## I. INTRODUCTION
Coronavirus disease (Covid-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a pandemic that has resulted in several thousand confirmed cases and deaths. (2). The mortality rate around the world shows variations that merit evaluation (2). It has been shown that comorbidities are frequently associated with Covid-19 and constitute risk factors for the severity of the disease (3).
In their study, Sina et al found that risk factors are associated with morbidity and mortality of CHD 2019 in several countries, including Central and Eastern Europe, Bangladesh, Brazil, China, India, Iran, Pakistan and Turkey. They found that there were more confirmed cases and deaths among men than women in most of these countries (see reference by Sina et al). In addition, the case-fatality rate for men was higher than for women (4). There are factors associated with the occurrence of morbidity and mortality linked to Covid-19, but these morbidity and mortality phenomena are significantly lower in sub-Saharan Africa than in high-income countries (5, 6).
In sub-Saharan Africa, some authors have reported that non-communicable diseases (NCDs) are associated with the occurrence of mortality in patients with severe Covid19, notably cardiovascular disease (including hypertension) with a proportion of $24.6\%$, diabetes with $18.4\%$ and chronic obstructive pulmonary disease (asthma) with $5.3\%$. The data compiled by Skip LA et al to assess the epidemiological and clinical characteristics of the Covid-19 cases who died throughout the African region south of the Sahara. More specifically, data on sex, age, underlying conditions and mode of detection were associated with the occurrence of deaths (7). In Burkina Faso in 2020, they point out that nearly half of confirmed Covid19 cases had a history of hypertension $(45.5\%)$, diabetes $(21.2\%)$ or other cardiovascular or pulmonary conditions, such as stroke, embolism or heart disease $(9.1\%)$ (7). In Mali in 2021, Soumana et al showed that mortality in patients infected with was associated with factors such as obesity, diabetes, hypertension, COPD, smoking, immunosuppression and chronic renal failure (8). In Senegal in 2022, Maryam Diarra et al found that patients aged over 65 and those suffering from hypertension, cardiovascular disease and diabetes were strongly associated with death (9).
In response to the first case of the pandemic in Guinea, the country has set up care facilities. According to data from the Agence Nationale de Sécurité Sanitaire (ANSS) for August 2022, 733,221 tests have been carried out in the country, of which 37,496 have been confirmed, with a positivity index of $5.1\%$. 37,302 patients have been hospitalized in the various CT-Epi units, of whom 36,787 have been cured, representing a cure rate of $98.1\%$. A total of 785 deaths due to Covid-19 were recorded, including 447 hospital deaths (10).
Despite the evidence of the association between comorbidities and the occurrence of morbidity and mortality in Covid-19-infected patients, there is insufficient information on the factors influencing the mortality of Covid-19-infected patients with comorbidities in the epidemiological treatment centers of Conakry in Guinea from 2020 to 2022. It therefore seems appropriate to analyze the factors associated with mortality in Covid-19-infected patients hospitalized in Conakry's CT-Epi from 2020 to 2022.
## II. MATERIALS AND METHODS
### a) Study Sites
The CT-Epi of Donka, Gbessia and Camp Alpha Yaya DIALLO served as the setting for our study. These CT-Epi are part of the six (06) epidemiological treatment centers in the capital Conakry, namely Nongo, Camp Alpha Yaya, Gbessia, Maison Centrale, Donka and Kenien. (21).
### b) Study Design
Secondary data collected in the Conakry CT-Epi on patients infected with Covid-19 from 12 March 2020 to 31 December 2022 were analyzed.
### c) Target Population
Suspected cases of Covid-19 who were hospitalized in three CT-Epi in Conakry, namely Donka, Gbessia and Camp Alpha Yaya during the collection period.
### d) Study Population
The study population consisted of all patients infected with Covid-19 confirmed by Gold standard RT-PCR and hospitalized in CT-Epi.
### e) Calculating Statistical Power
The sample size was 820 disabled people aged between 15 and 60 and the statistical power of this sample was calculated using the following parameters:
$$
For: n=10404
$$
The first-species error $\alpha = 0.05$
- An expected prevalence of 0.4
- An observed prevalence of 0.5
This gives a statistical power of $(1 - \beta) = 99\%$.
### f) Choice of Variables
## i. Dependent Variable
The dependent variable in this study was death, which was measured in people infected with Covid-19 and hospitalized at the Donka, Gbessia and Camp Alpha Yaya CT-Epi in Conakry.
## ii. Independent Variables
The variables were age, sex, marital status, level of education, patient residence, diabetes alone, hypertension alone, HIV alone, TB alone, chronic respiratory diseases, associated comorbidities and epidemiological treatment centers (CT-Epi).
### g) Operational Organization of Data Collection
A secondary analysis of the data collected on patients infected with COVID-19 was performed. The main objective of this study was to analyze the factors associated with mortality in patients infected with Covid-19 at the Gbessia epidemiological treatment center in Conakry, Republic of Guinea.
Ethical Considerations
Data collection was approved by the National Health Research Ethics Committee of the Republic of Guinea.
## III. DATA PROCESSING
The study data were collected in the Donka, Gbessia and Camp Alpha Yaya CT-Epi in Conakry. They were used for this work. After exploration of this database, our variables were selected. The selected variables were recorded in accordance with the different predefined modalities. The dependent variable was formed from the death variable. Out of a total of 10,416 observations, twelve (12) variables (marital status, profession, level of education and residence of patients, etc.) had missing values. Given the high proportion of missing values (over $15\%$ ), it was decided to exclude them from our analysis.
