## I. BACKGROUND
 Author $\alpha$ p: University Clinical Center of Republic of Srpska, Banja Luka, Bosnia and Herzegovina Faculty of Medicine, University of Banja Luka, Banja Luka, Bosnia and Herzegovina. e-mails:
[email protected],
[email protected], (
[email protected]) Author $\sigma$: General Hospital Gradiska, Gradiska, Bosnia and Herzegovina. Faculty of Medicine, University of Banja Luka, Banja Luka, Bosnia and Herzegovina. e-mail:
[email protected]
Brain injuries are a leading cause of death and disability, particularly among young people, in both developed and developing countries. Approximately 1.19 million people die each year as a result of road traffic crashes. It's disheartening to know that road traffic injuries are the leading cause of death among children and young adults aged 5 to 29 years old. What's even more surprising is that low- and middle-income countries account for $92\%$ of the world's fatalities on the roads despite having only $60\%$ of the world's vehicles. It's important to note that pedestrians, cyclists, and motorcyclists are the most vulnerable road users and account for over half of all road traffic deaths. Additionally, road traffic crashes cost countries $3\%$ of their gross domestic product worldwide. That's why the United Nations General Assembly has set an ambitious goal of reducing the number of deaths and injuries from road traffic crashes by $50\%$ globally by 2030[1]. Traumatic brain injuries are typically categorised using scoring systems derived from clinical examinations of the patient (e.g. Glasgow coma scale) or radiological diagnostics (e.g. Rotterdam score). The goal of treating patients with severe neurotrauma in intensive care units is to prevent any secondary brain injuries while continuously monitoring vital functions. The choice of sedatives administered to reduce increased cerebral metabolic demands stemming from the injury is dependent on the experience of the physician and the adopted ICU treatment protocol for neurotrauma. The primary aim is to assess the safety of barbiturate coma use in TBI patients without invasive intracranial pressure monitoring. The secondary objective is to investigate the etiological factors and health outcomes and describe the characteristics of the population with traumatic brain injury.
## II. METHODS
A retrospective observational study was conducted on patients with severe traumatic brain injury (TBI) at a five-year time point from 2017 to 2022. To conduct the study, the Ethics Committee of the University Clinical Center of the Republic of Srpska in Banja Luka (number: 01-19-126-2/22; date 26/04/2022) granted consent according to the Helsinki declaration for patients treated with barbiturate-induced coma due to traumatic brain injury. Patient information was obtained by reviewing printed and electronic medical records through the Clinical Information System (CIS) and the Radiological Information System (PACS).
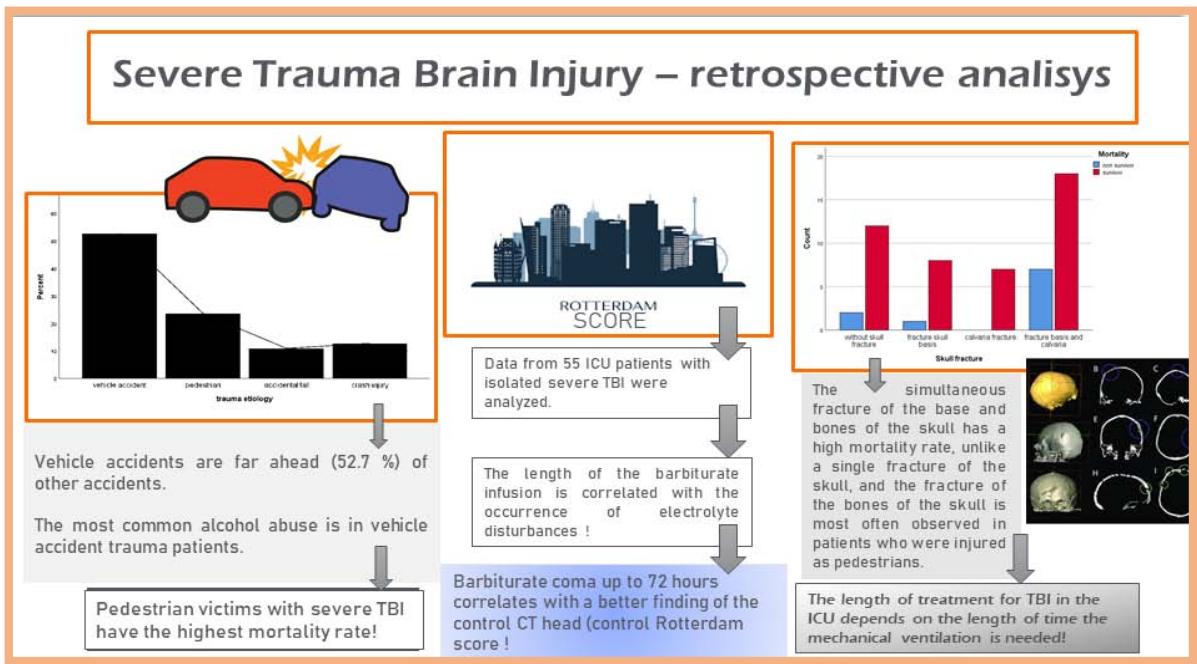
The study aimed to investigate etiological factors, health outcomes, and the effects of barbiturate infusion on neurotrauma and describe the characteristics of the TBI population. Data from 55 ICU patients with isolated severe TBI were analysed.
