Intraosseous synovial cysts (ISCs) are rare occurrences characterized by synovial proliferation within the bone. This article presents a case report of a 19-year-old patient with a carpal scaphoid bone fracture and an incidentally detected intraosseous cyst. The patient underwent surgical treatment involving careful curettage of the cystic cavity, addition of a spongy bone graft, and fracture stabilization. The histopathological examination confirmed the presence of an intraosseous synovial cyst. The patient achieved a satisfactory functional outcome, with early consolidation and resumption of daily activities. The study emphasizes the importance of accurate diagnosis and appropriate surgical management, highlighting the favorable prognosis and rarity of recurrences in intraosseous synovial cysts of the scaphoid bone.
## I. INTRODUCTION
Intraosseous synovial cysts (ISCs) are characterized by the presence of a specific radiological image and histology indicating synovial proliferation within the bone (1). Intraosseous synovial cysts of the scaphoid bone are an extremely rare cause of wrist and hand pain. The localization of this cyst specifically in the scaphoid bone is sparsely documented in the literature. This article presents a case report of a 19-year-old patient who experienced a carpal scaphoid bone fracture following a sports-related accident. Additionally, during the evaluation, an intraosseous cyst was incidentally detected.
## II. CASE REPORT
It is about a 19-year-old patient with no notable medical history. He came to the emergency department of CHU Avicenne after sustaining an injury to his left upper limb during a sports accident, with his hand landing in hyperextension. During the interview, he mentioned having experienced previous injuries and suffering from chronic wrist pain for the past 3 months, which is relieved by symptomatic treatment with painkillers and non-steroidal anti-inflammatory drugs. Upon clinical examination, the patient exhibited slight limitation of wrist function, accompanied by swelling and filling of the anatomical snuffbox. Palpation elicited pain during thumb retroversion and wrist pronation, as well as tenderness upon pressure in the anatomical snuffbox.
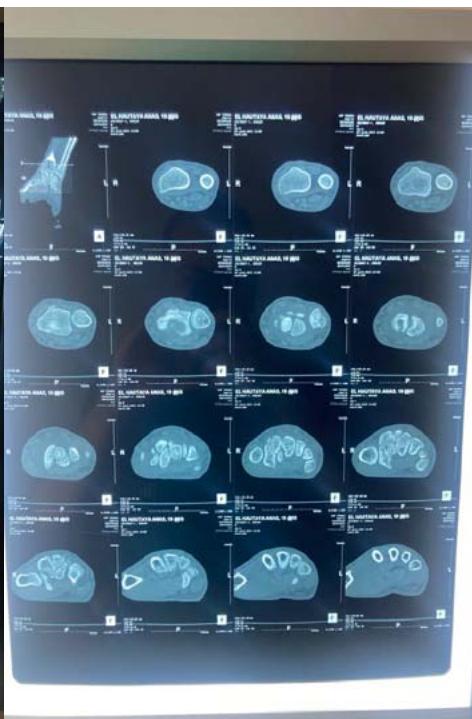
The standard radiographic assessment revealed a scaphoid fracture with an underlying gap, suggesting the possibility of a cyst or pseudarthrosis of the scaphoid (figure 1). The wrist CT scan confirmed the scaphoid fracture with a probable intraosseous cyst (figure 2).

 Figure 1: The standard X-ray of the wrist, in frontal and oblique views, revealed a displaced fracture of the scaphoid on a lacunar image located in the middle portion of the scaphoid.

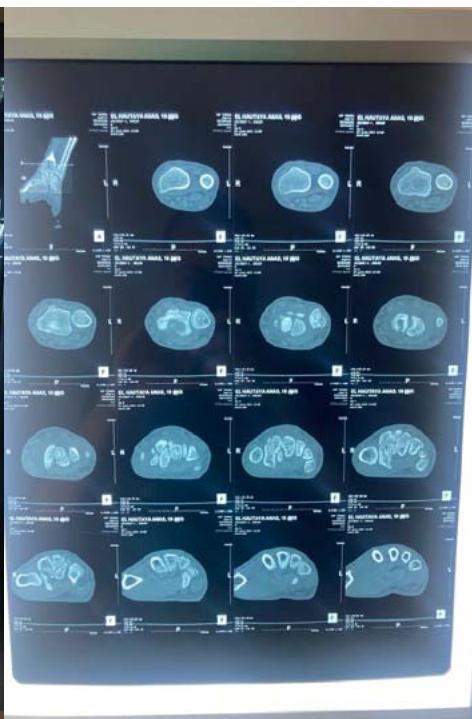 Figure 2: The computed tomography (CT) scan confirmed the scaphoid fracture and the localized and nonaggressive nature of the cyst.
The patient underwent surgery via an anterior approach. Careful curettage of the cavity was performed after distraction of the fracture site. The bone defect was filled with autologous cancellous graft harvested from the lower metaphysis of the ipsilateral radius. Fracture stabilization was achieved with 2 pins (figure 3). The histopathological examination of the curettage specimen showed that the cyst wall was lined with flattened fibroblastic cells resembling synovial cells, without true epithelial appearance. There was no mucoid degeneration or myxoid transformation.
 Figure 3: Postoperative radiograph after curettage, grafting, and stabilization with two pins.
The patient was immobilized for 2 months in a resin splint. After this period, the hardware was removed under local anesthesia. Several sessions of functional rehabilitation were initiated after plaster removal. At the latest follow-up at 6 months after treatment, the patient had regained good wrist function, with painlessness and resumption of leisure and professional activities.