## IV. DATA ANALYSIS
The first stage of the analysis was a descriptive analysis of all the selected variables. The sociodemographic characteristics of the study subjects were described. Numbers and percentages were calculated for each qualitative variable selected and compared using Pearson's chi2 test.
The bivariate analysis consisted of estimating the association between the dependent variable and each of the selected independent variables using simple logistic regression. This analysis yielded crude Odds Ratios (OR) with their $95\%$ confidence intervals (CI). A significance level of $0.2\%$ was used to include the explanatory variables in the final model.
For the multivariate analysis, a standard multivariate binary logistic regression was used to analyze the factors associated with mortality in patients infected with Covid-19, yielding adjusted odds ratios (AORs). A p value $< 0.05$ was considered statistically significant.
## V. RESULTS
We included 10,404 Covid-19-infected patients hospitalized in the epidemiological treatment centers in Conakry in our analysis.
Table I presents some socio-demographic characteristics and the distribution of patients infected with COVID-19 hospitalized in the Conakry CT-EPI. Males were more represented with a proportion of $61.6\%$, and the 0-39 age group was the most represented with $52.4\%$. The Donka CT-Epi had the highest number of hospitalized patients with a percentage of $87.9\%$. Approximately $6\%$ of patients had a co-morbidity.
Table I: Description of Covid-19-Infected Patients Hospitalized in Conakry's CT-Epis, 2020-2022 Figure 3 shows the proportion of deaths among Covid-19 patients hospitalized in Conakry's CT-EPI. $6\%$ of hospitalized patients died during the study period.
<table><tr><td>Variables</td><td>Number (N=10,404)</td><td>Percentage (%)</td></tr><tr><td>Gender</td><td></td><td></td></tr><tr><td rowspan="2">Male Female</td><td>6408</td><td>61,59</td></tr><tr><td>3996</td><td>38,41</td></tr><tr><td>Age (year) 0 -39</td><td></td><td></td></tr><tr><td>40-59</td><td>5422</td><td>52,11</td></tr><tr><td rowspan="2">60 and