### a) Sampling Strategy
All patients included in the study (n 55) received clinical examination and care from an anesthesiologist and neurosurgeon, as well as laboratory and radiological assessments before being admitted to the intensive care unit.
The criteria for patient selection included a primary diagnosis of traumatic brain injury requiring continuous barbiturate infusion for deep sedation, admission to the ICU within 12 hours of the injury, availability of comprehensive clinical and laboratory records, and access to radiological CT scans before and after cessation of the barbiturate infusion.
There are several criteria for excluding patients who have sustained traumatic brain injury but do not have it as their primary injury. These factors include severe traumatic damage to other organs or organ systems, limited use of barbiturate infusion, a short duration of continuous barbiturate infusion (less than 72 hours), admission to the ICU more than 12 hours after the trauma occurred, the need for extensive transfusion, incomplete medical documentation, and an inability to obtain insight into radiological CT diagnostics.
b) The Adopted ICU Treatment Protocol for Neurotrauma
Due to the severity of the traumatic brain injuries, upon admission, we implemented a comprehensive treatment plan that included antiedematous therapy with $20\%$ mannitol at a dosage of $1\mathrm{g/kg}$. Additionally, we initiated continuous barbiturate therapy (barbiturate-induced deep sedation) at a rate of $4\mathrm{g/12h}$ for adult patients, $12.5\mathrm{mg/kg/h}$, and $3-5\mathrm{mg/kg/h}$ for pediatric patients. We continuously monitored hemodynamics invasively and non-invasive hemodynamic and respiratory parameters throughout the treatment process. A clinical neurological examination was conducted every six hours, and CT diagnostics were performed as necessary based on clinical assessments. Control CT diagnostics and suspension of the barbiturate infusion were determined by experienced anesthesiologists and neurosurgeons based on clinical and neurological stability achieved over 48 hours. Our team also evaluated the Rotterdam score, which was assessed by a radiologist who reviewed both the admission and control CT scans. Compliance with the adopted protocol for administering barbiturates is of paramount importance in the treatment of traumatic brain injuries (TBI), as the inability to measure intracranial pressure poses a significant challenge in monitoring therapy. This limitation undermines the ability to evaluate the treatment's efficacy, thus impeding optimal patient care.
To ensure stable hemodynamics and achieve the desired cerebral perfusion pressure (CPP), we maintain a sufficient mean arterial pressure (MAP) by administering vasoactive drugs and providing adequate volume replacement. It is crucial to constantly monitor the MAP by placing an arterial line. For pain management, we prescribe opioid medication, and anticonvulsive drugs are initiated once barbiturate infusion is stopped.
### c) Statistical and Data Processing
In conducting our observational studies, we followed the STROBE guidelines. We used the statistical program SPSS (IBM® Statistics, Version 20) to process our data. We reported the mean +/- standard deviation or the median (interquartile range) for continuous data. Categorical data was compared using the Chi-square test. To test the significance of individual parameters and correlations between variables, we employed T-tests and Spearman Correlation. P-values of $\leq 0.05$ were considered to be statistically significant.
