Gina Matzembacher ${}^{\text{串}}$, Nívea Maria Bordin da Silva Chacur ${}^{\S}$, Rodrigo Cadore Mafaldo ${}^{\chi}$, Leandro Dias Gomes ${}^{\nu}$, Vicenzo Stein de Vargas ${}^{\theta}$ & Gabriella Andressa Marchesin de Castro ${}^{\zeta}$
## I. INTRODUCTION
Author o: MD, PhD, DSc, Clinica Leger, Rio Grande do Sul, Brazil.
Author p Θ: MD, Clínica Leger, Rio Grande do Sul, Brazil.
Author v: MD, PhD, Clínica Leger, Rio Grande do Sul, Brazil.
Author ζ: Biomedical, PhD, DSc, Clínica Leger, Rio Grande do Sul, Brazil.
Author α Φ Ψ: MD, Clínica Leger, Rio de Janeiro, Brazil.
Gynoid lipodystrophy is a complex and multifactorial condition, and its real causes and/or predispositions are yet to be determined. Therefore, it is still difficult to achieve significant efficacy in the treatments used. $^{1,2}$
There are non-invasive treatments, such as topical therapies, oral therapies, endermology, cryolipolysis, ultrasound, infrared light, intense pulsed light, extracorporeal pulse activation therapy, and radiofrequency, used to combat cellulite. Moreover, minimally invasive treatments such as carboxytherapy, mesotherapy, subcision, and Goldincision®2,3,9,10 can also be used to this end.
### a) Goldincision®
Goldincision® is a technique developed for the treatment of more advanced grades of cellulite, according to the classification of Nürenberger and Müller. It combines subcision with biostimulation of neocollagenesis using particulate products: polylactic acid, calcium hydroxyapatite, polycaprolactone and, mainly, polymethylmethacrylate to obtain a more satisfactory result $^{11,12}$.
Polymethylmethacrylate (PMMA) is a polymer used as a tissue filler in the form of synthetic microspheres with diameters between 40 and $60~\mu \mathrm{m}$. These microspheres may be suspended in a solution of collagen, be it protic or crystalloid, which is injected with microcannulas without cuts or surgeries. Currently, with the fourth generation of PMMA, a perfect granulometry can be observed. Due to its lack of impurities and regular surface, it provides a greater area of contact with the tissue and, consequently, faster tissue fixation[13].
The commercial product may vary between $2\%$, $5\%$, $10\%$, $15\%$, and $30\%$ depending on the concentration of PMMA. It has a permanent effect, as only the vehicle is absorbed, and tissue biostimulation occurs around the particles. Considering its property of stimulating neocollagenesis through a controlled inflammatory response $^{13,14}$, PMMA can also be used as a biostimulator when in small amounts and evenly distributed in the subdermal plane at a concentration of $10\%$.
Subcision is the undermining of fibrous septa in selected areas. This technique, despite apparent clinical improvement in some cases, leaves something to be desired. There may be cases of new adhesion of the same treated septum, ineffectiveness, and frequent complications such as seromas and hematomas, in addition to limited results in isolated areas without relevant neocollagenesis $^{12,15}$.
Goldincision® is used not only for sectioning fibrous septa (Figure 1) but also for general collagen biostimulation (Figure 2), improving sagging, circulation, local metabolism and lymphatic drainage (involved in cellulite genesis). Post-procedure care prevents adverse effects and scars, making Goldincision® a successful treatment which results in a high degree of satisfaction among patients and professionals $^{12}$.
Movimento paralleos à superficie da pele.
Parallel movements to the skin surface.
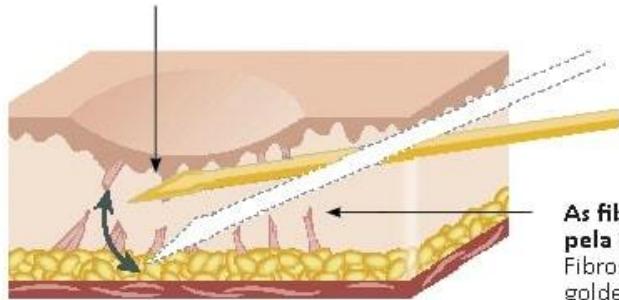
As fibroses são rompidas pelagulha de ouro.