over</td><td>2847</td><td>27,36</td></tr><tr><td>2135</td><td>20,52</td></tr><tr><td>CT-EPI</td><td></td><td></td></tr><tr><td>Donka</td><td>9145</td><td>87,90</td></tr><tr><td rowspan="2">Camp AlphaYaya Gbessia</td><td>749</td><td>7,20</td></tr><tr><td>510</td><td>4,90</td></tr><tr><td>Comorbidities</td><td></td><td></td></tr><tr><td>No</td><td>9778</td><td>93,98</td></tr><tr><td>Yes</td><td>626</td><td>6,02</td></tr></table>
 Proportionofdeaths Figure 1: Proportion of Deaths among Covid-19-Infected Patients Hospitalized In Conakry's CT-EPI, 2020-2022
Table III shows the distribution of deaths among patients hospitalized in the Conakry CT-EPI according to characteristics. The age group 60 years and over was the most represented with $66.3\%$. More than half $(51.9\%)$ occurred in the Gbessia CT-EPI. The proportion of deaths due to comorbidities was $43.7\%$.
Table II: Breakdown of Deaths among Covid-19-Infected Patients Hospitalized in Conakry's CT-EPI By Characteristics, 2020- 2022
<table><tr><td rowspan="2">Variables</td><td colspan="2">DEATH</td><td rowspan="2">p</td></tr><tr><td>Number (N=618)</td><td>Percentage (%)</td></tr><tr><td>Gender</td><td></td><td></td><td></td></tr><tr><td>Male Female</td><td>387</td><td>62,62</td><td></td></tr><tr><td></td><td>231</td><td>37,38</td><td></td></tr><tr><td></td><td></td><td></td><td>0,587</td></tr><tr><td>Age (year)</td><td></td><td></td><td></td></tr><tr><td>0 -39</td><td>69</td><td>11,17</td><td></td></tr><tr><td>40-59</td><td>139</td><td>22,49</td><td></td></tr><tr><td>60 and over</td><td>410</td><td>66,34</td><td><0,001</td></tr><tr><td>CT-EPI</td><td></td><td></td><td></td></tr><tr><td>Donka</td><td>291</td><td>47,08</td><td></td></tr><tr><td>Camp Alpha Yaya</td><td>6</td><td>0,97</td><td></td></tr><tr><td>Gbessia</td><td>321</td><td>51,94</td><td><0,001</td></tr><tr><td>Comorbidities</td><td></td><td></td><td></td></tr><tr><td>No</td><td>348</td><td>56,31</td><td></td></tr><tr><td>Yes</td><td>270</td><td>43,69</td><td><0,001</td></tr></table>
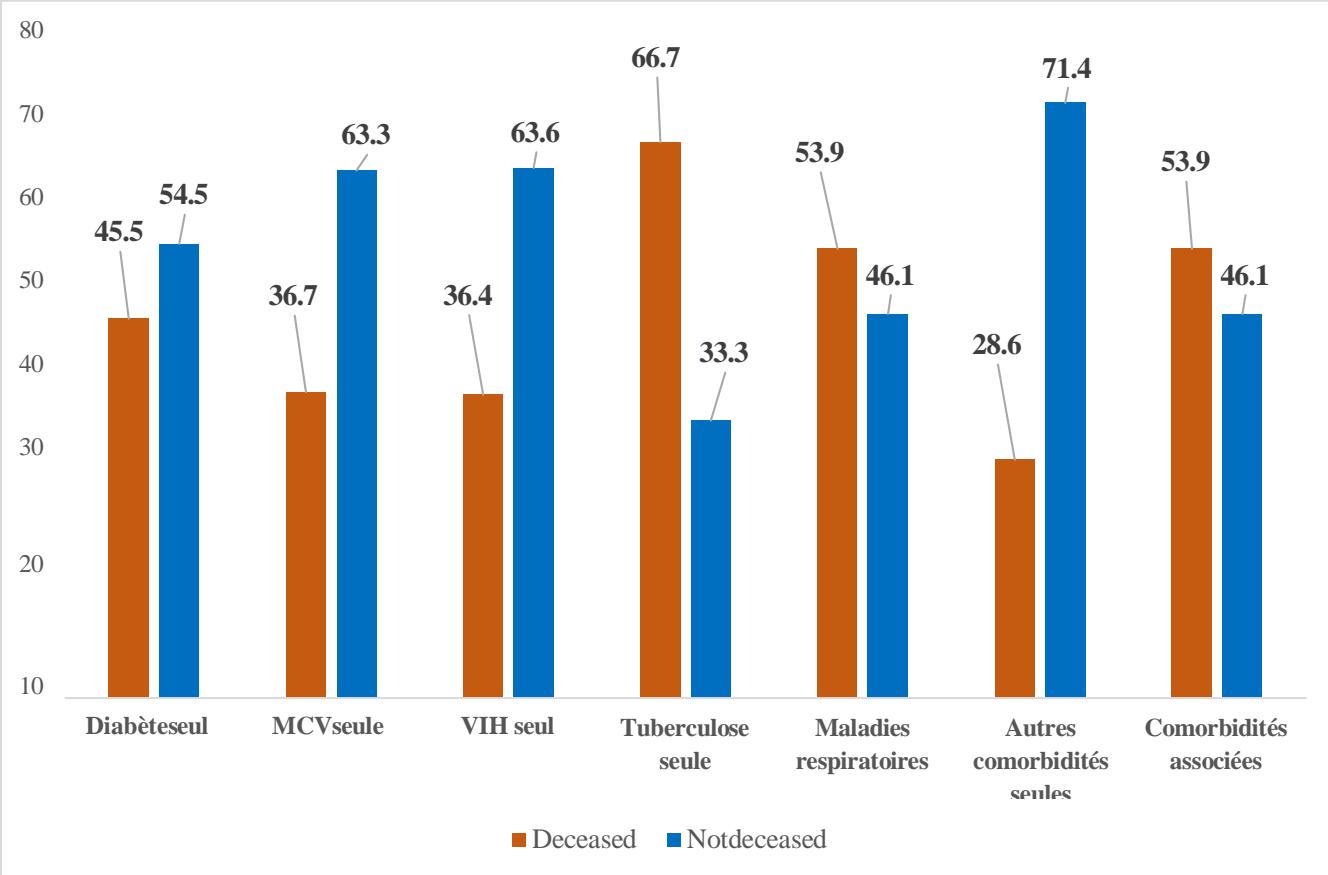
