## I. INTRODUCTION
Laparoscopic cholecystectomy (LC) is the most common elective laparoscopic procedure performed globally and is the gold standard treatment for gallstone disease. (1)
Variations in biliary anatomy are frequently encountered, Of these, a double gallbladder (GB), with or without duplication of cystic duct is a very rare surgical encounter, with an incidence of approximately 1 in 4000–5000 population (2)
Although duplicated gallbladder is found in both genders, its prevalence is higher in females. (3) Symptomatic conditions of duplicated gallbladder are usually associated with cholecystitis, cholangitis, gallstone disease, and pancreatitis but are rarely diagnosed with carcinoma. (3) Surgery is considered to be the ideal treatment choice of symptomatic duplicated gallbladder. (3) Failure to recognise the presence of a double GB in asymptomatic patient has required a repeat cholecystectomy for symptomatic gallstone disease in some instances to remove the missed second GB. However, there is currently no indication for a cholecystectomy in the asymptomatic patient if duplication of the GB was to be detected incidentally during the course of imaging for unrelated conditions (2).
Duplication of the gall bladder may be associated with duplication of cystic duct; the anatomy should be precisely visualized during surgery to avoid injuries to other structures (4). The anatomic variations of gallbladder duplications were classified based on the location and number of cystic ducts. (5) Type 1 includes gallbladder duplication separated with a septum and two separate gallbladders that fuse in the neck to form a single cystic duct; type 2 includes accessory gallbladders with two different cystic ducts (6)
The symptoms and signs of gallbladder duplication are like those of patients with a single gallbladder.(7) When diagnosed incidentally, prophylactic cholecystectomy is not required (3). Nevertheless, appropriate diagnosis is necessary to avoid biliary tract injuries that can occur during surgeries, postoperative complications, or a need for a reparative procedure (3,4)
## II. CASE PRESENTATION
41-year-old lady presented to the outpatient clinic on 30/06/0221 as a case of symptomatic cholelithiasis and obesity with a BMI of 36. Patient have undergone 4 C-sections that last one was 2 years ago. She started complaining of right upper quadrant pain episodes radiating to the back that was triggered by fatty food with no attacks of nausea/vomiting, dark urine, pale stool or jaundice. Her pre-operative liver function test was unremarkable. The biliary ultrasound that was done on 07/07/2022 showed a gallbladder with average distention showing multiple mobile echogenic stones casting shadows with reserved wall thickness and no pericholecystic collection, CBD was unremarkable. Based on that; laparoscopic cholecystectomy was planned.
Intraoperatively, the Pneumoperitoneum was created through a closed technique and insertion of the optical ports under vision in the left subcostal space. Three more secondary trocars were inserted.
Extensive adhesions between the gallbladder and the omentum were identified. The fundus of the gallbladder was retracted over the doom of the liver, and it was difficult due to large sized double looking gallbladder and the infundibulum was retracted in lateral direction exposing the triangle of calot. Adhesions were lysed sharply with gentle traction and Retrograde dissection was performed over the peritoneum overlying the infundibulum at which the cystic artery and double tubed cystic duct were identified then circumferential dissection was done and double clipping of both cystic duct and cystic artery were done. Afterheat, the gallbladder was then excised from its hepatic peritoneal attachment by electrocautery as the dissection proceeded. open examining the gallbladder after retrieving it, it was found to have double gallbladder with double cystic duct as it was confirmed intraoperatively No associated artery was identified no bile leak was found the remainder of the operation was routine. The patient's recovery was uneventful, and she was discharged on day one post op.
The gross specimen of histopathology was found to be: V-type gallbladder duplication. The first gallbladder measures $8.0 \times 3.0$ cm and $0.1 \, \text{cm}$ wall thickness. The second one measures $6.5 \times 2.0$ and $1.0 \, \text{cm}$ wall thickness. There is one stone entrapped in the neck measuring $0.3 \, \text{cm}$. The first gallbladder contains three stones with the biggest one measuring $0.6 \, \text{cm}$. It has rigid wall and flat pale mucosa with stone dust. The second gallbladder has green velvety mucosal surface with no stone. The serosal surface of both are smooth and glistening. Diagnosis for both first and second gallbladder shows chronic calculus cholecystitis.
