## I. INTRODUCTION
Hypertension (AH) is directly related to the development of cardiovascular diseases, accounting for $40\%$ of deaths from stroke, $25\%$ of deaths from coronary artery disease, and, in combination with diabetes mellitus (DM), $50\%$ of cases of end-stage chronic kidney disease (1). It is a chronic non-transmissible condition characterized by persistent elevation of blood pressure (BP) (2). In Brazil, it is estimated that $35\%$ of the adult population is hypertensive, according to data from the Ministry of Health (MS). Around $50\%$ of the remaining persons do not know they have the disease. Considering only those over 60, this percentage is around $65\%$ of the hypertensive people in the country.
In most cases is asymptomatic, implying the difficulty of early diagnosis and without adherence to the treatment recommended, whether pharmacological or not. For this reason, AH control is still so low, making it a challenge for health services. Associated with the main risk factors such as age, gender and ethnicity, obesity and dyslipidemia, sedentary lifestyle, salt and alcohol intake, and socioeconomic and genetic factors, AH contributes to the worsening of the patient's cardiovascular morbidity and mortality.
Since 2005, ischemic heart disease and cardiovascular disease have been Brazil's leading causes of death. Up to 2015, there was an increase of $18.8\%$ in deaths by the first cause and $13.3\%$ from the second cause. During this period, ischemic heart disease moved from the second to the first cause of premature deaths (below 60 years), with an increase of $8.5\%$ (3).
Among these risk factors related to hypertension, some can still promote inflammation, such as dyslipidemia and obesity. The fat tissue is a dynamic organ, the leading storage for primary, excess energy, has an endocrine function, and synthesizes a series of biologically active compounds that regulate metabolic homeostasis (4).
The inflammatory profile in obese individuals is called metabolic or meta-inflammation $^{(5)}$. This whole process alters the adipose tissue's functioning, thus characterizing a dysfunctional tissue. Among the characteristics of this dysfunction, the fat mass will present changes in its cellular composition, such as, for example, an increase in the number of inflammatory cells $^{(4)}$. It produces a series of substances, such as macrophages, which, in turn, infiltrate the adipose tissue during the advanced stages of obesity and participate in the inflammatory event by producing more cytokines, such as interleukin-6 (IL-6) $^{(6,7)}$.
Therefore, hypertension, known as a noncommunicable disease, imposes the need for the individual to adopt changes in their lifestyle, primarily related to those caused by restrictions resulting from the disease, therapeutic conditions, and clinical controls, as well as the possibility of recurrent hospitalizations (8).
Considering that hypertension is a severe public health problem, the importance of this study for health surveillance is highlighted to understand how it can alter the population's quality of life and morbidity and mortality profile.
The objective of this study is to observe the risk factors that a hypertensive population presents in the outpatient segment from the nurse's perspective of care.
## II. METHOD
### a) Design
This is a cross-sectional, analytical study with a quantitative, population-based approach.
The study was conducted in a primary health unit in the municipality of Barreiras in the state of Bahia, in the northeast region of Brazil. The unit is a reference in its area for the diagnosis, treatment, and follow-up of patients with hypertension. The sample was determined based on the patients linked to this health unit using the simple random sampling method. All patients in the hypertensive follow-up program were considered for the study. As the number of hypertensive patients (n) monitored by the health unit was known (70 patients), all were invited to participate in the study. To calculate the sample size a confidence level (z) of $95\%$ was used, a standard deviation (p) of 0.5, and a margin of error (e) of $+/- 5\%$, being estimated 60 participants. Size = $[z^2 x p(1-p)] / e^2 / 1 + [z^2 x p(1-p)] / e^2 x n$
The inclusion period comprised October 2019 to May 2020, and there was no impact or risk to participants due to the COVID-19 pandemic.
Individuals over 18 and hypertensive patients enrolled in the health unit were included after their written consent. Patients with cancer undergoing treatment in the last five years, the presence of viral hepatitis or HIV infections, rheumatologic diseases such as lupus and rheumatoid arthritis, pregnant women, and chronic users of steroids were not considered for the study.