Figure 4 shows the distribution of deaths by type of comorbidity. Around $45\%$ of patients with diabetes alone died. More than a third $(36.7\%)$ of patients with cardiovascular disease alone and $36.4\%$ of patients with HIV alone died. Two-thirds (66.7%) of patients with tuberculosis alone died. More than half of the patients with respiratory diseases alone (53.8%) and associated comorbidities (53.9%) had died.
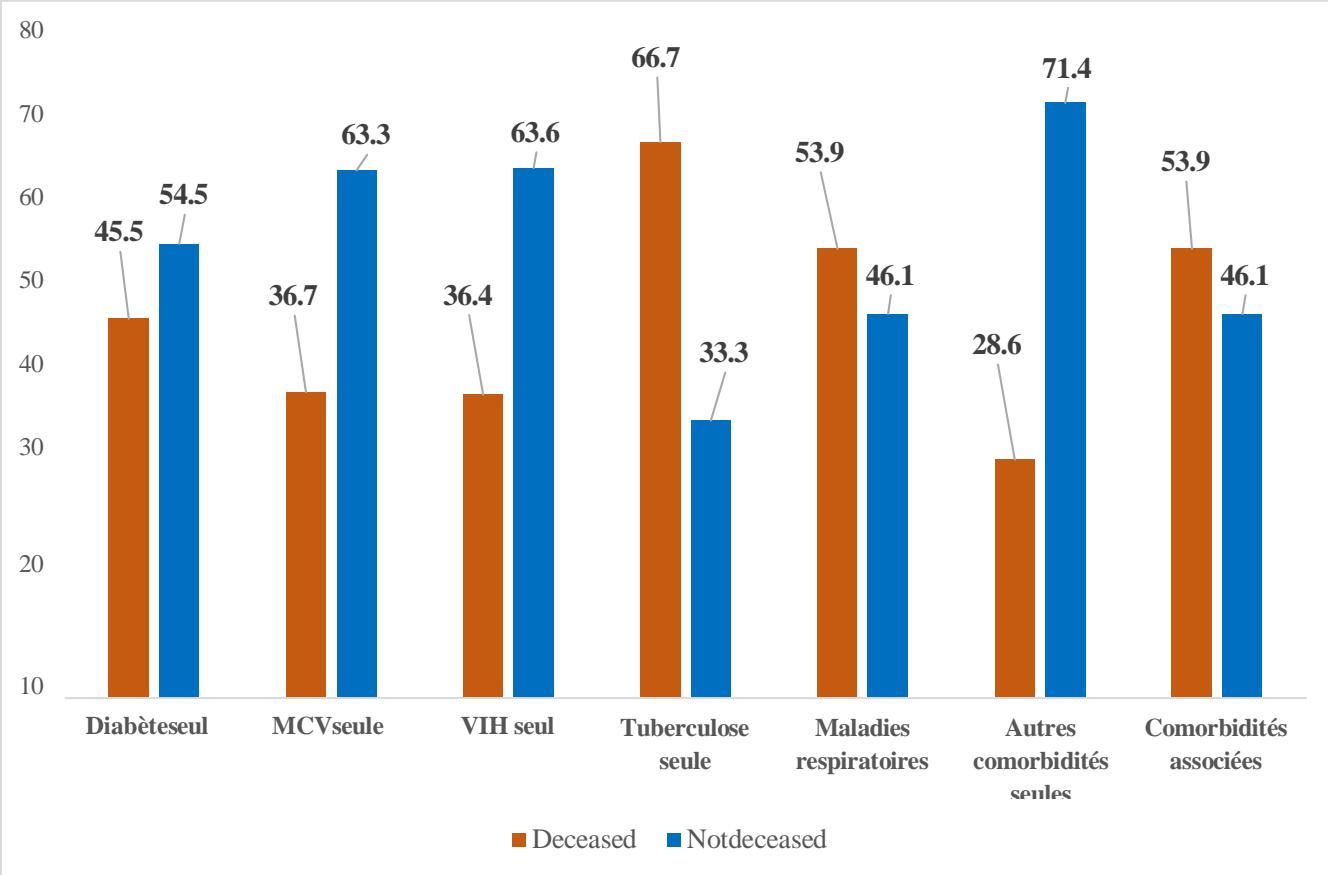 Figure 2: Proportion of Deaths by Type of Comorbidity among Covid-19-Infected Patients Hospitalized in Conakry's CT-EPI, 2020 - 2022 (N = 10404)
Table IV shows the results of the bivariate logistic regression analysis. In the univariate analysis, the variables significantly associated with death in patients infected with Covid-19 were age, CT-Epi, diabetes alone, HIV alone, TB alone, chronic respiratory disease alone, other comorbidities alone and associated comorbidities.
Compared with Covid-19 patients aged 0-39 years, patients aged 40-59 years and 60 years and over were respectively 4 times (OR= 3.98; CI $95\% = 2.97 - 5.33$; p= 0.000) and 19 times (OR=19.05; CI $95\% = 14.67 - 24.72$; p= 0.000) more likely to die from Covid-19. Compared with Covid-19-infected patients hospitalized at the Donka National Hospital, patients hospitalized at the Gbessia CT-Epi were 18 times more likely to die from their disease (OR=18.90; 95% CI = [13.70 - 26.08] p= 0.000). In contrast, patients hospitalized at the CT-Epi in the Alpha Yaya camp had a 75% lower probability of dying than patients hospitalized in Donka (OR = 0.25; 95% CI = [0.11- 0.55] p= 0.000).
Compared with non-diabetic Covid-19-infected patients, patients with diabetes alone had 13 times the risk of dying from Covid-19 (OR = 13.81; 95% CI = [8.45 - 22.60] p= 0.000). Compared with uninfected patients, patients infected with HIV alone were 9 times (OR = 9.21; 95% CI = [4.5 - 18.80] p= 0.000) more likely to die from their infection; patients infected with TB alone were 32 times more likely (OR = 31.97; 95% CI = [7.98 - 128.14] p= 0.000); respiratory disease alone, 18 times more likely (OR = 18.67; 95% CI = [6.26 - 55.73] p= 0.000); other comorbidities alone, 6 times more likely (OR = 61.35; 95% CI = [1.23 - 32.80] p= 0.000) and associated comorbidities 22 times more likely (OR = 22.33; 95% CI = [16.74- 29.79] p= 0.000) to die from their condition.
