



I. INTRODUCTION
According to their self-image as generalists, G.P.s specialize in the whole person (1) and thereby apply a biopsychosocial approach to health and illness (2). However, to synthesize the various aspects in a case-specific way, G.P.s - and other health professionals - must apply their specialist knowledge to specific situations and cases. For this, they need a "hermeneutic understanding of the case" (3, 4): "General Practice takes somatic, psycho-social, socio-cultural and ecological aspects into account. When interpreting symptoms and findings, it is particularly important to appreciate the importance of the patient's understanding of his disease, his environment, and personal history (hermeneutic approach). (3)
However, physicians do not learn these basic skills in education, training and continuing education. Fortunately, most of them already have some of the relevant competencies based on their pre- and nonprofessional experience and continue to develop them in their everyday practice. Ortmann, therefore aptly speaks of the "family doctor as an inventor" (5). Accordingly, GP's action varies with the practitioner and the respective contexts, which are given, among other things, by the respective biographical experiences, the current life situation, the framework conditions of the treatments, and the relationship of the participants. Person-centered medicine becomes possible by encountering "whole people" in a specific setting. So far, this core of GP activity has received little attention in the science of general practice, which tends to focus on the formality of medical roles and the rule-based nature of procedures.
Viktor von Weizsacker, the founder of the Heidelberg School of Anthropological Medicine, had already called for the "introduction of the subject into medicine" in the first third of the 20th century and justified this epistemologically with reference to the findings of physics, morally against the background of human rights and clinically under the aspect of value-guided coordination processes on treatment goals (6, 7). Furthermore, Weizsacker underlined that the relationship between the sick person (or person seeking help) and his or her helper is a companionship, independent of professional specialization, and should be the basis of general (or anthropological) medicine (6). More recently, similar considerations have been taken up again under the aspect of person-centeredness.
The characteristic features of person-centeredness are conceptually derived from the findings of various sciences (such as philosophy, psychiatry, pedagogy, sociology, systems theory, neuroscience, and linguistics, for example) on the one hand and on the experiences of practicing health professionals ("reflective practice") on the other. Mezzich names the following principles in his overview:
- Ethical commitment
- Cultural awareness and responsiveness
- Holistic approach, relational focus
- Individualization of care
- Collaborative diagnosis and shared decision-making
- People-centered organization of services
- And person-centered education and research (8).
Thus, person-centered medicine can be defined in summary by Mezzich et al. as "promoting the care of the person (of the totality of the person's health, including its ill and positive aspects), for the person (promoting the fulfillment of the person's life project), by the person (with clinicians extending themselves as full human beings with high ethical aspirations) and with the person (working respectfully, in collaboration and in an empowering manner)". (9, emphasis mine, OB)
II. FROM "PATIENT AS TEXT" TO DIALOGUE-BASED MEDICINE
In an essay published in 1986, Daniels emphasizes that medical action has always implied interpretative acts (10). However, the art of interpretation ("hermeneutics"), anchored in the humanities, receives little attention as a methodological procedure in medicine. He proposes to understand the patient as a "text" analogous to literary works, distinguishing four levels:
- The primary text refers to bodily layered life experiences that are expressed, among other things, in symptom formations.
- For these to become legible, a (spoken and written) medical history must be collected and, thus, a secondary text generated.
- The physician's task is then to interpret these two texts, which leads to a diagnosis and, using documentation, to a third-order text.
- Therapeutic action constitutes the fourth text by (re)interpreting the patient's problem regarding the patient's social context. To do this, the therapist must empathically engage with the patient and use a prior understanding of what is meaningful for the patient ("hermeneutic circle"). However, the
practitioner is not unaffected by this, so the consultation extends into the lifeworld of both participants.
Daniels' proposal was taken up, critically discussed, and expanded. Not only does the doctor decode the messages, but this takes place constantly in everyday life in concrete interactions and self-reflexive acts and is also embedded as professional action in dialogues. At least the following dimensions can be distinguished:
- Patient as "text" - doctor as "interpreter" (10)
- Patient as "text" and as "interpreter" (11)
- Patient as "text" and as "interpreter" - doctor as "interpreter" against the background of pre-existing "scripts" ("illness is between people", (6))
- Patient as "text" - patient and doctor as joint interpreters and authors of a modified "text" (12)
- Patient as "text", doctor as "con-text" - patient and doctor as collaborative interpreters and authors of modified "texts" (13)
- Patients and physicians as individual and collaborative readers and texters against the background of existing and changing scripts.