The demographic information of each patient and the risk factors for a cardiovascular disease they presented were collected. These factors were the presence of dyslipidemia, diabetes, smoking, obesity, sedentary lifestyle, and occurrence of coronary artery disease.
A blood pressure measurement for staging their disease was performed according to the Brazilian Hypertension guideline (2).
The laboratory variables evaluated to determine renal function were serum creatinine, assessed by the modified Jaffe reaction. The estimative of the glomerular filtration rate (eGFR) was performed by the CKD-EPI equation $^{(9,14)}$.
The identification of chronic kidney disease (CKD) was defined as the eGFR of less than 90 ml/min/1.73m2, according to KDIGO (10).
The Framingham scale was used to measure the cardiovascular risk of each patient (11-13).
Each patient's inflammatory status was assessed by measuring ultra-sensitive C-reactive protein (CRP), interleukin-6 (IL-6), serum ferritin, and serum 25-OH-vitamin D. These parameters were measured by electrochemiluminescence.
### b) Statistical Analysis
For the statistical analysis, the SPSS v21.0 software was used. The Kolmogorov-Smirnov test was used to verify the uniformity of the data.
Non-parametric tests were used to allow the analysis of variables with different distributions.
Statistical analyses were sequentially adjusted for the following confounding factors: 1) mean and standard deviation for quantitative variables; 2) percentage for qualitative variables, except for variables describing inflammatory markers, which were described as mean, standard deviation, median, 25th and 75th percentiles, minimum and maximum.
Spearman's correlation analyzed the relationships between quantitative variables, and the chi-square test was used for qualitative variables. A significance level of 0.05 (5%) was defined for this study. A logistic regression model was constructed to evaluate the predictive variables for hypertension and high cardiovascular (CV) risk development.
Regardless of their significance, all quantifiable and non-quantifiable variables were used in the statistical analysis of the studied sample.
The study followed the STROBE systematization for cross-sectional studies.
The study was approved under number 3.286.842, issued by the local ethics committee.
## III. RESULTS
Table 1 presents the descriptive data of the characteristics of the sample. Seventy participants were invited to participate in the study, of which 61 answered the call, and all 61 individuals met the inclusion criteria. Thus every participant was included, and no data was lost.
The participants involved in this research had a mean age of $58 \pm 11$ years, $56\%$ female.
Table 1: Demographic characterization of the sample and cardiovascular risk factors in Barreiras, Bahia, Brazil, 2020
<table><tr><td colspan="2">Variables</td><td>Participants (n=61)</td></tr><tr><td colspan="2">Age years)</td><td>58±11</td></tr><tr><td colspan="2">Weight (Kg)</td><td>71.7±13.1</td></tr><tr><td colspan="2">Height (m)</td><td>1.6±0.1</td></tr><tr><td colspan="2">Waist circumference (cm)</td><td>95.3±9.4</td></tr><tr><td colspan="2">BMI (Kg/m2)</td><td>27±5</td></tr><tr><td>Sex</td><td></td><td></td></tr><tr><td></td><td>Male</td><td>27 (44.3%)</td></tr><tr><td></td><td>Female</td><td>34 (55.7%)</td></tr><tr><td>Ethnicity</td><td></td><td></td></tr><tr><td></td><td>Caucasian</td><td>6 (9.8%)</td></tr><tr><td></td><td>Black</td><td>55 (90.2%)</td></tr><tr><td>Education</td><td></td><td></td></tr><tr><td></td><td>None</td><td>8 (13.1%)</td></tr><tr><td></td><td>Literate</td><td>4 (6.6%)</td></tr><tr><td></td><td>incomplete 1st grade</td><td>20 (32.8%)</td></tr><tr><td></td><td>complete 1st degree</td><td>10 (16.4%)</td></tr><tr><td></td><td>incomplete high school</td><td>3 (4.9%)</td></tr><tr><td></td><td>complete high school</td><td>9 (14.8%)</td></tr><tr><td></td><td>Incomplete higher</td><td>3 (4.9%)</td></tr><tr><td></td><td>Graduated</td><td>4 (6.6%)</td></tr><tr><td>Consumption of alcohol</td><td></td><td></td></tr><tr><td></td><td>Yes</td><td>12 (19.7%)</td></tr><tr><td></td><td>No</td><td>49 (80.3%)</td></tr><tr><td>Hypertensive therapy</td><td></td><td></td></tr><tr><td></td><td>None</td><td>2 (3.3%)</td></tr><tr><td></td><td>Use one medication</td><td>19 (31.1%)</td></tr><tr><td></td><td>Use two medications</td><td>20 (32.8%)</td></tr><tr><td></td><td>Use three medications</td><td>11 (18%)</td></tr><tr><td></td><td>Use more than three medications</td><td>9 (14.8%)</td></tr><tr><td>Use of drugs</td><td></td><td></td></tr><tr><td></td><td>Yes</td><td>1 (1.6%)</td></tr><tr><td></td><td>No</td><td>60 (98.4%)</td></tr><tr><td>Chronic kidney disease</td><td></td><td></td></tr><tr><td></td><td>Yes</td><td>4 (6.6%)</td></tr><tr><td></td><td>No</td><td>57 (93.4%)</td></tr></table>
The characterization of inflammatory markers was described in Table 2 in detail to allow identification of the sample amplitude, as shown in Figure 1.