Fibrosis are broken by the golden needle.
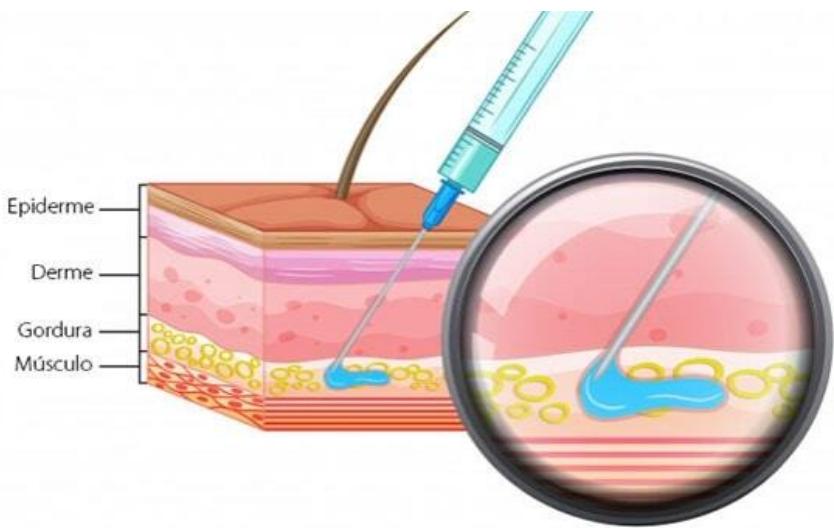 Figure 1: Sectioning of the septa with the Goldincision technique. Source: https://goldincision.com.br/tratamento-celulite-subcisao-preenchimento/ Figure 2: Application of collagen biostimulant with PMMA using the Goldincision technique. Source: https://goldincision.com.br/tratamento-celulite-subcisao-preenchimento/
## II. METHODOLOGY
This is a multicenter observational study. The case records of 47 patients who were submitted to the Goldincision® technique in 2021, using the team's protocol for evaluation, treatment, and follow-up, were evaluated. This study was approved by the Research Ethics Committee under protocol number 30867114.3.0000.5333.
Inclusion criteria were female patients with advanced grades of gynoid lipodystrophy. Exclusion criteria were patients who had hyaluronic acid, hydrogels, and biopolymers in the treated region. Pregnant patients were also excluded, along with those who were breastfeeding or had a low degree of gynoid lipodystrophy.
The evaluation criteria were the age of the patients, recommended treatment area size, number of sessions performed, volume used in each session, and adverse effects.
### a) Description of the technique
After the individual assessment of the patient by the professional, the former signed an informed consent form and had their photographic record taken. The Goldincision® procedure may be summarized as follows
- A – Preparation for the procedure;
- B - Marking of skin depressions;
- C - Asepsis;
- D - Local anesthesia;
- E - Biostimulation of neocollagenesis;
- F - Sectioning of the fibrous septa;
- G - Compressive dressings.
A. Preparation of the room and opening of sterile supplies for the procedure.
- Sterile field, gloves, and gauze are used to prepare the materials. For the procedure, an 18G malleable cannula with a blunt, atraumatic tip, an 18G needle, $2\%$ lidocaine, sterile saline for the dilution of the anesthetic, anesthesia syringe, and biostimulator are used. B. Marking of the skin depressions.
- The depressions are marked immediately before the procedure with the patient standing in a relaxed position.
- With the patient in an upright position, the septa are marked for further sectioning. C. Local disinfection.
- With the patient in the prone position, skin disinfection of the site is performed before the procedure. D. Local anesthesia is performed by cutaneous infiltration of lidocaine.
After disinfection of the area, local anesthesia is performed using $2\%$ lidocaine with vasoconstrictor diluted in sterile saline (1:1). An 18G needle is used to open the entry point for an 18G malleable cannula with a blunt, atraumatic tip. Local anesthesia infiltration is performed considering the maximum amount of anesthetic calculated by the patient's weight, generally $0.2 \mathrm{~mL}$ of lidocaine per kg or $0.4 \mathrm{~mL}$ of solution per kg.
