauterine pathology and in addition to this diagnostic role, it has a therapeutic role to perform in releasing intrauterine adhesions, releasing cornual blocks by chromopertubation, tubal cannulation, and excision of endometrial polyps, fibroids, septum and an endometrial biopsy can be taken at the same sitting for hormonal assay.
The incidence of various pathological conditions are $23.5\%$ cases of primary and $15.4\%$ cases of secondary infertility, there is no obvious pathology. Tubal pathology is seen in $5.9\%$ and $23.1\%$ cases of primary and secondary, ovarian pathology is seen in $35.3\%$ and $26.9\%$ cases of primary and secondary. Uterine pathology contributes to $38.2\%$ and $38.5\%$ of primary and secondary. Endometriosis $11.8\%$ and $7.7\%$ respectively, tuberculosis to about $5.9\%$ and $11.5\%$ of primary and secondary, peritoneal factors $7.7\%$ in secondary infertility.
The etiology found in reevaluated cases were stenosed cervical os, abnormally directed cervical canal, septate uterus, endometrial polyps, narrow uterine cavity, pelvic tuberculosis, pelvic disease, endometriosis, tubal blocks, adhesions and inflamed tubes. Operative procedures were carried out in the same sitting to get optimal outcome.
To conclude an investigation of female infertility is incomplete without a Hystero-laparoscopy, as all the exact etiology which may be of the ovarian, tubal, uterine, peritoneal, endometriotic, cervical, causes can be known, and in addition treatment for these causes can also be offered in the same sitting.
Author Contributions
Funding - None
Conflict of interest
The authors declare that they have no conflict of interest.
Generating HTML Viewer...
References
13 Cites in Article
A Gour,A Zawiejska,L Mettler (2008). Hysteroscopycurrent trends and challenges.
Tarek Shokeir,Hesham Shalan,Mohamed El‐shafei (2004). Combined diagnostic approach of laparoscopy and hysteroscopy in the evaluation of female infertility: Results of 612 patients.
P Kaminski,M Gajewska,M Wielgos,I Szymusik,K Ziolkowska,R Bartkowiak (2006). The usefulness of laparoscopy and hysteroscopy in the diagnostics and treatment of infertility.
Chetana Gopchade (2009). Role of Diagnostic Laparoscopy in Cases with Female Infertility.
Zulfo Godinjak,Edin Idrizbegović (2008). Should Diagnostic Hysteroscopy be a Routine Procedure During Diagnostic Laparoscopy in Infertile Women?.
J Hucke,F De,P Balan (2000). Hysteroscopy in infertility-diagnosis and treatment including falloposcopy.
W Ombelet,I Cooke,S Dyer,G Serour,P Devroey (2008). Infertility and the provision of infertility medical services in developing countries.
Prasanta Nayak,Purna Mahapatra,J Mallick,S Swain,Subarna Mitra,Jayaprakash Sahoo (2013). Role of diagnostic hystero-laparoscopy in the evaluation of infertility: A retrospective study of 300 patients.
E Zhang,Y Zhang,L Fang,Q Li,J Gu (2014). Combined hysterolaparoscopy for the diagnosis of female infertility: a retrospective study of 132 patients in china.
S Parveen,M Khanam (2010). Role of combined diagnostic laparoscopy and simultaneous diagnostic hysteroscopy for evaluation of female subfertility factors.
N Khurshid,F Sadiq,Iftikhar Consecutive 300 Diagnostic Laparoscopies at Arif Memorial Teaching Hospital.
P Adamson,K Krupp,A Freeman,J Klausner,A Reingold,P Madhivanan (2011). Prevalence & correlates of primary infertility among young women in Mysore, India.
Van Herendael,B (1995). Instrumentation in hysteroscopy.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Ruheena Nakhuda. 2026. \u201cEvaluation of Infertility Cases Attending Tertiary Care Centre with Hystero-Laparoscopy\u201d. Global Journal of Medical Research - E: Gynecology & Obstetrics GJMR-E Volume 25 (GJMR Volume 25 Issue E1): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.