Table 2: Characterization of the laboratory parameters of the population studied in Barreiras, Bahia, Brazil, 2020
<table><tr><td rowspan="2"></td><td rowspan="2">Mean±SD</td><td rowspan="2">Median</td><td colspan="2">Percentiles</td><td rowspan="2">Minimum</td><td rowspan="2">Maximum</td></tr><tr><td>25</td><td>75</td></tr><tr><td>Hemoglobin (g/dL)</td><td>14.17 ± 1.69</td><td>14</td><td>12.70</td><td>15.25</td><td>11.10</td><td>18.80</td></tr><tr><td>Hematocrit (%)</td><td>42.63 ± 4.63</td><td>41.90</td><td>39.40</td><td>45.30</td><td>32.90</td><td>52.60</td></tr><tr><td>Creatinine (mg/dL)</td><td>0.91 ± 0.25</td><td>0.89</td><td>0.73</td><td>1.08</td><td>0.42</td><td>1.44</td></tr><tr><td>Urea (mg/dL)</td><td>29.3 ± 7.65</td><td>29.00</td><td>23</td><td>34</td><td>14</td><td>51</td></tr><tr><td>Neutrophil/Lymphocyte Ratio</td><td>1.67 ± 0.65</td><td>1.60</td><td>1.18</td><td>2.07</td><td>0.38</td><td>3.13</td></tr><tr><td>IL-6 (pg/mL)</td><td>2.61 ± 1.17</td><td>2.24</td><td>1.53</td><td>3.56</td><td>1.35</td><td>6.10</td></tr><tr><td>Ferritin (ng/mL)</td><td>173.11 ± 99.92</td><td>154</td><td>99.65</td><td>207</td><td>27.40</td><td>400</td></tr><tr><td>D Vitamin (ng/mL)</td><td>26.18 ± 6.58</td><td>25.50</td><td>21.75</td><td>29.70</td><td>13.60</td><td>42.30</td></tr><tr><td>CRP (mg/L)</td><td>0.28 ± 0.29</td><td>0.15</td><td>0.06</td><td>0.45</td><td>0.02</td><td>1.19</td></tr></table>
When cardiovascular risk (CV) was stratified, 09 patients presented a low risk, 13 patients at intermediate risk, 37 patients with high risk, and 02 patients showed a very high risk in the sample studied.
When calculating the glomerular filtration rate (GFR) in the studied sample, $55.73\%$ (34 patients) had an expected result. In contrast, the others, $44.26\%$ (27 patients), presented an altered result when comparing the parameters age, creatinine, sex, and ethnicity, by the CPK-EPI equation ${}^{(9,14)}$.