## III. RESULTS
Vehicle accidents are far ahead (52,7%) of other accidents that most often lead to isolated neurotrauma, surpassing pedestrian accidents (23,6%), accidental falls (10,9%), or crash injuries (12,7%). - Figure1.
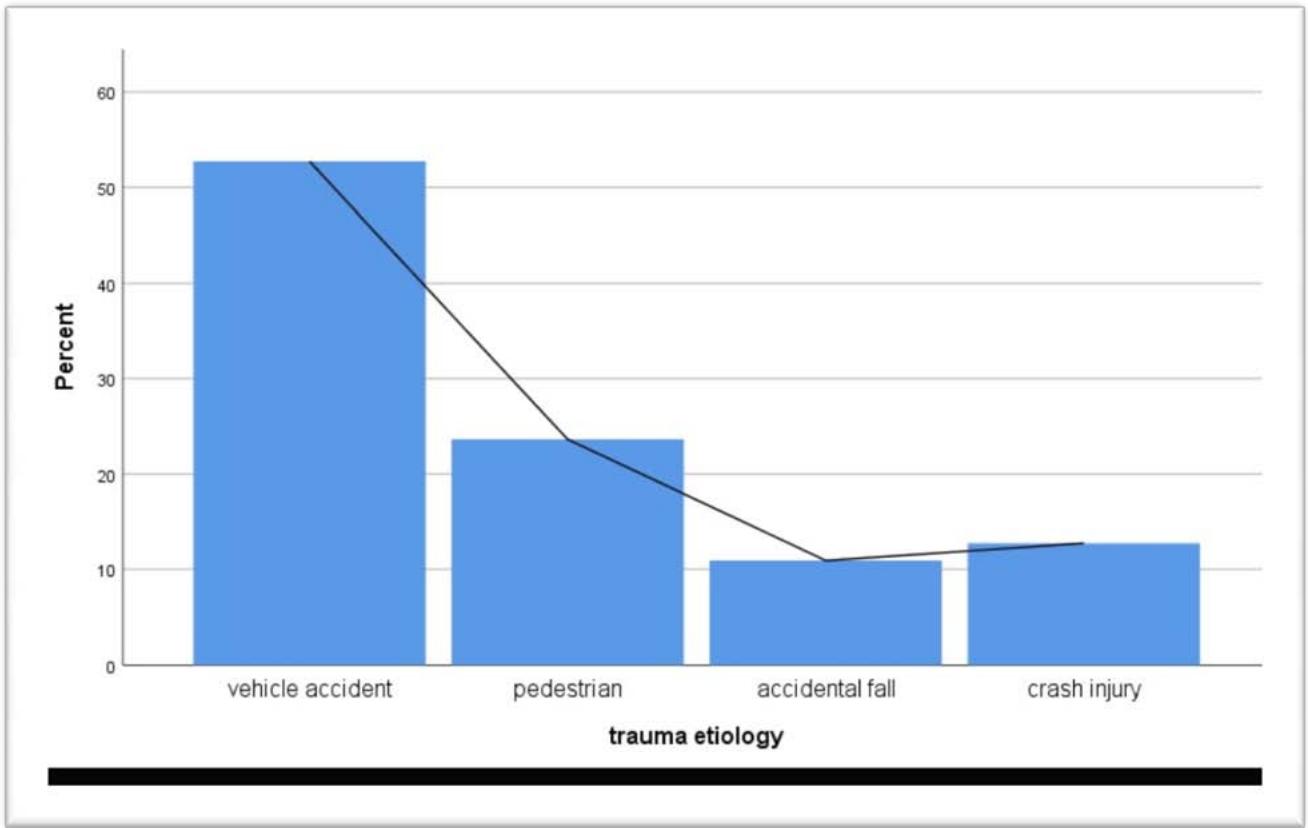 Figure 1: Bar chart of TBI aetiology by per cent of the examined patient
The demographic with the highest prevalence of severe Traumatic Brain Injury (TBI) diagnoses is individuals in their fourth decade (31-40y), followed by those in their third decade (21-30y). The average age of our patients is 39 years old, and children up to 16 years old represented $12.7\%$ of our study. Males make up the majority of TBI patients across all age groups (74,6%), except for the second decade (11 to 20 years old), where females are more commonly diagnosed.- Figure 2.