Table III: Factors Associated with the Occurrence of Death among Covid-19-Infected Patients Hospitalized in Conakry's CT-Epi, 2020-2023 in Bivariate Analysis
<table><tr><td>Features</td><td colspan="2">Crude Odds ratio (95% CI)p</td></tr><tr><td>Gender</td><td></td><td></td></tr><tr><td>Male Female</td><td>Ref.</td><td></td></tr><tr><td></td><td>0,95(0,81-1,13)</td><td>0,587</td></tr><tr><td>Age</td><td></td><td></td></tr><tr><td>(year)</td><td>Ref.</td><td><0,001</td></tr><tr><td>0 - 39</td><td>3,98(2,97-5,33)</td><td><0,001</td></tr><tr><td>40-59</td><td>19,05(14,67-24,72)</td><td></td></tr><tr><td>60 and over</td><td></td><td></td></tr><tr><td>CT-EPI</td><td></td><td><0,001</td></tr><tr><td>Gbessia</td><td>51,68(41,71-64,03)</td><td><0,001</td></tr><tr><td>Camp Alpha Yaya Donka</td><td>0,25(0,11-0,55)</td><td></td></tr><tr><td></td><td>Ref.</td><td></td></tr><tr><td>Diabetes</td><td>Ref.</td><td><0,001</td></tr><tr><td>alone No</td><td>13,81(8,45-22,60)</td><td></td></tr><tr><td>Yes</td><td></td><td></td></tr><tr><td>CVD alone No</td><td></td><td></td></tr><tr><td>Yes</td><td>Ref.</td><td></td></tr><tr><td></td><td>10,79(8,33-13,99)</td><td><0,001</td></tr><tr><td>HIV</td><td>Ref.</td><td><0,001</td></tr><tr><td>Alone</td><td>9,21(4,51-18,80)</td><td></td></tr><tr><td>No</td><td></td><td></td></tr><tr><td>Yes</td><td></td><td></td></tr><tr><td>TB</td><td>Ref.</td><td></td></tr><tr><td>only No</td><td>31,97(7,98-128,14)</td><td><0,001</td></tr><tr><td>Yes</td><td></td><td></td></tr><tr><td>Respiratory disease</td><td>Ref.</td><td></td></tr><tr><td>alone No</td><td>18,67(6,26-55,73)</td><td><0,001</td></tr><tr><td>Yes</td><td></td><td></td></tr><tr><td>Other comorbidities</td><td>Ref.</td><td></td></tr><tr><td>alone No</td><td>6,35(1,23-32,80)</td><td>0,027</td></tr><tr><td>Yes</td><td></td><td></td></tr><tr><td>Associated</td><td>Ref.</td><td></td></tr><tr><td>comorbidities No</td><td>22,33(16,74-29,79)</td><td><0,001</td></tr><tr><td>Yes</td><td></td><td></td></tr></table>
Table V shows the results of the multivariate binary logistic regression analysis in explaining the occurrence of death in Covid- 19 infected patients. The variables age, CT-Epi, diabetes alone, CVD alone, HIV alone, TB alone, chronic respiratory disease alone, other comorbidities alone and associated comorbidities were reintroduced into the multivariate logistic regression model. This final model involved 10,404 observations. The explanatory variables that were significantly associated with death at a threshold $< 2\%$ were the age ranges of Covid-19 infected patients, CT-Epi, diabetes alone, HIV alone and associated comorbidities. Covid-19-infected patients in the 40-59 age bracket had a 3-fold increased risk of death (AOR = 2.99; CI95% = [2.17-4.10]; p = 0.01) and those aged 60 and over an
11-fold increased risk of death (AOR = 11.23; CI95% = [8.42-14.98]; p = 0.000) compared with Covid-19-infected patients in the 0-39 age bracket when adjusting for other factors.
Covid-19-infected patients hospitalized at the CT-Epi de Gbessia compared with those hospitalized at the Hopital National Donka had an 18-fold increased risk of death (AOR= 18.90; CI $95\%$ = [13.70- 26.08]; p = 0.000); holding other variables constant in the model. Covid-19 patients hospitalized at Camp Alpha CT-Epi had a $78\%$ lower risk of death (AOR=0.22; 95% CI = [0.09-0.50]; p=0.000), compared with those hospitalized at Donka National Hospital. Patients with
Covid-19 associated with diabetes alone had a 5-fold increased risk of death (OR =5.20; 95% CI = [2.45-11.04]; p = 0.000) compared with those without diabetes, holding other constants in the model. Patients with Covid-19 in combination with HIV alone had a 6-fold increased risk of death (OR =6.59; 95% CI = \[2.50-
17.40\]; $p = 0.000$ compared with those without HIV, adjusting for other variables. Patients with Covid-19 and several comorbidities had a 2-fold increased risk of death (OR =2.57; 95% CI = [1.66-4.00]; $p = 0.000$ ) compared with those without, adjusting for other variables.
Table IV: Factors Associated with the Occurrence of Death in Patients Infected with Covid-19 Hospitalized in Conakry's CT-Epi, 2020-2023, Multivariate Analysis
<table><tr><th>Features</th><th>Adjusted odds ratio (95% CI)</th><th>p</th></tr><tr><td colspan="3">Age (year) 0 -39</td></tr><tr><td>40-59</td><td>Ref.</td><td></td></tr><tr><td rowspan="2">60 and over</td><td>2,99 (2,17-4,10)</td><td><0,001</td></tr><tr><td>11,23 (8,42-14,98)</td><td><0,001</td></tr><tr><td colspan="3">CT-EPI</td></tr><tr><td>Gbessia</td><td>18,90 (13,70-26,08)</td><td><0,001</td></tr><tr><td rowspan="2">Camp Alpha Yaya Donka</td><td>0,22 (0,09-0,50)</td><td><0,001</td></tr><tr><td>Ref.</td><td></td></tr><tr><td colspan="3">Diabetes</td></tr><tr><td>alone No</td><td>Ref.</td><td></td></tr><tr><td>Yes</td><td>5,20 (2,45-11,04)</td><td><0,001</td></tr><tr><td colspan="3">CVD</td></tr><tr><td>alone No</td><td>Ref.</td><td></td></tr><tr><td>Yes</td><td>1,52(1,00-3,31)</td><td>0,052</td></tr><tr><td colspan="3">HIV</td></tr><tr><td>Alone</td><td>Ref.</td><td></td></tr><tr><td>No</td><td>6,59(2,50-17,40)</td><td><0,001</td></tr><tr><td>Yes</td><td></td><td></td></tr><tr><td colspan="3">Tuberculosis</td></tr><tr><td>alone No</td><td>Ref.</td><td></td></tr><tr><td>Yes</td><td>4,00(0,85-18,91)</td><td>0,080</td></tr><tr><td colspan="3">Chronic respiratory diseases</td></tr><tr><td>alone No</td><td>Ref.</td><td></td></tr><tr><td>Yes</td><td>0,93(0,27-3,25)</td><td>0,912</td></tr><tr><td colspan="3">Other comorbidities</td></tr><tr><td>alone No</td><td>Ref.</td><td></td></tr><tr><td>Yes</td><td>0,58(0,10-3,53)</td><td>0,555</td></tr><tr><td colspan="3">Associated comorbidities No</td></tr><tr><td>Yes</td><td>2,57(1,66-4,00)</td><td><0,001</td></tr></table>
## VI. DISCUSSION
The general objective of this study was to analyze the factors associated with mortality in patients with Covid-19 hospitalized in the Conakry CT-Epi in the Republic of Guinea from March 2020 to December 2022.