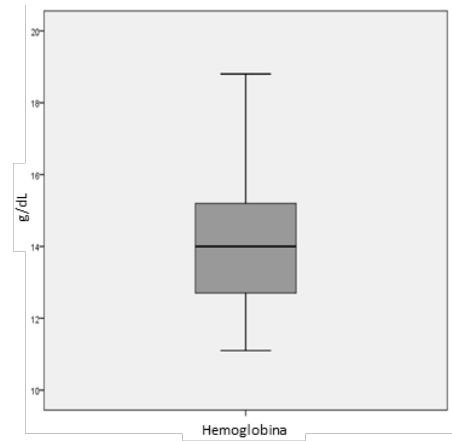
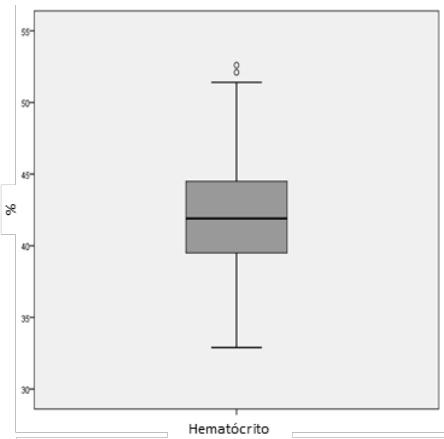
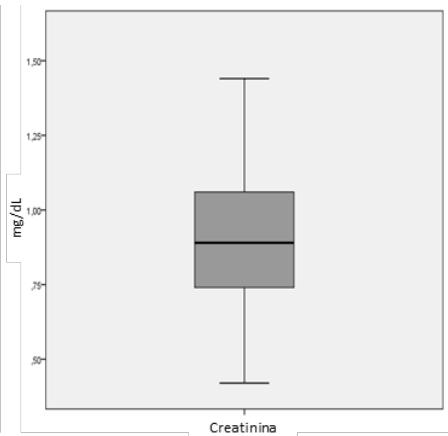
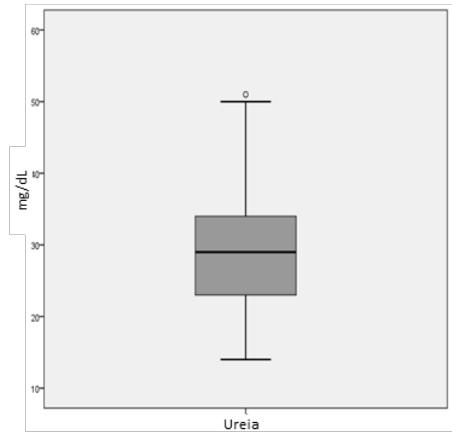

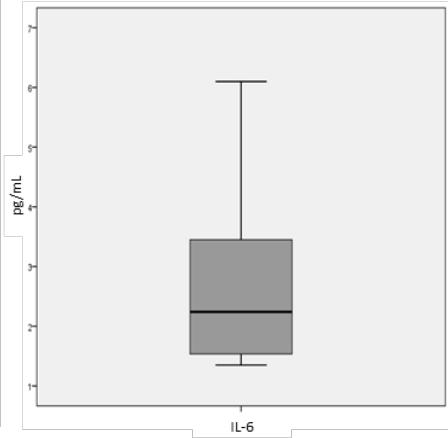
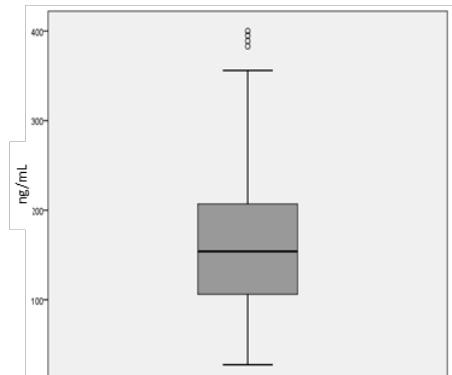
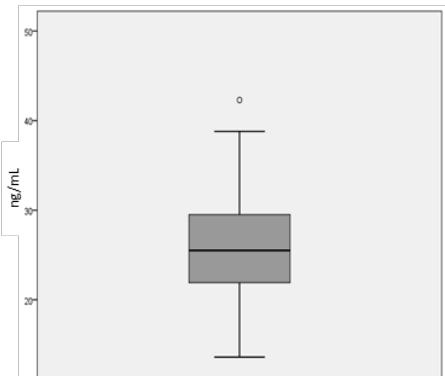
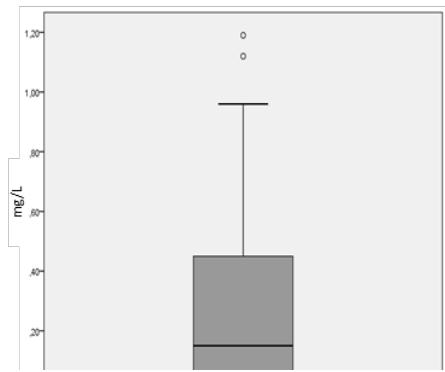 Figure 1: Box diagram for inflammatory marker variables
Grams by deciliter (g/dL); percentage (%); milligrams by deciliter (mg/dL); interleukin 6 (IL-6); picogram by milliliters (pg/mL); nanograms by milliliters (ng/mL); C reactive protein (PCR); milligrams by liter (mg/L).