## III. DISCUSSION
Gallbladder duplication is a rare congenital anomaly (3). Anticipation and recognition of this anomaly and its various types are important to avoid surprises therefore preoperative diagnosis plays a crucial role in planning surgery and preventing possible surgical complications or re-operation if accessory gallbladder has been overlooked during initial surgery (3,4,7).
during which a single primordium bifurcates (1). The time that bifurcation occurs determines the type of duplication that will occur i.e., the earlier the bifurcation; the more complete the degree of duplication (1). A true accessory gallbladder arises from two separate primordia on the biliary tree and possesses a separate cystic duct (5). Histologically, gallbladder duplication is differentiated from a choledochal cyst by the presence of a muscular wall with an epithelial lining (3). In 1929 Boyden reported 20 cases of double gallbladder he found in the literature from 1674 to 1929, He described a system to classify gallbladder duplications including "vesica fellea divisa"(bilobed gallbladder that has one cystic duct) and "vesica felleaduplex" (true gallbladder duplication) (1).
The latter is subclassified into "Y-shaped type" (two cystic ducts uniting before entering the common bile duct), and "H-shaped or ductular type" (two cystic ducts enter separately into the common bile duct) (Table1) (5). In 1936, Gross described congenital abnormalities of gallbladder and classified them into six types labelled A-F (4). In 1977, Har-laftis et al. further modified the classification by describing two main types based on morphology and embryogenesis (2). Although his classification is the most universally accepted, a modified Harlaftis classification has been reported in the literature by describing a left trabecular variant to type 2 classification (6). Has-san et al. reported an accessory gallbladder branching from both the left and right hepatic ducts (7). Causey et al. reported a new variant in which a septated type 1 gallbladder has 2 cystic ducts(8). Our case represents V-shaped type.
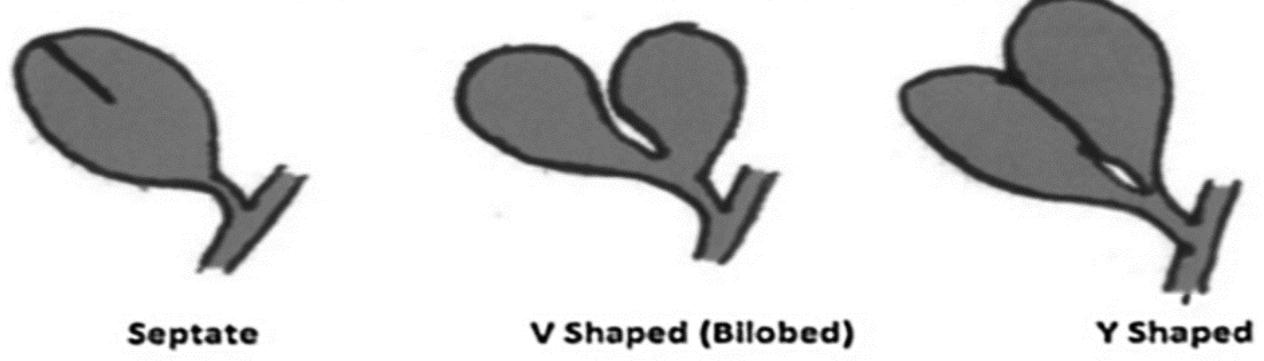 Table 1: Boyden's system classification of duplicated GB Type 1: Split Primordlum Group
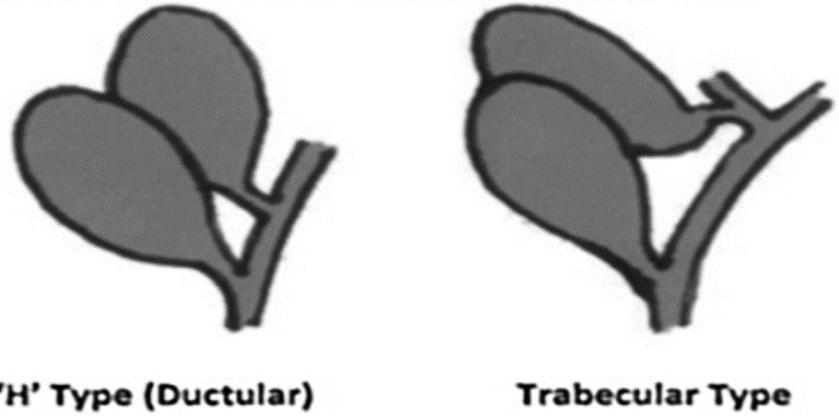 Type 2: Accessory Gallbladder Group
Diagnosing duplicated
gallbladder preoperatively greatly improves the surgical outcome and reduce the risk of complications (3,4). In addition, thorough knowledge of the anatomical variations of the gallbladder and cystic duct greatly aids the surgeon in anticipating duplications, managing it accordingly and avoiding any complications (7,8,9).