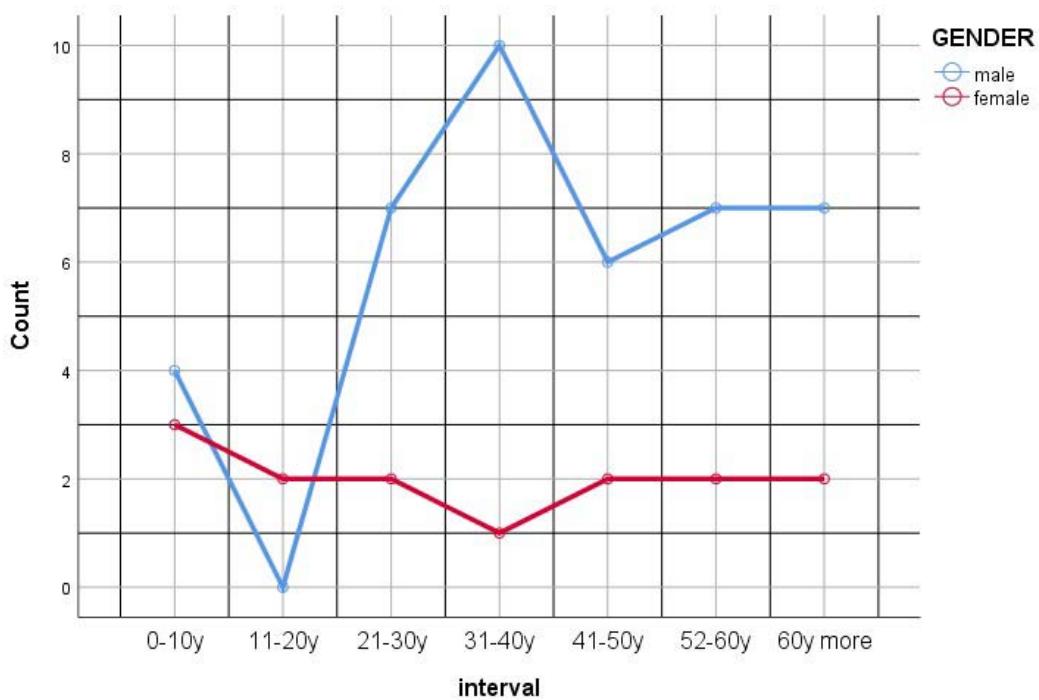 Figure 2: Gender distribution by age intervals in patients with severe TBI
After analysing the data, it was discovered that motor vehicle accidents are the leading cause of traumatic brain injuries. Thoracic trauma was found to be the most common type of injury (65%). Interestingly, cervical injuries were more significant for victims who were inside vehicles (p 0.03). On the other hand, pedestrians involved in accidents were more prone to skull bone fractures (84.6%). The study also revealed that a considerable proportion of patients admitted to the ICU due to vehicular accidents had consumed alcohol (15.8%). These findings are further supported by the data presented in Table 1.
Table 1: Categorical Data of Trauma Aetiology, Type of non-dominant injury with severe TBI patients, and mortality
<table><tr><td></td><td>Vehicle accident (%)</td><td>p*</td><td>Pedestrian (%)</td><td>p*</td><td>Crash Injury (%)</td><td>p*</td><td>Mortality (%)</td><td>p*</td></tr><tr><td>Alcohol abuse</td><td>15.8%</td><td>0.7</td><td>7.7%</td><td>0.4</td><td>11.1%</td><td>0.6</td><td>%</td><td>0.1</td></tr><tr><td>Fracture of calvaria</td><td>76.4%</td><td>0.3</td><td>84.6%</td><td>0.7</td><td>22.2%</td><td>0.6</td><td>80%</td><td>0.3</td></tr><tr><td>Cervical injury</td><td>31.6%</td><td>0.03</td><td>23.1%</td><td>0.9</td><td>0%</td><td>-</td><td>30%</td><td>0.6</td></tr><tr><td>Toracic trauma</td><td>65.8%</td><td>0.08</td><td>53.8%</td><td>0.7</td><td>66.7%</td><td>0.4</td><td>70%</td><td>0.4</td></tr><tr><td>Mortality</td><td>18.2%</td><td>0.9</td><td>38.5%</td><td>0.03</td><td>0%</td><td>-</td><td>-</td><td>-</td></tr></table>
Patients treated with barbiturate coma showed significant improvement in their computerised tomography head scan, with their Rotterdam score values shifting from the initial Rotterdam score I $(4.06\pm 0.12$; mean $\pm \mathrm{SD}$ ) to the control score values of Rotterdam score II $(3.35\pm 0.13$; mean $\pm \mathrm{SD})$ p $< 0.001$
Moreover, those who received neurosurgery within the first 24 hours, TBI patients with vasoactive support during barbiturate infusion, and surviving TBI patients displayed a significantly more favourable Rotterdam score II compared to their Rotterdam score I upon admission(p 0.001; p 0.001; p < 0.001).- Table 2.