Table 3 shows the variables that presented correlation when analyzed among themselves. The relationship between age and glucose was direct $(p = 0.008)$, while eGFR was inverse $(p < 0.001)$. Waist circumference is directly related to both BMI $(p < 0.001)$ and CRP $(p = 0.019)$, so BMI and CRP are also directly related $(p = 0.001)$. An inverse relationship was found between IL-6 and GFR $(p = 0.027)$, a direct relationship with CRP $(p = 0.009)$, and a direct relationship between Glucose and Ferritin $(p = 0.020)$.
Table 3: Relationship between blood variables and age with BMI and waist circumference in Barreiras, Bahia, Brazil, 2020
<table><tr><td></td><td>Glucose</td><td>BMI</td><td>GFR</td><td>IL6</td><td>CRP</td><td>Vitamin D</td></tr><tr><td>Age</td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Correlation Coefficient*</td><td>0.339</td><td>-0.246</td><td>-0.492</td><td>0.076</td><td>0.088</td><td>-0.022</td></tr><tr><td>p-value</td><td>0.008</td><td>0.056</td><td>< 0.001</td><td>0.581</td><td>0.502</td><td>0.868</td></tr><tr><td>Waist circumference</td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Correlation Coefficient*</td><td>0.044</td><td>0.752</td><td>-0.009</td><td>0.151</td><td>0.300</td><td>-0.029</td></tr><tr><td>p-value</td><td>0.738</td><td>< 0.001</td><td>0.944</td><td>0.272</td><td>0.019</td><td>0.823</td></tr><tr><td>BMI</td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Correlation Coefficient*</td><td>0.005</td><td rowspan="2">-</td><td>0.043</td><td>0.183</td><td>0.421</td><td>-0.034</td></tr><tr><td>p-value</td><td>0.972</td><td>0.744</td><td>0.181</td><td>0.001</td><td>0.793</td></tr><tr><td>IL6</td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Correlation Coefficient*</td><td>-0.181</td><td>0.183</td><td>-0.298</td><td rowspan="2">-</td><td>0.351</td><td>-0.198</td></tr><tr><td>p-value</td><td>0.191</td><td>0.181</td><td>0.027</td><td>0.009</td><td>0.148</td></tr><tr><td>Ferritin</td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Correlation Coefficient*</td><td>0.301</td><td>0.005</td><td>-0.001</td><td>-0.092</td><td>-0.096</td><td>0.191</td></tr><tr><td>p-value</td><td>0.020</td><td>0.970</td><td>0.994</td><td>0.503</td><td>0.462</td><td>0.141</td></tr></table>
Table 4: Association between blood glucose and cardiovascular risk in Barreiras, Bahia, Brazil, 2020
<table><tr><td></td><td colspan="2">Normal Glucose
Changed</td><td>p-value</td></tr><tr><td>Cardiovascular risk</td><td></td><td></td><td></td></tr><tr><td>Low</td><td>7 (77.8%)</td><td>2 (22.2%)</td><td></td></tr><tr><td>Intermediary</td><td>6 (50%)</td><td>6 (50%)</td><td>0.027*</td></tr><tr><td>High</td><td>11 (28.9%)</td><td>27 (71.1%)</td><td></td></tr><tr><td>Very high</td><td>0 (0%)</td><td>2 (100%)</td><td></td></tr></table>
## IV. DISCUSSION
This study was conducted in the municipality of Barreiras, a medium-sized city in the state of Bahia, 863 km from the capital. It has an area of $7,538\mathrm{km}^2$, with an estimated population of 153,831 inhabitants, and is considered the twelfth largest population, economic, political, and cultural center of Bahia (15).