III. THE LAYERING OF MEANING
The layering of meaning is a process (table 1): The members of a society are born into a field of meaning that has materialized in symbols and is constantly produced and expanded in concrete interactions 1. This social body of knowledge contains ideas about health and illness and the appropriate way to deal with them. On an individual level, life-world experiences [2] form the background for (possibly crisislike) (bodily) experiences of people who are/will potentially become patients [3] and evaluate their experiences themselves against the background of their concepts of health and illness [4]. If those affected - or their relevant reference group - ascribe disease value to the phenomena, this can lead to medical care utilization. The patient's experiences and self-interpretations thus become symptoms [5], perceived by the physician [6], and recorded in the form of findings [7]. The doctor synthesizes them into diagnoses [9] against the background of his or her individually and professionally developed health/illness and treatment concepts [8]. The doctor's own crisis management experiences [10], the shared treatment history [11] as well as the patient's readiness for treatment and possibility of change [12] frame - in addition to the inherent dynamics of the processes to be interpreted and the resources available in the social environment - the prognosis [13], based on which the therapy plan [14] is developed. Whether the therapy is helpful or not [16] is ultimately determined by whether the patient (and his or her reference system) can successfully cope with (modified) everyday life [15].
Defining "success" is ultimately left to the patient [17] and is done about a future-oriented concept of a meaningful life. However, these assessments are potentially in competition with interpretations made from other perspectives (in particular, the doctor, social reference system, and funding agency) [18].
| 1. prior social production of meaning fields and symbols | |
| Patient's lifeworld | 2. individual experiences of crisis and coping |
| 3. current (crisis) (bodily) experiences of (potential) patients | |
| 4. health and illness concepts of (potential) patients | |
| 5. complaints and symptoms | |
| Medical world | 6. perceptionsofthedoctor |
| 7. findings | |
| 8. health/disease and treatment concepts of the doctor | |
| 9. diagnoses | |
| 10. crisis management experiences of the doctor | |
| 11. joint treatment experiences of patient and doctor | |
| 12. the patient's willingness to change/treat | |
| 13. prognosis | |
| 14. therapy plan | |
| Patient's lifeworld | 15. patient's willingness and ability to implement treatment |
| 16. changed everyday coping | |
| 17. patient'sfeelingofrecovery | |
| 18. evaluation as therapy (failure) success | |
The question is no longer whether medical action is (also) a hermeneutic endeavor but how this is done. In particular, one has to clarify which "case" is to be understood in the sense of the GP's way of working.
IV. THE VIEW OF THE CASE
According to a widespread understanding in medicine, patients represent individual manifestations of a case of something, which is to be elicited and treated according to the appropriate guideline. From a time perspective, a case can denote a single consultation, a treatment episode, or also the development in the course. The developmental dynamics come to the fore concerning the disease entity. If one focuses on the doctor-patient interaction, their relationship and the course of treatment can become a case (13-15). If the patient's life world and biography are taken into account, the respective way of coping with oneself and the world ("staging") can be determined and processed as a case. Finally, the rules that become effective in the respective social reference group (family, work, community) can be considered. So, the social system becomes a case. Other possible case levels concern professional action. Thus, the personal style of the individual doctor, performed in different interactions, can be questioned in supervision concerning its patient-related appropriateness and traced in a biographical perspective in its life-historical shaping (16, 17). In a comparative analysis, the modes of action common to different doctors and their structural foundations point to the respective professional profile. Differences between other practitioners can become an occasion for reflection on what is appropriate. The case can be constructed at each level of meaning stratification described above and can be understood in the tradition of structural hermeneutics (18) in terms of the "structuring law of a social practice". Understanding means becoming aware of its latent social meaning.