a) The Overall Prevalence of Mortality in the Covid-19 Infected Population Hospitalized in the Conakry CT-EPI
The death rate among Covid-19-infected patients hospitalized in Conakry's CT-Epi is not negligible, at $6\%$, but it is low compared with death rates in northern countries. This result may be linked to a younger population, which limits the risk and number of deaths, and a favorable climate (hot and humid), which reduces viral transmission. This death rate could be underestimated by the fact that several cases of death were notified at community level and were not included in the total number of deaths occurring in the CT-Epi.
This result is similar to those found by certain researchers in Africa, who reported the same realities in 2020, with an even lower number of deaths per standardized population (22). Although reduced, the trend is identical for North Africa, which has 5 times fewer cases and 10 times fewer deaths per standardized population than the regions of Europe (22). Other studies have documented the overall mortality of patients infected with Covid-19 at $5\%$, which is close to our result (23).
Overall prevalence of mortality due to co-morbidities in Covid-19 patients hospitalized in Conakry's CT-EPIs In our analysis, we found high proportions of co-morbidities among patients who died of Covid-19 in the Conakry CT-Epi. This could be explained by the realities of African countries, with the epidemiological transition from infectious diseases to chronic diseases and the precarious health situation. Our results are in line with previous research which has shown a high proportion of co-morbidities in patients who die of Covid-19. A study conducted in South Africa by Waasila Jassat et al (24) reported that in 2022, $37.4\%$ of patients who died from Covid-19 had hypertension, $27.4\%$ had diabetes, $9.1\%$ were living with HIV, $3.6\%$ had tuberculosis (24).
Laura Skrip et al demonstrated in Burkina Faso in 2020 that the presence of underlying conditions was high among cases of death in Covid-19 patients. They also pointed out that almost half of confirmed Covid-19 cases had a history of hypertension (45.5%), diabetes (21.2%) or other cardiovascular or pulmonary conditions, such as stroke, embolism or heart disease (9.1%). (7).
Factors associated with the occurrence of death in patients infected with COVID-19 hospitalized in the Conakry CT-Epi, multivariate analysis.
With regard to the risk factors for death associated with Covid-19 infection in patients, our study showed that the age groups of patients infected with Covid-19, the epidemiological treatment centers in Conakry (CT-Epi), diabetes alone, HIV alone and associated comorbidities accounted for this high case-fatality rate.
In our analysis, age groups appear to be risk factors for death among Covid-19 patients, with a more pronounced emphasis on the $60+$ age group, which is 11 times more likely to die. In our context, this excess mortality among elderly patients could be explained by the association of co-morbidities in elderly subjects, which would contribute to a decline in immunity and precarious health conditions. In Mali,
Bourahima Koné et al found that the age group [65-75] was the most affected, with $31.06\%$. (25). Kombila U. D. et al in Gabon in 2022, found that age over 65 was the main independent risk factor for death $(p < 0.001; \mathrm{OR} = 4.632 \mathrm{IC95\%}$ [2.243-9.565]) (26). Other authors have also shown clear evidence for the association between mortality in Covid-19 patients and age and have also explained that age is a risk factor for mortality (27).
The epidemiological treatment center (CT-Epi de Camp Alpha Yaya) appears in our study to be a protective factor for hospitalized patients infected with Covid-19. However, another treatment center (CT-Epi de Gbesia) appears to be a risk factor for patients. It should be noted that we did not find any data in the scientific literature concerning the treatment centers for hospitalized patients infected with Covid-19. However, it should be noted that the CT-Epi at Camp Alpha Yaya did not have a resuscitation unit for the management of severe cases, so all severe cases from the CT-Epi at Camp Alpha Yaya were referred to the CT-Epi at Gbessia.
According to a multicenter study carried out by the World Health Organization (WHO) in 2020, prevention and treatment services for non-communicable diseases (NCDs) with co-morbidities have been severely disrupted since the start of the Covid-19 pandemic. This study was carried out in 155 countries by the WHO, which confirms that the impact is global, but that low-income countries in sub-Saharan Africa are the hardest hit. Health services have been partially or completely disrupted in many countries. This situation exposes patients suffering from NCDs (diabetes, arterial hypertension, heart disease, kidney disease, obesity, etc.) to the risk of serious illness and death due to Covid-19. In more than half $(53\%)$ of the countries responding to the survey, hypertension treatment services are partially or totally disorganized; in $49\%$ of countries, services for treating diabetes and its complications are disorganized; in $42\%$ of countries, cancer treatment services are disorganized; and in $31\%$ of countries, cardiovascular emergency services are disorganized. (28).
In Yaoundé, Mendimi Nkodo J.M et al also explained in their analysis that the risk of death was higher in infected patients with a combination of comorbidities such as arterial hypertension, diabetes, cardiovascular disease, obesity, chronic kidney disease, tuberculosis, HIV, etc., which undoubtedly explains the systemic dysfunction of the blood microcirculation in the lungs and other organs. (29).
