## I. INTRODUCTION
Acquired diverticulosis of the small bowel was first described by Baillie and Sommering in 1794. In 1807, Sir Astley Cooper specifically described jejunal diverticula with $75\%$ of them affecting the proximal jejunum, $20\%$ the distal jejunum and $5\%$ the ileum(4).
Diverticula of the gastrointestinal tract may occur from the upper esophagus down to the rectum. The outpouchings of the gastrointestinal tract may be true diverticula that involve all layers of the bowel wall. The most common true diverticulum is a Meckel's diverticulum present in approximately $2\%$ of the population and usually found in the ileum(5).
Complications such as perforations, adhesion, fistula, and peritonitis are more common than massive lower gastrointestinal bleeding, and these complications are reported only in $10\%$ of cases. Surgery is the definitive treatment option in case of complicated diverticulitis with perforation like in our case(1)
## II. CASE REPORT
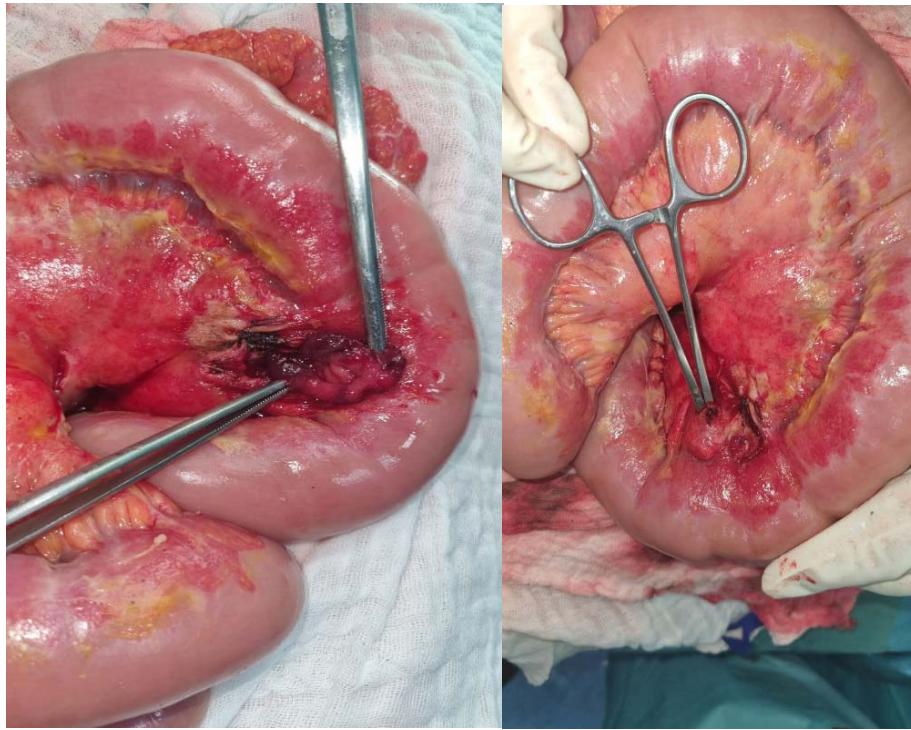
A 53-year-old patient, followed for chronic kidney disease for 7 years, hospitalized in the nephrology department for suspicion of peritonitis on a peritoneal dialysis catheter, with a clinical picture of generalized abdominal pain, nausea and vomiting, without digestive hemorrhage or transit disorder, all evolving in a context of feverish sensation. The clinical examination found a conscious patient SG=15/15, BP=11/06mmHg, FR=16cpm, FC=68bpm, T°=38,9°. The abdominal examination found a generalized abdominal tenderness, with a peritoneal dialysis catheter at the left para-umbilical level. On biological assessment WBC=23610ele/mm, CRP=149mg/L, Pro calcitonin=5ng/L. Cytobacteriological study of the peritoneal fluid was negative. The patient was initially treated with antibiotics for 6 days with no significant improvement. The biological check-up found an increase in white blood cells at 36000elem/mm, CRP=256mg/L, procalcitonin=34ng/L, and the cytobacteriological examination of the peritoneal fluid found white cells at 17920 with E. Coli as the identified germ. The indication of an exploratory laparotomy was put. Surgical exploration found a large pus effusion with several false membranes, and a perforated jejunal diverticulum 20 centimeters from the duodeno-jejunal angle opposing the mesenteric border (fig. 1). The procedure consisted of a resection of the diverticulum with terminal anastomosis. The postoperative course was simple and without complications.