Table 2: The initial Rotterdam score (Rotterdam score I) and the control Rotterdam score (Rotterdam score II) are based on the patient's hemodynamic stability at ICU admission, neurosurgery, vasopressors, duration of barbiturate infusion, and survival
<table><tr><td></td><td>Rotterdam scor I (mean±SD)</td><td>Rotterdam scor II (mean±SD)</td><td>p*</td></tr><tr><td>Total (mean±SD)</td><td>4.06±0.12</td><td>3.35±0.13</td><td><0.001</td></tr><tr><td>Hemodynamically stable on ICU admission (n 21, 38%)</td><td>4.1±0.8</td><td>3.4±1</td><td>0.2</td></tr><tr><td>Hemodynamically unstable on ICU admission (n 34, 62%)</td><td>4±1</td><td>3.2±0.9</td><td>0.2</td></tr><tr><td>The neurosurgical operation performed in the first 24 hours (n 16, 29%)</td><td>4.6±0.8</td><td>3.6±0.8</td><td>0.001</td></tr><tr><td>The neurosurgical operation was not performed in the first 24 hours (n 39, 71%)</td><td>3.8±0.9</td><td>3.3±1</td><td>0.02</td></tr><tr><td>There was no vasoactive support during the barbiturate coma (n 16, 29%)</td><td>4.6±0.9</td><td>4.1±1.1</td><td>0.2</td></tr><tr><td>There was vasoactive support during the barbiturate coma (n 39, 71%)</td><td>3.8±0.9</td><td>3.1±0.8</td><td>0.001</td></tr><tr><td>Surviving (n 45, 82%)</td><td>3.9±0.9</td><td>3.2±0.9</td><td><0.001</td></tr><tr><td>Deceased (n 10, 18%)</td><td>4.6±0.7</td><td>4.3±1</td><td>0.4</td></tr></table>
It has been observed that patients who have severe traumatic brain injury and are receiving barbiturate infusion may be more likely to develop hypokalemia (29 cases) compared to hypernatremia (17 cases). The extent of electrolyte imbalances seems to be directly linked to the duration of the barbiturate infusion (p=0.007 for hypokalemia; p=0.006 for hypernatremia). The duration of mechanical ventilation and barbiturate infusion are crucial factors that can affect the length of treatment in the intensive care unit (p\<0.001). However, these elements do not significantly impact the mortality rate (p=0.3; p=0.5). -Table 3.
Table 3: The impact of the duration of barbiturate infusion and mechanical ventilation on electrolyte disturbances and treatment length in the ICU for severe TBI patients
<table><tr><td></td><td>Total (media n±IQR)</td><td>Hypokalemia (n 29)</td><td>Normokalemia (n 26)</td><td>p*</td><td>Hypernatremia (n 17)</td><td>Normonatremia (n 38)</td><td>p*</td><td>ICU length p**</td><td>Mortality p**</td></tr><tr><td>Length of bar-biturate infusion by days (median±IQR)</td><td>4(6)</td><td>5(1)</td><td>3(4)</td><td>0.007</td><td>5(2)</td><td>3(2)</td><td>0.006</td><td><0.001</td><td>0.3</td></tr><tr><td>Length of mechanical ventilation by days (median±IQR)</td><td>10(36)</td><td>10(7)</td><td>10.5(11)</td><td>0.2</td><td>10(7)</td><td>10(10)</td><td>0.6</td><td><0.001</td><td>0.5</td></tr></table>
## IV. DISCUSSION
Traumatic brain injuries (TBI) are a significant public health concern as they affect a large number of people in their most productive years. The care and treatment of TBI are both long-term and costly, and the outcomes of treatment in intensive care units worldwide are uncertain and vary greatly. Often called the "silent epidemic," [2] TBI continues to be a growing public health issue, causing the highest impact on death and disability among all trauma-related injuries globally [3]. According to our study, TBI was more prevalent in men. This result is consistent with previous research on TBI by Majdan [4]. One of the reasons for this trend is that men tend to use seat belts less frequently while driving and protective equipment less often at work. Additionally, they are more likely to consume alcohol, which can increase the risk of trauma-related injuries.