## III. DISCUSSION
Cysts of the carpal scaphoid are uncommon in daily practice. Most often, they are either mucoid cysts or synovial cysts. These cysts typically develop at an advanced age, with an average age of 41 and 47 years in the two largest series [2].
The pathophysiology of bone cysts remains controversial, with two main opposing hypotheses. Some authors argue that the bone cyst forms through synovial inclusion from the outside to the inside. Others suggest synovial metaplasia originating within the bone itself, potentially influenced by local microtrauma or ischemic phenomena [3,4].
Intraosseous synovial cysts can present in two distinct ways: they may not exhibit any symptoms or they can result in moderate pain that typically does not respond well to painkillers. Other clinical manifestations may arise due to complications associated with intraosseous synovial cysts [1, 5, 6], such as wrist swelling caused by the rupture of the cysts and the spread of its contents within the joint. Moreover, a pathological fracture can occur, exacerbating the pain [1,5].
From a radiological perspective, typical images show osteolytic lesions of a few millimeters in diameter, either solitary or multilobulated, accompanied by a peripheral rim of osteosclerosis [7]. This description corresponds to the lesion observed on our patient's radiographs, along with a discontinuity at the scaphoid neck, indicating a pathological fracture due to weakening of the scaphoid neck. Computed tomography, whether performed with or without contrast agent injection, allows for precise determination of the nature of the intracystic contents and any cortical involvement [1,7]. It also helps establish a surgical protocol by specifying the most appropriate approach, including the preferred surgical access route.
The only patients requiring surgical intervention are those who experience persistent pain or swelling of soft tissues, as well as those with a pathological fracture, as in our case. Additionally, preventive intervention may be considered for lesions at risk of fracture due to their location (scaphoid neck) and volume (large geode with significant cortical thinning) [8]. The surgical procedure involves a thorough excision by cureting the contents of the cystic cavity as completely as possible. A spongy bone graft is systematically added, along with osteosynthesis if necessary, as recommended by most authors [9,10]. The functional prognosis is generally favorable, and recurrences are exceptional (5). In our case, we observed an early consolidation (55 days) compared to the usual timeframe of 3 months, with a highly satisfactory functional outcome.
## IV. CONCLUSION
The functional prognosis of intraosseous synovial cysts of the scaphoid bone is generally favorable, with exceptional recurrences. In our case, we observed an early consolidation occurring in just 55 days compared to the usual timeframe of 3 months, with a highly satisfactory functional outcome. This case report highlights the importance of accurate diagnosis and appropriate surgical management for patients with intraosseous synovial cysts of the scaphoid bone. Careful curettage of the cystic cavity and the systematic addition of a spongy bone graft, along with possible osteosynthesis, were recommended to ensure complete excision and optimal consolidation. Standard radiography and computed tomography were valuable tools in confirming the diagnosis and guiding the surgical treatment. Through appropriate management, the patient was able to regain satisfactory wrist function and resume daily activities. However, long-term monitoring is necessary to detect any potential recurrences. This study also emphasizes the importance of ongoing research and documentation of intraosseous synovial cysts of the scaphoid bone to improve understanding of their pathophysiology and treatment options.
Ethics approval and consent to participate
Ethical approval was not sought. Written consent was obtained from the patients.
Availability of data and materials
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors contributions
All authors Have read and approved the final manuscript.
Generating HTML Viewer...
References
10 Cites in Article
C Chantelot,P Laffargue,E Masmejean,B Peltier,P Barouk,C Fontaine (1998). Fracture du scaphoïde carpien sur kyste intra-osseux.
Samuel Logan,Louis Gilula,Michael Kyriakos (1992). Bilateral scaphoid ganglion cysts in an adolescent.
E Masmejean,J-Y Alnot,C Chantelot,R Beccari (2000). La prothèse trapèzométacarpienne anatomique Guepar.
M Yakoubi,N Meziani,M Yahia Cherif,A Zemmouri,R Benbakouche (2009). Fracture pathologique du scaphoïde carpien (kyste synovial intraosseux). Aspect clinique et thérapeutique. À propos d’un cas.
S Logan,L Gilula,M Kyriakos (1992). Bilateral scaphoid ganglion cysts in an adolescent.
Ignacio Uriburu,Violeta Levy (1999). Intraosseous ganglia of the scaphoid and lunate bones: Report of 15 cases in 13 patients.
E Masmejean,J-Y Alnot,C Chantelot,R Beccari (2000). La prothèse trapèzométacarpienne anatomique Guepar.
H Mestdagh,Y Butruille,C Maynou,J Delobelle,M Lecomte-Houcke (1993). Les kystes synoviaux intraosseux du carpe. À propos de trois cas.
H Forstner (1992). A28: Geode (Also Referred to as Subchondral Cyst and Osteoarthritic Cyst); Soft Tissue and Intra-osseous Ganglion (Also Referred to as Intra-osseous Ganglion, Juxta-articular Bone Cyst, and Periosteal Ganglion).
M Waizenegger (1993). Intraosseous Ganglia of Carpal Bones.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Marouane Dinia. 2026. \u201cIntraosseous Synovial Cysts of the Scaphoid Bone: A Rare Case of Fracture and Surgical Management\u201d. Global Journal of Medical Research - H: Orthopedic & Musculoskeletal System GJMR-H Volume 23 (GJMR Volume 23 Issue H2).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.