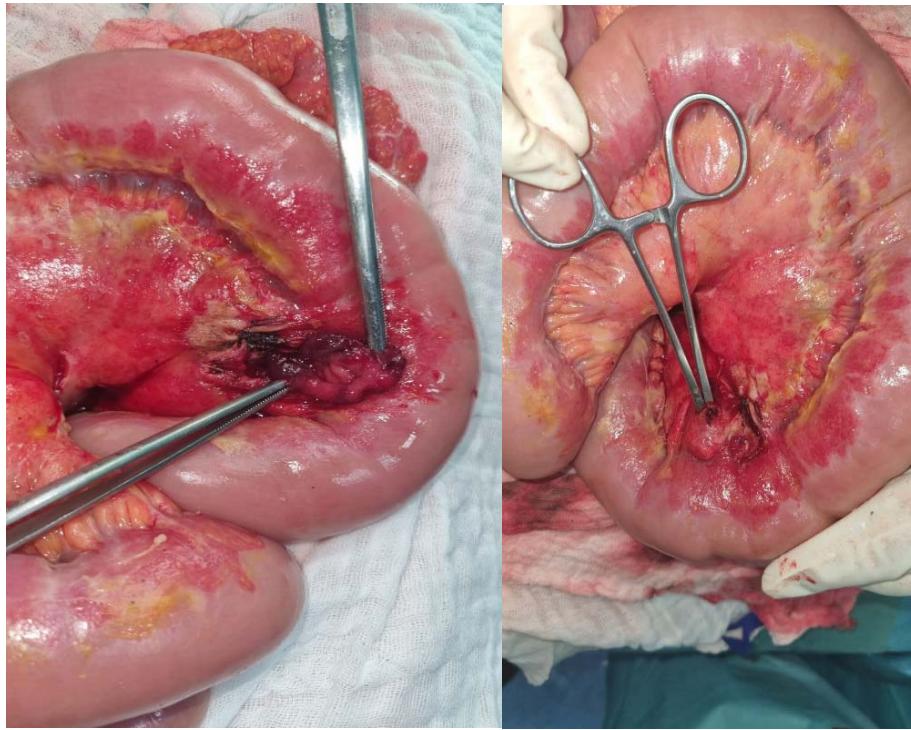 Fig. 1: Intra-operative view showing the perforated jejunal diverticulum
## III. DISCUSSION
The increased incidence of diverticula in the proximal jejunum compared to the distal jejunum and the ileum is attributed to the larger diameter of blood vessels in the proximal jejunum, vasa recta, or anastomosis arches between the jejunal arteries and ileal, originating from the superior mesenteric artery(6).
Small bowel diverticula can be either congenital or acquired. Congenital diverticula are located on the antimesenteric border of the small bowel. It contains all the layers of the bowel including mucosa, submucosa, muscularis, and serosa. When present, they are usually solitary and Meckel's diverticulum is considered the most common example(2). Acquired diverticula are formed by a herniation of the mucosa and submucosa through the muscular layer of the bowel wall, while false diverticula probably due to motor dysfunction of the smooth muscle or the myenteric plexus of the small intestine, generating an increase in intraluminal pressures such as progressive systemic sclerosis, visceral neuropathies and myopath(1,6).
Jejunal diverticulosis is usually asymptomatic. Only $29\%$ of patients develop symptoms and $10\%$ develop complications such as perforation, obstruction, adhesion, fistula, peritonitis, and lower gastrointestinal bleeding(nigam). Perforation of jejunal diverticula is a severe complication that occurs in 2 to $6\%$ of cases(1).