At which level(s) of trapping the definition of the professional society DEGAM is aimed is unclear. A personal understanding subject is almost entirely missing. The patient, who is to be understood holistically, is confronted with "general practice". Thus, the discipline does not perceive its subject basis in its self-definition. This is all the more astonishing since, in statistical analyses, "the doctor factor" is attributed to the most significant part in explaining the large differences in process and outcome quality in primary care (19).
Wanting to treat the whole person corresponds to the idealized professional self-image of many health professionals and the wishes of many patients (20 - 22). However, comprehensive care is rarely realized. As can be seen from well-documented individual cases, person-centeredness is nevertheless possible (e.g. 4, 23). Suppose (general) practitioners - and their patients who co-create their treatment - are "inventors". In that case, it should be possible to make person-centeredness comprehensible by reconstructing their interactions and shaping everyday life that precedes or follows them. In particular, it seems useful to analyze specific cases of "positive deviant behavior" (24) in the sense of salutogenesis to elaborate on conditions for a successful person-centered practice.
V. THE INTRODUCTION OF THE SUBJECT
Health-related processes and health-related actions are permanently embedded in the social actions of concrete persons and are inevitably interpreted in terms of their social meaning. Even if the interpretation concepts of participants, social environment, and professional helpers may differ, they are always attributions by persons who should be aware of their subjectivity and make it comprehensible. Mezzich's definition of person-centeredness is also applicable to health-related research (9). It, too, needs to be person-centered and framed as a collaborative interpretive effort. Therefore, health researchers are in need of a specific basic attitude, methodological competencies, and the willingness of all actors to cooperate (25).
Person-centered health research presupposes humility, self-reflexivity, respect for participants, a desire to understand others, and interpretive communities grounded in mutual connectedness as human beings (26). These principles are claimed for health-related research and practice similarly. The concrete design varies depending on the directness of the interactions - and thus on the respective case level. As this is a highly complex process (27, 28), it is impossible to consider the case levels outlined here simultaneously. I will limit to exemplary hints from my research practice or that of colleagues I know personally (as a first approximation, see Table 2).
| Dimension | Expression of affected person's competence | Researchers's Subjectivity | Methodology |
| The patient's life world | Narration and self-reflectionFacial expression, gesturesPictures, Photos | Active listening and self-reflectionFacial expressions, gestures, and counter-transference analysisSelf-insertion | Biographical interviews,narrativesDocument analysis (e.g. diary, photos) Participatory observation Interaction Analysis |
| Medical world | Narration and self-reflectionDesign of the setting | Active listening and self-reflectionFacial expressions, gestures, and counter-transference analysisSelf-insertionCreativityGestalt perception | (Professional) biographical interviews,narratives Document analysis (e.g. diary, files) Participatory observation Video-assisted recall Transcript analysis Analysis in the group |
a) The
The social and biographical background against which problems acquire illness value and the person concerned becomes a patient can best be explained by the person himself and, if necessary, by his significant others (family, friends). For this purpose, I conducted biographical interviews. I gave the interviewees much space for narration and took on the role of an active listener who influenced the narrative flow as little as possible and, if necessary, tried to contribute to clarification and deepening by asking questions. Where the flow of the story got bogged down, I also gave impulses through my own examples in the sense of self-input. In doing so, I also paid attention to the accompanying gestures and facial expressions and, in the sense of Devereux's theorem that countertransference is the most relevant datum of the behavioral sciences (29), I made sure the feelings triggered in me in order to guess what might be going on in the interlocutor. I remember a particularly impressive conversation in which a woman of about 45 years of age talked for several minutes without a break, weighing up the pros and cons of a dilemmatic decision-making situation, while her face showed her being torn back and forth. Suddenly she broke off and abruptly asked me what I thought. I was completely overwhelmed, as I could not and would not decide for her. However, at this moment I now understood that she urgently needed a counterpart and why her GP described the conversations with her as "mirror fencing", in which he felt powerless and at the same time indispensable for the patient. To my relief, I could ascertain that my acknowledgment of her dilemma was sufficient for the interviewee: she had not sought advice but understanding, which was also allowed to express itself in more in-depth questions.