Its population is predominantly non-white and mixed. It is the gateway to health services through primary care or the regional hospital that serves the entire western region of Bahia.
Although abdominal circumference provides independent and additive information to the body mass index (BMI), the hypertensive effect of weight gain was well recorded (2). Excessive body adiposity, especially visceral adiposity, is a significant risk factor for BP elevation, which may be responsible for 65 to $75\%$ of cases of hypertension (2).
Weight loss reduces BP, even without reaching the desired body weight. For overweight or obese individuals, weight loss is an essential recommendation in treating $\mathsf{AH}^{(2)}$. All participants had a waist circumference above $80~\mathrm{cm}$ in diameter in the sample studied. Those with higher waist circumference also had higher weight and a higher BP, thus confirming that individuals with higher weight also had more elevated BP. In addition to being overweight, the mean BMI $(27\pm 5)$ and waist circumference $(95.3\pm 9.4)$ were above the recommended, corroborating the obesity of the studied population.
However, it was impossible to establish a direct relationship between obesity and a sedentary lifestyle since the frequency of physical exercise practiced by the study participants was not evaluated; only the practice of any physical activity was verified. Nor can a relationship be established with the sex of the patients, although the highest proportion was female (55.7%).
However, the Brazilian Guidelines on Hypertension states there is a relationship between a sedentary lifestyle and hypertension since the lack of physical activity is $27.5\%$, with a higher prevalence among women $(31.7\%)$ than men $(23.4\%)$, confirming the profile found in the sample studied (2,16).
Ethnicity is also considered an essential factor for hypertension because non-white individuals are more likely to develop higher cardiovascular risk. Non-white individuals (90.2%) were the majority in the study population, consistent with the ethnicity prevalent in the region (2).
Regarding the education/instruction of the individual, it is associated that the lower level of education can generate limited conditions of absorption of information to people about their health, linking to more illness and negative correlation with the prevention, control of hypertension, and treatment adherence. In the sample, we obtained $32.8\%$ of individuals with incomplete primary education and $13.1\%$ with no education, with a total of $43.9\%$ of people with little or no education, which seems to be a more relevant factor for the differences in the prevalence of hypertension than ethnic implication itself.
In addition to risk factors being predictors of outcomes, hypertensive patients should periodically undergo laboratory tests, and these, when associated with traditional cardiovascular risks, can assist in this stratification. In hypertensive patients, it is also essential to investigate associated comorbidities, especially DM.
According to the Guidelines of the Brazilian Society of Diabetes, fasting glucose levels for nonpregnant adults are considered normal when they vary between $70 - 99\mathrm{mg / dL}^{(17)}$. In the study, $71.1\%$ of the patients in the sample presented glycemic changes, which corroborates directly with the increase in CV risk $(60.6\%)$.
Smoking is associated with the development of albuminuria, which may contribute to progressive kidney disease and increased risk of CVD (14,18). According to the Dialysis Morbidity and Mortality Study (DMMS) Wave 2, $40\%$ of patients on dialysis are current smokers $(16.6\%)$ or former smokers $(24.2\%)$ (19). Smoking has vasoconstrictive, thromboembolic, and direct effects on the vascular endothelium and is a strong predictor of increased serum creatinine levels in non-diabetic patients 65 years of age and older (20, 21).
Among the inflammatory markers is IL-6, a proinflammatory cytokine that acts in different tissues, mainly concerning immune and humoral effects, and is released primarily by adipocytes (22-24). Visceral adipose tissue releases about 15 to $30\%$ of all IL-6 production (23). This fact strengthens the inclusion of obesity as one of the risk factors for CVD (23).