### E. Biostimulation of neocollagenesis.
After local anesthesia, the biostimulation of neocollagenesis with $15\%$ PMMA is carried out, helping to stimulate the production of neocollagen and the improvement of local circulation. The objective of this step is to improve the overall quality of the skin, improve vascularization, collagen and metabolism in the entire region.
This step is performed with the patient in the prone position using an 18G malleable cannula with a blunt, atraumatic tip. The biostimulator is injected in a retrograde, fan-like fashion to homogeneously distribute the particulate product into the subcutaneous tissue throughout the region and not only in the depressions, and before fibrous septum detachment. Thus, it is possible to avoid the accumulation of product and the formation of nodules.
# F. Sectioning of the
After the biostimulation of the region, the sectioning of the subcutaneous septa is done using an 18G needle. For a clear view of the sectioning, it should be performed with the patient standing, so that skin undermining is kept to a minimum, just enough to even out apparent irregularities. During the procedure, some blood vessels close to the septa might be cut, resulting in the formation of transient ecchymoses with a risk of hematoma and seroma. These may be avoided with local compression during the first 24 hours. The presence of one or more surgical assistants throughout the procedure is important to maintain immediate compression of the septa after skin undermining.
# G. Compression
A compression dressing is applied to the undermined area (figure 3). The patient is instructed to keep it for 24 hours before removal. A compression garment is also worn right after the procedure. The patient must continue wearing it for at least seven days.
 Figure 3: Compression dressing on the undermined areas and compression garment. Source: Own figure.
After the procedure, the patient is instructed to wear the compressive shorts for at least seven days and not to do any physical activity until the dressings are removed (24 hours), as well as being encouraged to perform local lymphatic drainage.
 Figure 4: Ecchymosis after 7 days of Goldincision treatment. Source: Own figure.
### b) Goldincision kit
The post-treatment guidelines were associated with the use of the post-Goldincision® kit (figure 5). It consists of the use of an antithrombotic ointment made with heparin, vitamin K1, and Methyl Nicotinate, the ingestion of arnica pellets containing CH5, Echinacea D2, and Calendula D2, and subsequent use of a depigmenting cream with tranexamic acid, thioglycolic acid, and Haloxyl. This way, it is possible to minimize the main adverse effects of the procedure.
 Figure 5: Post-Goldincision kit. Source: Own figure.
## III. RESULTS
The cases of 47 female patients who underwent the Goldincision® technique were analyzed retrospectively. The average age of the participants was 39.48 years old. The regions where the technique was applied were the buttocks (n=32; 68.08%); the buttocks and posterior thighs (n=6; 12.76%); the buttocks and posterior and lateral thighs (n=2; 4.25%); posterior thighs (n=2; 4.25%); buttocks and thighs (n=4; 8.51%); and buttocks, anterior and posterior thighs (n=1; 2.12%), as seen in Table 1.
Table 1: Region of application of the Goldincision® technique.
<table><tr><td>Region</td><td>N</td><td>%</td></tr><tr><td>Buttocks</td><td>32</td><td>68.08%</td></tr><tr><td>Buttocks and posterior thighs</td><td>6</td><td>12.76%</td></tr><tr><td>Buttocks and posterior and lateral thighs</td><td>2</td><td>4.25%</td></tr><tr><td>Posterior thighs</td><td>2</td><td>4.25%</td></tr><tr><td>Buttocks and thighs</td><td>4</td><td>8.51%</td></tr><tr><td>Buttocks and anterior and posterior thighs</td><td>1</td><td>2.12%</td></tr></table>
The application area sizes ranged from small (n=8; 17.02%) to medium (n=26; 55.31%), large (n=11; 23.40%), and extra-large (n=2; 4.25%), as shown in Table 2. There was no significant association between the size of the application area and the number of sessions needed, with 2.23 being the average number of sessions.
Table 2: Size of the area of application of the Goldincision® technique.