A study carried out in South Africa by Waasila Jassat et al (24) reported that among patients who died in 2022 from Covid-19: $37.4\%$ had hypertension, $27.4\%$ had diabetes, $9.1\%$ were living with HIV and $3.6\%$ had tuberculosis. It also found that other associated factors were chronic heart disease, chronic kidney disease, etc.
(24). For Peter et al in South Africa in 2020, the triple burden of Covid-19, tuberculosis and the human immunodeficiency virus is one of the major global health challenges of the 21st century. Tuberculosis is a risk factor for Covid-19 in terms of both severity and mortality (30).
## VII. LIMITATIONS OF THE STUDY
Our study was based on collected data, and we came up against shortcomings in filling in the forms, which made it impossible to use information on gender, level of education, profession, economic level and place of residence. The type of study used in our work is a cross-sectional survey which makes it possible to establish an association between death and the various explanatory variables but cannot establish a causal link. Despite its limitations, this study has the merit of laying the foundations for an analysis of the factors associated with death in Covid-19-infected patients hospitalized in the epidemiological treatment centers in Conakry.
## VIII. CONCLUSION
Our study determined the factors associated with the occurrence of death in Covid-19-infected patients hospitalized in the Conakry epidemiological treatment centers from 2020 to 2022. The age groups of patients infected with Covid-19, the epidemiological treatment centers in Conakry (CT-Epi), diabetes alone, HIV alone and associated comorbidities are variables that influence the occurrence of death in patients infected with Covid-19. Further quantitative and qualitative research is needed to determine the best means of correctly measuring and also determining the factors associated with death in patients with co-infection comorbidities and Covid-19, who constitute a vulnerable population.
Generating HTML Viewer...
References
29 Cites in Article
A Sanyaolu,C Okorie,A Marinkovic,R Patidar (2020). Comorbidity and its Impact on Patients with COVID-19.
Adebayo Otitoloju,Ifeoma Okafor,Mayowa Fasona,Kafilat Bawa-Allah,Chukwuemeka Isanbor,Onyeka Chukwudozie,Olawale Folarin,Taiwo Adubi,Temitope Sogbanmu,Anthony Ogbeibu (2020). COVID-19 pandemic: examining the faces of spatial differences in the morbidity and mortality in sub-Saharan Africa, Europe and USA.
A Lounici,A Benmekki,A Ghenou,S Tahir,A Belmimoune,S Zini (2021). Clinical characteristics of diabetic patients hospitalised for Covid-19 over a one-year period.
Sina Tazerji,Fatemeh Shahabinejad,Mahya Tokasi,Mohammad Rad,Muhammad Khan,Muhammad Safdar,Krzysztof Filipiak,Lukasz Szarpak,Tomasz Dzieciatkowski,Jan Jurgiel,Phelipe Duarte,Md. Rahman,Md. Sobur,Md. Islam,Adnan Ahmed,Mohamed Shaheen,Awad Shehata,Rasha Gharieb,Mohamed Fawzy,Yashpal Malik,Nagaraj Jaganathasamy,Vinodhkumar Rajendran,Kannan Subbaram,P Ali,Sheeza Ali,Saif Rehman,Mehmet Ozaslan,Gulfaraz Khan,Muhammad Saeed,Umair Younas,Safdar Imran,Yasmeen Junejo,Parmida Arabkarami,Unarose Hogan,Alfonso Rodriguez-Morales (2022). Global data analysis and risk factors associated with morbidity and mortality of COVID-19.
Binta Diop,Marieme Ngom,Clémence Pougué Biyong,John Pougué Biyong (2020). The relatively young and rural population may limit the spread and severity of COVID-19 in Africa: a modelling study.
M Njenga,Jeanette Dawa,Mark Nanyingi,John Gachohi,Isaac Ngere,Michael Letko,C Otieno,Bronwyn Gunn,Eric Osoro (2020). Why is There Low Morbidity and Mortality of COVID-19 in Africa?.
Laura Skrip,Prashanth Selvaraj,Brittany Hagedorn,Andre Ouédraogo,Navideh Noori,Amanda Orcutt,Dina Mistry,Jamie Bedson,Laurent Hébert-Dufresne,Samuel Scarpino,Benjamin Althouse (2021). Seeding COVID-19 across Sub-Saharan Africa: An Analysis of Reported Importation Events across 49 Countries.
C Soumana,M Youssouf,C Mr,D Mahamane,D Mr,B Massaoulé (2021). Organ dysfunction during sars-cov-2 respiratory infection in Mali.
Noémie Legendre (2022). Une nouvelle agence de sécurité sanitaire.
Jasper Fuk-Woo Chan,Shuofeng Yuan,Kin-Hang Kok,Kelvin Kai-Wang To,Hin Chu,Jin Yang,Fanfan Xing,Jieling Liu,Cyril Chik-Yan Yip,Rosana Wing-Shan Poon,Hoi-Wah Tsoi,Simon Kam-Fai Lo,Kwok-Hung Chan,Vincent Kwok-Man Poon,Wan-Mui Chan,Jonathan Ip,Jian-Piao Cai,Vincent Chi-Chung Cheng,Honglin Chen,Christopher Kim-Ming Hui,Kwok-Yung Yuen (2020). A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster.
Y Liu,A Gayle,A Wilder-Smith,J Rocklöv (2020). The reproductive number of Covid-19 is higher compared to SARS coronavirus.