IL-6 also has effects on carbohydrate and lipid metabolism. As adipose tissue is an essential source of this cytokine, in obese individuals, IL-6, as a potent stimulator of CRP, can inhibit the activity of lipoprotein lipase, causing a low glucose uptake mediated by insulin, increasing insulin resistance, exemplified in table 3, which shows the direct relationship of glycemia and IL-6, as well as CRP $^{(25,26)}$.
The neutrophil/lymphocyte ratio (NLR) can be used as an easy marker of integration into the laboratory routine at virtually no additional cost. There is an increase in NLR when there are inflammatory events ${ }^{(27)}$.
High serum levels of CRP indicate a higher risk of the individual developing coronary and cardiovascular diseases, through the elevation of BP, by hemodynamic, hormonal, and biomechanical mechanisms (28-32). In the sample, hypertensive patients with higher abdominal circumference and BMI had the highest values of CRP, showing that obesity is directly related to hypertension. A direct relationship was also established between CRP and glycemia and IL-6, reaffirming cardiovascular risk.
On the other hand, Ferritin is associated with the presence of anemia and, in high concentrations, implies iron overload, resulting in oxidative stress, therefore participating in the inflammatory effect. No impact of anemia was detected in the population studied. However, it is considered a non-traditional risk factor in the development of cardiovascular diseases, as it contributes to myocardial hypertrophy and indirectly to higher mortality of patients with CKD (17, 33).
The results of the present study should be analyzed considering some limitations. Despite being a population-based sample, the individuals allocated were limited to those treated in a reference health unit linked to the Family Health Strategy, which may affect the generalization of the results. Another limiting fact is based on the food issue. Although eating habits have an important impact on BP reduction, this study should have evaluated them, considering the logistical difficulty in applying dietary recalls. However, all participants were asked if the unit's professionals about adopting consistent eating habits to control hypertension instructed them. Another question infers the sample size; although it is sufficient for the analysis, there is a limitation of the cross-sectional design, making it impossible to establish causal relationships between exposure and disease development.
In conclusion, although hypertension has a multifactorial etiology, obesity, smoking, and glycemia were the risk factors positively correlated with it. Given this, it is essential to intensify the control of hypertension and cardiovascular risk factors, aiming to reduce or control morbidity and mortality through prevention and better quality of life for the population.
Generating HTML Viewer...
References
32 Cites in Article
Luis Peres,Ademar Cunha Júnior,Alex Schäfer,Aline Silva,Arianne Gaspar,Deborah Scarpari,Julia Alves,Rodolfo Girelli Neto,Thaís Oliveira (2013). Biomarkers of acute kidney injury.
Anne Groth,Maria Closs Ono,Viktoria Weihermann,Luísa Brasil Bastos,Thamyle Rezende,Deisy Dalke,Catharina Borssuk Ferreira (2018). A Picture of Breast Reconstruction in a Public Oncology Hospital in Latin America: A Ten-Year Experience.
Fabiane Francisqueti,André Nascimento,Camila Correa (2015). Obesidade, inflamação e complicações metabólicas.
N Ouchi,Parker Lugus,J Walsh,K (2011). Adipokines in inflammation and metabolic disease.
A Trzeciak-Ryczek,B Tokarz-Deptuła,P Niedźwiedzka-Rystwej,W Deptula (2011). Adipose tissue -component of the immune system.
T Suganami,Y Ogawa (2010). Adipose tissue macrophages: their role in adipose tissue remodeling.
Fernanda Oliveira,Maria Alves,Aline Bezerra (2009). Co-morbidades e mortalidade de pacientes com doença renal: atendimento terceirizado de nefrologia.
Kazutoshi Fujibayashi,Hiroshi Fukuda,Hirohide Yokokawa,Tomomi Haniu,Fukuko Oka,Miki Ooike,Toshiaki Gunji,Noriko Sasabe,Mitsue Okumura,Kimiko Iijima,Teruhiko Hisaoka,Hiroshi Isonuma (2012). Associations between Healthy Lifestyle Behaviors and Proteinuria and the Estimated Glomerular Filtration Rate (eGFR).