Narrative interviews can also provide access to central experiences in coping with health and illness. For example, they can clarify how patients experience the process of treatment as a whole, what is particularly important to them, how they take up recommendations made by their helpers, how successful this is, and how they interpret this themselves (see e.g. 30).
b) The
When I began my studies on doctor-patient communication, I assumed, in accordance with the prevailing model of Talcott Parsons (31), that patient and doctor encounter each other as role bearers and that the doctor's task was to take appropriate account of the individual characteristics of each patient. After I had presented an interaction analysis at a congress using the means of structural hermeneutics with which I was familiar, a man approached me who bore an astonishing resemblance to the colleague I had presented. Moreover: it was him too - and he commented that his wife, a musician, could undoubtedly have done much with my interpretation. Left unsaid was what he had missed, but I immediately understood that I had objectified him and not taken any notice at all of the terms of his doctoring. We subsequently interpreted some of his conversations together - a cross-professional quality circle emerged from this, and I learned that the doctor also acts in a lifeworld context (32). Another family doctor pronouncedly drew attention to the subjectivity of the doctor as a resource:
"When you observe doctor-patient conversations, the doctor typically remains as a professional and not as a symmetrical partner who brings in his problems. Well, that's what we are taught, and that's what psychotherapists teach us, to use the conversation as an instrument and not as a personal expression of personal concern. I am of a completely different opinion, namely that this is not possible as a family doctor. This psychotherapeutic attitude is not a family doctor's attitude. I am rather of the opinion that we have to deal with our very personal life stories, which the patients also experience! We not only experience the patient's life story, but we also experience our own, so that we also have to be doctors with it." (Family doctor, 50 years)
Accordingly, I have been interested in how one becomes the doctor he or she is and which lifeworld and institutional conditions influence their actions. Biographical interviews have also proved helpful for this purpose (16, 33).
c) Medical world (levels 6,7,9,11-14)
I then approached the (general) medical world through the analysis of video-documented doctor-patient interactions, which dedicated teaching physicians had already produced with the consent of the participants. I was particularly interested in how the different worlds can be mediated in dialogue in such a way that a joint understanding can emerge and the patient can speak of "his family doctor" and the doctor of "his patient" (34). For this purpose, selected interaction sequences were interpreted in detail, partly directly on the video material (video-assisted recall; (35)) and partly additionally based on transcripts. Ideally, this was done in an interdisciplinary group, involving researchers, practitioners from different health care professions, and occasionally patients. Patterns of interaction could be worked out in contrast to possibilities imaginable in thought experiments without yet being realized.
Since the consultations are typically shaped in the context of long-term treatments (14), we extended our analyses and, for example, reconstructed courses of illness and treatment based on information from the medical records. These individual case analyses allowed typifications but no indications of frequencies. I could gain practical epidemiological insights through targeted documentation. I was impressed by a 2-day observation visit, during which conversations were recorded by video, and I could be present in the consulting room. I experienced the challenge of holistically adjusting to very different people every 10 minutes. Furthermore, I got to know the extraordinary willingness of all those involved to support such practical research after the objective had become apparent and the participants had a sense of the researcher. My colleague Vera Kalitzkus was even able to observe during her observation how the consultation hour takes on an overall shape and how earlier ones could influence later conversations even if other patients were involved (36).
In the EUROCOM study (37), we documented consultations in 6 countries by video and evaluated a total of more than 3000 consultations. For this purpose, 190 physicians recorded 20 conversations consecutively by video and documented additional information on the reasons for encounters and diagnoses. The patients answered the same questions through questionnaires and provided insights into their expectations and satisfaction with the consultations. Unfortunately, the extensive data collection was carried out in a division of labor, and the researchers rarely interacted with the "researched". Therefore this limited insight into the contexts.
Moreover, the researchers' relationship-building with the patients and clinicians involved was restricted. While willingness to participate was still high, it was lower than in studies where my colleagues and I had face-to-face contact. However, the statistical analyses did provide information on, among other things, interview duration and workload. Overall, the country- and health system-related differences were remarkable 37). Even more important to us seemed to be the sizeable physician-related variance, which was evident in the style of interviewing and documentation and pointed to the influence of the physician as a subject. In order to be able to examine the interrelationships in an exemplary manner, we prepared case studies in Germany in cooperation with some physicians on issues of particular interest to us, which were later used in the training of medical students (as an example: 38).
d) Multi-perspective view
In the doctor-patient conversation, the life worlds of the participants and the "institutional world" overlap. This consultation, located in the institutional framework, is referred to as a "medical conversation", which is misleading insofar as a co-creative performance takes place to which all interlocutors contribute.