The risk factors for jejunal diverticula perforation include blunt abdominal trauma leading to a necrotizing inflammatory reaction in $82\%$ of cases, foreign body impaction in $6\%$ of cases(7), cocaine sniffing, NSAID usage (as noted in our case), amyloid disease and malignancy like lymphosarcoma, MEN1, and fibrous histiocytoma, and Ehler-Danlos syndrome (2).
Symptomatic cases present with early satiety, bloating, anorexia, diarrhea/steatorrhea due to bacterial overgrowth, colicky pains in epigastrium, peri-umbilical region, loud rumbling noises in the abdomen following meals(8).
Small bowel diverticulosis is often diagnosed incidentally in patients undergoing upper endoscopy or imaging for upper gastrointestinal symptoms. Plain film radiographs of the abdomen will suggest the diagnosis from the presence of air-fluid levels in multiple diverticula throughout the small intestine(1).
Contrast studies, including enteroclysis of the jejunum and ileum, will reveal a large outpouching with retained contrast medium after the main lumen has become empty. The lumen of the intestine will be dilated in the diverticula, and the mucosal folds will be thickened and prominent(9).
The CT scan has the diagnostic value higher to identify the presence, site and cause intestinal perforation(8). It can allow the diagnosis of diverticular perforation of the jejunum, based on the following images: free intraperitoneal air, extraluminal air bubbles concentrated near the intestinal wall, asymmetric thickening of the wall, edema or thickening of surrounding fatty tissue. However, an accurate diagnosis is rarely made before laparotomy or exploratory laparoscopy(10) For stable patients with contained perforations, non-operative treatment such as bowel rest, intravenous fluids and antibiotics, has been successfully reported(11). For larger peridiverticular abscesses, CT-
guided percutaneous drainagemay be required. In the case of failure of non-operative management and in patients with generalized peritonitis surgery is mandatory(12).
## IV. CONCLUSION
Acquired jejunal diverticulosis is a rare disorder of the small intestine. Perforation of a jejunal diverticulum have a high morbidity and mortality rates.
The treatment of diverticular perforation associated with peritonitis, is the resection of the segment of the small intestine involved with anastomosis.
Conservative treatment is possible in some mild cases and presents an alternative for surgery.
Rohik Anjum,Navin Kumar,Tanuj Singla,Rishit Mani,Bibek Karki (2021). A Case of Isolated Jejunal Diverticulum Presented as Free Perforation: A Rare Cause of Acute Abdomen.
Aradhya Nigam,Faye Gao,Mark Steves,Paul Sugarbaker (2020). Acute abdomen caused by a large solitary jejunal diverticulum that induced a midgut volvulus. Report of a case.
Tagleb Mazahreh,Abdelwahab Aleshawi,Mohammed Alorjani,Rasheed Elayyan,Nabil Al-Zoubi (2019). Arteriovenous malformations within jejunal diverticulosis: case report and literature review.
H Prough,S Jaffe,B Jones (2019). Jejunal diverticulitis.
M Kuzmova,M Salame,P Colonval Diverticule jéjunal perforé et abcédé : revue de la littérature.
Yeqian Huang,Mina Sarofim,Ruben Cohen‐hallaleh (2021). Foreign body perforation of a jejunal diverticulum: a rare cause of rectal bleeding.
Prajjwol Luitel,Bibek Shrestha,Shankar Adhikari,Bishnu Kandel,Paleswan Lakhey (2021). Incidental finding of jejunal diverticula during laparotomy for suspected adhesive small bowel obstruction.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
El Hattabi Khalid. 2026. \u201cIncidental Finding of Perforated Jejunal Diverticulum during Laparotomy for Suspected Peritonitis on Peritoneal Dialysis Catheter: A Case Report\u201d. Unknown Journal GJMR-I Volume 23 (GJMR Volume 23 Issue I1): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.