(2013). Notice.
Paulo Lotufo (2008). O escore de risco de Framingham para doenças cardiovasculares.
Stefan Pilz,Simona Iodice,Armin Zittermann,William Grant,Sara Gandini (2011). Vitamin D Status and Mortality Risk in CKD: A Meta-analysis of Prospective Studies.
Andrew Levey,Lesley Stevens,Christopher Schmid,Yaping Zhang,Alejandro Castro,Harold Feldman,John Kusek,Paul Eggers,Frederick Van Lente,Tom Greene,Josef Coresh (2009). A New Equation to Estimate Glomerular Filtration Rate.
Fli Pontes,Junior,J Prestes,R Leite,D Rodriguez (2010). Influence of aerobic training on the pathophysiological mechanisms of systemic arterial hypertension.
Brazil (2020). Clinical Protocol and Therapeutic Guidelines for Type 1 Diabetes Mellitus.
Stephan Orth,Eberhard Ritz,Robert Schrier (1997). The renal risks of smoking.
A Stack,B Murthy (2010). Cigarette use and cardiovascular risk in chronic kidney disease: an unappreciated modifiable lifestyle risk factor.
Stephan Orth,Axel Stöckmann,Christian Conradt,Eberhard Ritz,M Ferro,W Kreusser,G Piccoli,M Rambausek,D Roccatello,K Schäfer,H Sieberth,C Wanner,B Watschinger,P Zucchelli (1998). Smoking as a risk factor for end-stage renal failure in men with primary renal disease.
Anthony Bleyer,Lynn Shemanski,Gregory Burke,Kimberley Hansen,Richard Appel (2000). Tobacco, hypertension, and vascular disease: Risk factors for renal functional decline in an older population.
Martin Lotz (1995). Interleukin-6: A comprehensive review.
Jc; Sanchez,Z Df; Lopez,O Finch (2010). Adipokines and the metabolic syndrome: multiple aspects of a complex pathophysiological process.
Gemma Francisco,Cristina Hernández,Rafael Simó (2006). Serum markers of vascular inflammation in dyslipemia.
Carla Silva,Teixeira (2014). Prediction of plasma concentrations of IL-1B, IL-6, and TNF-α by clusters of cardiovascular risk factors in adolescents.
M Heliövaara,A Teppo,S Karonen,J Tuominen,P Ebeling (2005). Plasma IL‐6 concentration is inversely related to insulin sensitivity, and acute‐phase proteins associate with glucose and lipid metabolism in healthy subjects.
Heitor Santos,Luiz Izidoro (2018). Neutrophil-Lymphocyte Ratio in Cardiovascular Disease Risk Assessment.
David Chappell,Signe Varner,Robert Nerem,Russell Medford,R Alexander (1998). Oscillatory Shear Stress Stimulates Adhesion Molecule Expression in Cultured Human Endothelium.
Shunichiro Komatsu,Julián Panés,Janice Russell,Donald Anderson,Vladimir Muzykantov,Masayuki Miyasaka,D Granger (1997). Effects of Chronic Arterial Hypertension on Constitutive and Induced Intercellular Adhesion Molecule-1 Expression In Vivo.
Kenichi Yasunari,Kensaku Maeda,Munehiro Nakamura,Junichi Yoshikawa (2002). Oxidative Stress in Leukocytes Is a Possible Link Between Blood Pressure, Blood Glucose, and C-Reacting Protein.
R Rocha (2002). Aldosterone induce a vascular inflammatory phenotype in the rat heart.
Claudia Chae,Richard Lee,Nader Rifai,Paul Ridker (2001). Blood Pressure and Inflammation in Apparently Healthy Men.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Bettanin, Francelise Susan Mihara. 2026. \u201cInflammatory Markers and Risk Factors in Hypertensive Patients: A Cross-Sectional Study\u201d. Global Journal of Medical Research - F: Diseases GJMR-F Volume 23 (GJMR Volume 23 Issue F2): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