The average age of our patients is 39 years old, and children up to 16 years old represented $12.7\%$ of our study. These demographic findings are similar to those of a significant epidemiological cross-sectional analysis conducted by Majdan et al. on TBI among residents of European Union countries[5]. However, the study showed substantial differences in TBI incidence rates among different EU countries, partly attributed to the varying methodologies used to process and manage medical data. The same authors also studied TBI epidemiological data in Belgium for over ten years. Their findings indicated a slight increase in the incidence of TBI among individuals over 65 years old and a significant decrease in the incidence among those under 65 years old[6].
This kind of data is an increasingly frequent finding in TBI studies, and it is impossible to explain it only by an increase in the proportion of older people in the general population [7].
Our research provides a comprehensive overview of how vehicle accidents affect individuals. It includes detailed information about the percentage of pedestrian injuries, crash injuries, and mortality rates resulting from these accidents. Additionally, it highlights the percentage of cases involving alcohol abuse, fracture of skull bones, cervical injury, thoracic trauma, and mortality rates.
The study's findings varied depending on the region and were greatly influenced by living conditions and cultural factors. It is worth noting that over the past decade, incidents of traffic-related trauma have decreased in the USA, Europe, and Japan. However, incidents of TBI caused by falls among those over 65 years have increased significantly, as reported in studies [7, 8, 9].
Providing sufficient volume replacement and administering vasoactive drugs as necessary is essential to ensure the best possible outcome. It is crucial to continuously monitor the mean arterial pressure (MAP) by inserting an arterial line. Studies have shown that hypotension is associated with a twofold rise in mortality in traumatic brain injuries compared to controls [10].
Elevated intracranial pressure (ICP) is a fatal event associated with TBI. In treating patients with TBI, basic therapeutic measures must be implemented regardless of the availability of ICP monitoring [11]. According to our research, barbiturate infusion is a viable treatment option where invasive intracranial pressure monitoring is not feasible. Our findings indicate that patients who received this treatment exhibited noteworthy enhancements in their control head CT scans. All TBI patients with severe injuries experienced a marked improvement in their control Rotterdam score values compared to their initial Rotterdam score. Patients suffering from severe traumatic brain injury and undergoing barbiturate infusion treatment may be at a higher risk of developing hypokalemia, as opposed to hypernatremia. The severity of electrolyte imbalances is proportional to the duration of barbiturate infusion. The duration of mechanical ventilation and barbiturate infusion can influence the length of treatment within the intensive care unit. However, these factors do not seem to affect the mortality rate significantly.
The study has certain limitations due to the retrospective nature of the analysis. Despite a five-year duration, it is not appropriate to conduct this research in a single centre, mainly if it is carried out in a middle-income country that lacks a national cohort of trauma patients.
## V. CONCLUSION
This study is valuable in helping to understand the nature of TBI and identify specific areas that require attention and intervention to reduce their occurrence and severity. By analysing this data, we can gain insight into the severity of trauma illnesses and develop effective therapies to improve treatment outcomes. The safety of a patient in a barbiturate coma is reflected in the absence of evidence that such treatment, without invasive monitoring of intracranial pressure, has an impact on unwanted outcomes.
The ongoing research in this area should emphasise neuroinflammation as a hidden metabolic parameter. Additionally, it should focus on developing medications such as growth factors and stem cells that promote neuronal growth and repair.