J Gehanno,V Bonneterre,P Andujar,J Pairon,C Paris,A Petit,C Verdun-Esquer,Q Durand-Moreau,P Brochard (2020). Arguments pour une possible transmission par voie aérienne du SARS-CoV-2 dans la crise COVID-19.
Who (2023). Covid-19 Weekly Epidemiological.
Lori Post,Salem Argaw,Cameron Jones,Charles Moss,Danielle Resnick,Lauren Singh,Robert Murphy,Chad Achenbach,Janine White,Tariq Issa,Michael Boctor,James Oehmke (2020). A SARS-CoV-2 Surveillance System in Sub-Saharan Africa: Modeling Study for Persistence and Transmission to Inform Policy.
Jenny Garcia,Catalina Torres,Magali Barbieri,Carlo-Giovanni Camarda,Emmanuelle Cambois,Arianna Caporali,France Meslé,Svitlana Poniakina,Jean-Marie Robine,Karine Guerrouche (2021). Différences de mortalité par Covid-19 : conséquence des imperfections et de la diversité des systèmes de collecte des données.
Musa Sono-Setati,Peter Mphekgwana,Linneth Mabila,Masenyani Mbombi,Livhuwani Muthelo,Sogo Matlala,Takalani Tshitangano,Naledzani Ramalivhana (2022). Health System- and Patient-Related Factors Associated with COVID-19 Mortality among Hospitalized Patients in Limpopo Province of South Africa’s Public Hospitals.
Joseph Donamou,Abdoulaye Touré,Amadou Camara,Djiki Camara,M'mah Camara,Abdourhamane Traoré,Mariame Camara,Almamy Bangoura,Boubacar Dramé,Luc Sossa,Jean-Marc Roméo Abékan,Axel Edemessi,Sow Saliou (2021). Predictive factors of mortality in patients with covid-19 in Guinea: analysis of the first 140 cases admitted to intensive care unit.
(2020). Plan national de préparation et de riposte à l'infection éventuelle par le nouveau coronavirus Covid-19.
(2021). République de la Guinée | Plan de réponse (janvier–décembre 2021).
J Hardy,P Flori (2021). Specific epidemiological features of Covid-19 in Africa: a current or future public health concern?.
M Jaspard,M Saliou Sow,S Juchet,E Dienderé,B Serra,R Kojan,A Poda,S Keita,X Anglaret,D Malvy (2021). Présentation clinique, survie et facteurs associés à la mortalité: une étude prospective dans trois centres COVID-19 en Afrique de l’Ouest.
Waasila Jassat,Cheryl Cohen,Stefano Tempia,Maureen Masha,Susan Goldstein,Tendesayi Kufa-Chakezha,Pelagia Murangandi,Dana Savulescu,Sibongile Walaza,Jamy-Lee Bam,Mary-Ann Davies,Hans Prozesky,Jonathan Naude,Trevor Mnguni,Charlene Lawrence,Hlengani Mathema,Jarrod Zamparini,John Black,Ruchika Mehta,Arifa Parker,Perpetual Chikobvu,Halima Dawood,Ntshengedzeni Muvhango,Riaan Strydom,Tsholofelo Adelekan,Bhekizizwe Mdlovu,Nirvasha Moodley,Eunice Nemavhandu,Paul Rheeder,Jacqueline Venturas,Nombulelo Magula,Lucille Blumberg (2021). A national cohort study of COVID-19 in-hospital mortality in South Africa: the intersection of communicable and non-communicable chronic diseases in a high HIV prevalence setting.
O Koné,A Kassogué,A Tembely,B Coulibaly,Hjg Berthé,O Dembélé,M Diakité (2021). Granulome inguinal inflammatoire sur hydrocèle bilatérale : une association inhabituelle.
U Kombila,C Manomba Boulingui,M Igala,J Ngomas,E Ayo Bivigou,A Ifoudji Makao,R Massolo,P Kouna,M Bouyou Akote,J Boguikouma (2022). Évolution clinique et facteurs pronostiques de décès des patients infectés par le SARS-CoV-2, hospitalisés en secteur d’infectiologie COVID du centre hospitalier et universitaire (CHU) de Libreville, Gabon.
Chaomin Wu,Xiaoyan Chen,Yanping Cai,Jia’an Xia,Xing Zhou,Sha Xu,Hanping Huang,Li Zhang,Xia Zhou,Chunling Du,Yuye Zhang,Juan Song,Sijiao Wang,Yencheng Chao,Zeyong Yang,Jie Xu,Xin Zhou,Dechang Chen,Weining Xiong,Lei Xu,Feng Zhou,Jinjun Jiang,Chunxue Bai,Junhua Zheng,Yuanlin Song (2020). Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China.
Who (2020). Covid-19 has serious repercussions on health services treating non-communicable diseases.
Mendimi Nkodo,J,Ngah Komo,M Ngo Pambe,C,Poka Mayap,V (2023). Morbidity and Pulmonary Histomorphology of Covid-19 Patients in Yaoundé.
Jacques Tamuzi,Birhanu Ayele,Constance Shumba,Olatunji Adetokunboh,Jeannine Uwimana-Nicol,Zelalem Haile,Joseph Inugu,Peter Nyasulu (2020). Implications of COVID-19 in high burden countries for HIV/TB: A systematic review of evidence.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Jean Konan Kouame. 2026. \u201cFactors Associated with Mortality in Covid-19 Patients Hospitalized in Conakrys CT-Epi, from 2020 to 2022\u201d. Global Journal of Medical Research - K: Interdisciplinary GJMR-K Volume 24 (GJMR Volume 24 Issue K1): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.