All surgeons should be aware of this rare congenital abnormality of the gallbladder, which requires particular attention to preoperative radiographic studies and special attention to the biliary ductal and arterial anatomy during cholecystectomy.
## IV. CONCLUSION
Duplication of the gallbladder is a rare congenital abnormality, which requires special attention to the biliary ductal and arterial anatomy. Furthermore, the preoperative diagnosis in most of cases cannot be achieved. Failure to recognise the presence of a double GB in asymptomatic patient has required a repeat cholecystectomy for symptomatic gallstone disease in some instances to remove the missed second GB [8]. However, there is currently no indication for a cholecystectomy in the asymptomatic patient if duplication of the GB was to be detected incidentally during imaging for unrelated conditions.
LC Laparoscopic Cholecystectomy
GB Gallbladder
### ACKNOWLEDGEMENTS
Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2022R306), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia
Authors contribution
Nouf Tuhaif Algahtani: Concept and design of study, data collection, literature review, drafting, revision.
Monira Khalid Alhasan: Concept and design of study, data collection, literature review, drafting, revision
Saeed Saad Alshlwi: revision, approval of final manuscript
Abdullah Saleh Alhudaib: revision, approval of final manuscript
Ahmed Abdulhamid Alanazi: revision, approval of final manuscript
Guarantor
Saeed Saad Alshlwi.
Conflict of interest
All the contributing authors declare that they have no conflicts of interest.
Funding
No funding.
Availability of data and materials
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report. A copy of the written consent is available for review from the editor of this journal.
Ethical approval
Not applicable
Generating HTML Viewer...
References
8 Cites in Article
Tim Harding,Enda Hannan,Conor Brosnan,William Duggan,David Ryan,Anthony Stafford,Donal Maguire (2020). The dilemma of the duplicated cystic duct: a case report.
Mohammud Musleh,Hugh Burnett,Balashanmugam Rajashanker,Basil Ammori (2017). Laparoscopic double cholecystectomy for duplicated gallbladder: A case report.
A Bawazir,O Bawazir,R Bawazir (2021). A pediatric case of double gallbladder with gallstone.
Sardar Arif,Ihsan Hussein,Ayad Mohammed (2019). Duplicated gall bladder with gall bladder polyp presenting with cholecystitis.
Jai Singh (2021). Duplication of the Gallbladder as an Operative Surprise: A Case Report with Review of the Literature.
Kabul Gürbulak,E Özşahin,H Düzköylü,Y Akgün,I Battal,M Gürbulak,B (2015). Single incision laparoscopic cholecystectomy for gallbladder duplication.
Yagan Pillay (2015). Gallbladder duplication.
Aziza Al Rawahi,Yahya Al Azri,Salah Al Jabri,Abdulrazaq Alfadli,Suad Al Aghbari (2016). Successful laparoscopic management of duplicate gallbladder: A case report and review of literature.
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.