<table><tr><td>Size</td><td>N</td><td>%</td></tr><tr><td>Small</td><td>8</td><td>17.02%</td></tr><tr><td>Medium</td><td>26</td><td>55.31%</td></tr><tr><td>Large</td><td>11</td><td>23.40%</td></tr><tr><td>Extra large</td><td>2</td><td>4.25%</td></tr></table>
The number of sessions is related to the body's response to the applied stimulus. All the patients $(n = 47)$ were submitted to the first session (Figure 6) of the technique (subcision $= 47$, biostimulus $= 44$ ); $80.85\%$ $(n = 38)$ underwent a second session (Figure 7) (subcision $= 38$, biostimulus $= 28$ ); $38.29\%$ $(n = 18)$
underwent a third session (Figure 8) (subcision=18, biostimulation=7); and $4.2\%$ $(n = 2)$ underwent a fourth session (Figure 9) which consisted only of the subcision of some remaining septa. A fifth session was not necessary for any of the patients in the analysis group.
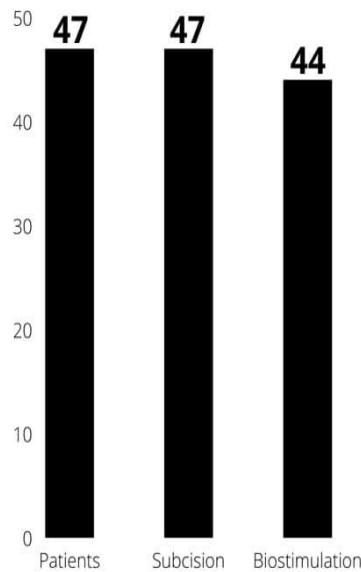 Figure 6: First session using the Goldincision® technique. Source: Own figure.
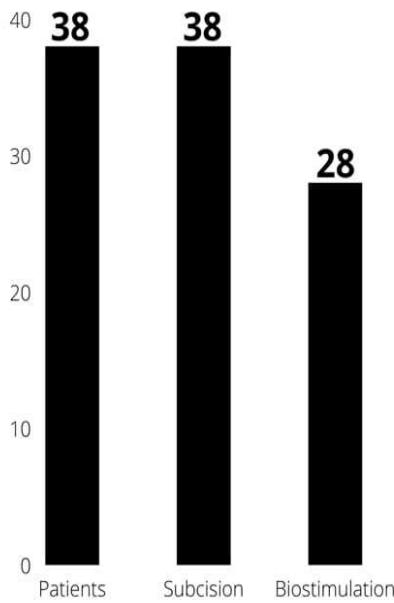 Figure 7: Second session using the Goldincision® technique. Source: Own figure.
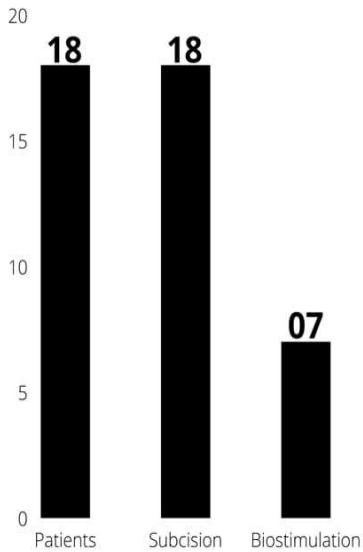 Figure 8: Third session using the Goldincision® technique. Source: Own figure.
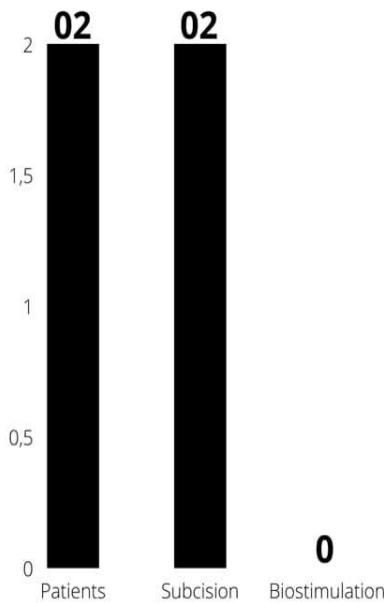 Figure 9: Fourth session using the Goldincision® technique. Source: Own figure.
The mean volume of $15\%$ polymethylmethacrylate used per session was $39.48 \mathrm{~mL}$ in the first session, $21.82 \mathrm{~mL}$ in the second session, and $12.85 \mathrm{~mL}$
in the third session. Biostimulation of neocollagenesis with the particulate product was not used in the fourth session, as shown in Table 3.