To examine this process, we made multiperspective observations in the project "Health Promoting Practices" (39). Step by step, we retraced how the field of meaning was enriched on a case-related basis. For this purpose, two scientifically accompanied interprofessional quality circles were formed, which explored possibilities of strengthening self-help potentials in patients with chronic diseases using the example of video-documented consultations of the participants. The 30 participants worked in different primary care professions; two were affected patients and represented self-help groups. In almost each of the 50 2-3 hour group meetings, one of the participants presented one of their conversations for discussion and provided supplementary contextual information about the working methods and focus of their practice, their clientele, and the treatment process to date. The conversations were initially discussed as a whole, with group participants drawing different facets of a conversation depending on their qualifications, age, gender, and biographical experiences, which then gradually took on a coherent shape.
Furthermore, there were as many countertransferences offered as participants. These countertransferences referred to the patient's subjectivity and showed possible relationship constellations available to him. In detailed analyses of selected conversation sequences, patterns could then be worked out, in structural hermeneutics (18), for how patient and doctor systematically failed to perceive possible interaction alternatives. The joint analysis aimed at revealing meaningful but unspoken goals. Finally, we considered how to raise the treasure of emerging unused self-help potentials. Each participant thus took away concrete suggestions for treating the patients he or she presented and gained cross-case indications for a more flexible approach to patients with chronic illnesses.
In an interim assessment after one year, it was noted as a shared result that ingrained routines could stand in the way of the perception of specific problem situations and that doctor and patient often talked past each other despite knowing each other well from the "experienced anamnesis". The groups suggested deliberately abandoning the standard procedure to conduct a conversation with their long-term patients as if the participants were meeting for the first time. Instead, the way should be opened for an unprejudiced discussion of the patient's central life and treatment goals by excluding previous knowledge.
This modified procedure was tested in the second year. The video-documented conversations with the patients already presented in the first project year were discussed in the manner described above. As a rule, the patients could use the extended conversation space. The participants thus achieved a new understanding and rated this as enriching and relieving. In individual cases, however, the possible freedom also proved to be threatening, and further need for support became apparent.
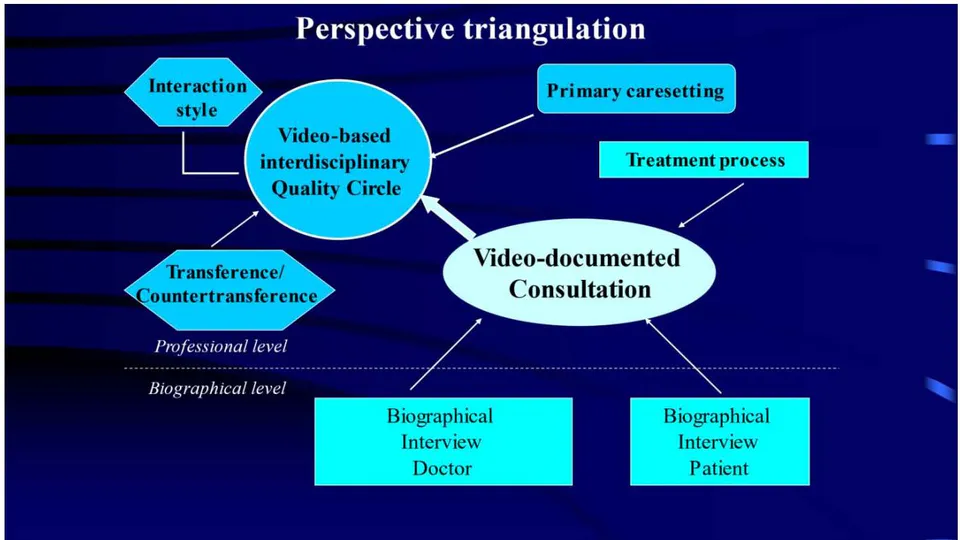
After completing the work phase of the quality circles, we interviewed the primary care providers involved and those patients whose conversations had been discussed and analyzed. Again, we used guideline-supported open and biographically directed interviews so that a multi-layered, multi-perspective view was possible for each "case" (cf. figure).1
We evaluated and modified the jointly developed conversation type of the review dialogue in a follow-up project with other stakeholders (40, 41). However, the approach was similar, so I will refrain from further elaboration here.