Table 3: Mean volume used per session of the Goldincision® technique.
<table><tr><td>Volume per session</td><td>N</td><td>Mean volume 10%</td></tr><tr><td>Session 1</td><td>44</td><td>39.48 mL 15%</td></tr><tr><td>Session 2</td><td>28</td><td>21.82 mL 15%</td></tr><tr><td>Session 3</td><td>7</td><td>12.85 mL 15%</td></tr><tr><td>Session 4</td><td>No biostimulation</td><td>-</td></tr></table>
As shown in Table 4, internal bleeding $(n = 47$; $100\%)$, hemosiderin staining $(n = 7$; $14.89\%)$, seroma formation $(n = 1$; $2.12\%)$, hematoma formation $(n = 1$;
2.12%), nodule formation (n=1; 2.12%), and occasional pain (n=1; 2.12%) were the complications associated with the technique.
Table 4: Complications associated with the Goldincision® technique.
<table><tr><td>Complication</td><td>N</td><td>%</td></tr><tr><td>Bleeding</td><td>47</td><td>100%</td></tr><tr><td>Hemosiderin staining</td><td>7</td><td>14.89%</td></tr><tr><td>Seroma formation</td><td>1</td><td>2.12%</td></tr><tr><td>Hematoma formation</td><td>1</td><td>2.12%</td></tr><tr><td>Nodule formation</td><td>1</td><td>2.12%</td></tr><tr><td>Occasional pain</td><td>1</td><td>2.12%</td></tr></table>
 Figure 10: Patient, 42 years old, submitted to 2 sessions of Goldincision treatment. In the first session, $39\mathrm{ml}$ of PMMA was used to biostimulate the region and the fibroussepta were sectioned. The second session was performed 42 days after the first, with only the section of the remaining septa, no product was used again. First photo taken before the procedure and the second photo taken 3 months after the second session. Source: Own figure.
 Figure 11: Patient, 43 years old, submitted to 1 session of Goldincision treatment. 45ml of PMMA was used to biostimulate the region and the fibroussepta were sectioned. First photo taken before the procedure and the second photo taken after 71 days. Source: Own figure.
## IV. DISCUSSION
Gynoid lipodystrophy presents a clinical aspect of irregular appearance of the epidermis. A fibrotic band can be seen in $97.6\%$ of the cases, especially when related to poor local circulation and metabolic insufficiency[16,17].
According to the Brazilian Society of Dermatology, gynoid lipodystrophy affects $95\%$ of women after puberty, having a significant negative impact on personal, professional, and social levels[^18].
As it is a condition with a high level of complexity, studies on the creation and improvement of treatment techniques are regularly carried out. In 1997, the subcision technique was described for the treatment of gynoid lipodystrophy grades 3 and 4 (according to the Nürenberger and Müller classification). It consists of skin undermining for the sectioning of the fibrous septa in selected areas; however, this technique alone has limited results since the production of neocollagen is not significant $^{19}$.
We do not use the term SubcisionTM because this technique has the concept of not using a product and/or association of fillers and biostimulators[^14]. The Goldincision® technique was developed to meet the needs of patients with advanced lipodystrophy. The noteworthy effects of the technique are related to its methodology, which associates stimulation of neocollagenesis with subcision, providing the undermining of fibrotic retraction but also improving the quality of the skin as a whole, improving not only the point-to-point treatment in a more effective way with the patient standing and a whole evaluation and follow-up protocol, but acting on the genesis of cellulite, resulting in an improvement of cellulite in all degrees with restructuring of collagen, a component of local metabolism, and neovascularization[^12].
## V. CONCLUSION
This study described the Goldincision® technique for the treatment of gynoid lipodystrophy. It proved to be effective and safe in improving the quality of the skin and sectioning the fibrous septa; thus, providing a homogeneous skin appearance. The treatment must be prescribed and performed by a professional who is trained to perform the technique, understands the associated adverse effects, and has the resources and scientific knowledge to deal with them, ensuring patient safety.
The positive clinical effects of Goldincision® on the treatment of gynoid lipodystrophy were evident, and its use is very promising as the main minimally invasive treatment for this condition.
### Financial Disclosure and Products Page
All authors have no commercial interests or financial relationships with any of the products, devices or drugs mentioned in this manuscript. Therefore, there is no conflict of interest with the information presented in the submitted manuscript. Own financing.
Generating HTML Viewer...
References
19 Cites in Article
Ana Mendonça,Michelle Pádua,Ana Ribeiro,Giovana Milani,Sílvia João (2009). Confiabilidade intra e interexaminadores da fotogrametria na classificação do grau de lipodistrofia ginóide em mulheres assintomáticas.
Pérez Atamoros,F,Alcalá Pérez,D Aszsigall,D,Ávila Romay,A,Barba Gastelum,J De Lapeña Salcedo,J,Escalante Salgado,P,Gallardo Palacios,G Guerrero-Gonzalez,G,Morales De La Cerda,R,Ponce Olivera,R,Rossano Soriano,F,Solís Tinoco,E,Welsh Hernández,E (2018). Evidencebased treatment for gynoid lipodystrophy: A review of the recent literature.
Paulo João,Thaís Junqueira M Afonso,Maria Cardoso De Mello Tucunduva,Bussamara Valéria,Ediléiabagatin Pinheiro (2010). Cellulite: a review.
D Hexsel,T Dal’forno,C Hexsel (2009). A validated photonumeric cellulite severity scale.
Kamila Tokarska,Sławomir Tokarski,Anna Woźniacka,Anna Sysa-Jędrzejowska,Jarosław Bogaczewicz (2018). Cellulite: a cosmetic or systemic issue? Contemporary views on the etiopathogenesis of cellulite.
F Nürnberger,G Müller (1978). So‐Called Cellulite: An Invented Disease.
F Nurnberger (1981). Practically important diseases of the subcutaneous fatty tissue (including so-called cellulite).
M De La Casa Almeida,C Suarez Serrano,J Rebollo Roldán,J Jiménez Rejano (2013). Cellulite’s aetiology: a review.
Schonvvetter Bianca,Juliana Soares,Bagatinediléia Marques (2014). Longitudinal evaluation of manual lymphatic drainage for the treatment of gynoid lipodystrophy.
Daniel Friedmann,Garrett Vick,Vineet Mishra (2017). Cellulite: a review with a focus on subcision.
David Orentreich,Norman Orentreich (1995). Subcutaneous Incisionless (Subcision) Surgery for the Correction of Depressed Scars and Wrinkles.
Roberto Chacur,Honorio Sampaio Menezes,Danuza Dias Alves,Nivea Maria Bordin,Silva Da,Renata Chacur,D'oliveira Bataiolli,Raissa Nardi (2019). Cellulite treatment using subcision and polymethyl methacrylate filling (goldincision®): case report.
Gottfried Lemperle,Vera Morhenn,Ulrich Charrier (2003). Human Histology and Persistence of Various Injectable Filler Substances for Soft Tissue Augmentation.
Roberto Chacur (2018). Ciência e Arte do Preenchimento. 1ª edição.
Dóris Hexsel,Rosemari Mazzuco (2000). Subcision: a treatment for cellulite.
Lauren Whipple,Craig Fournier,Adee Heiman,Amanda Awad,Malcolm Roth,Sebastian Cotofana,Joseph Ricci (2021). The Anatomical Basis of Cellulite Dimple Formation: An Ultrasound-Based Examination.
Enzo Emanuele,Piercarlo Minoretti,Karmela Altabas,Elio Gaeta,Velimir Altabas (2011). Adiponectin expression in subcutaneous adipose tissue is reduced in women with cellulite.
Doris Hexsel (2021). Avaliaçao do grau (evaluación del grado) de celulite em mulheres em uso de três (que utilizan tres) diferentes dietas.
Enzo Emanuele (2013). Cellulite: Advances in treatment: Facts and controversies.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Honório Sampaio Menezes. 2026. \u201cGoldincision – A Multifactor Approach To Cellulite Treatment\u201d. Global Journal of Medical Research - F: Diseases GJMR-F Volume 23 (GJMR Volume 23 Issue F9): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