With the development of the review interview, I got an idea of answers to the questions that led me to family medicine. Accordingly, as a sociologist initially from outside the field, I could now participate in recommendations for the design of initial interviews in GP practices (42) and promote the fact that the proposal was developed in the unity of research and professional training. The - also biographically based - diversity of competencies thus becomes an opportunity for collaborative learning, and the limit of equal participation depends on the conditions of the division of labor.
Participatory research with people with whom I had come into contact in their role as patients had so far only been possible to a limited extent. In the conversation, I respected their expert status as a matter of course. In individual cases, I obtained and gave feedback on research results in the sense of communicative validation. Increasingly, I involved patients as experts in their own right in the quality circle discussions, and they were involved in the process of generating the results (39). However, I have not yet been able to take the step towards citizen research, in which potentially all participants become researchers. Presumably, this also presupposes that the participants transcend the framework of health care with its strongly differing role offerings and seek common ground in solving questions that affect all participants (45).
e) Where is the researcher as the subject?
In the general understanding, scientificity is equated with objectivity, as if the practically active cognizing subject were unimportant. However, even the choice of topic is value-driven and an expression of interest in knowledge. In continuously developing the topic, a research program characteristic of the person can reveal itself. For example, through a friend, I was allowed to work on a project with people with chronic illnesses - and this world was very familiar to me because I had experienced vital and vulnerable, chronically ill people in my family from birth. In the process, I grew up with a flexible way of dealing with being stigmatized, self-stigmatization, and passive as well as active stigmatization. Thus I approached my counterparts with a pre-concept of salutogenesis, curious about the specific ways in which they were involved and found solutions. This attitude was palpable to my counterparts, whether they were more in the role of help-seeker or helper at the time. However, I addressed my background of experience only occasionally and when explicitly asked. Such questions were rare and mostly came at the end of the conversation. Perhaps one can also say: that with the transgression of the roles we had met, they simultaneously prepared the return to their respective worlds.
Empathy is required of the researcher in health and social care professionals in the data collection phase. Being able to speak out may occasionally also have a quasi-therapeutic effect in the context of research interviews. People do remarkable developmental work and are capable of fundamental self-corrections in a stimulated self-reflection if the interlocutor lets them and, at most, asks follow-up questions that enable further clarification. The same is true in group discussions, in which new perspectives for action are constantly emerging. My turn was to enable autopoietic processes, but not as an advisor. In accompanying the group discussions, I functioned as a representative of the group memory and as the person ultimately responsible for the products that emerged (protocols, case studies, project reports, concept of the review dialogue).
In the texting and reporting, the person of the researcher seems to be erased. Processes congeal into structures, which in the German language becomes clear in passively constructed sentences and in the renunciation of acting subjects. The "I" is replaced by a "man", perhaps also "the scientist". If I do not follow these rules, my scientific community reminds me of them. However, a personal relationship to the research "object" usually develops in a research process that lasts several years. I see this as a specific creative achievement to be made transparent in its development process, not merely a subjective deformation (bias). Thus, in my opinion, Sartre could rightly say about his portrait of Gustave Flaubert that he was not interested in whether the other had been as Sartre described him - what was important was whether Flaubert could have been like that. "I would like my study of Flaubert to be read like a novel because it is the story of an apprenticeship (...). However, I would also like people to take it for the truth when they read it, for a true novel. Throughout the book, it is Flaubert as I imagine him (emphasis mine, O.B.), but since I have methods that seem to me stringent, I also think that it is Flaubert as he is, as he has been." (46)
Wheeler is one of the few to reflect in her excellent doctoral thesis on the particular contribution she made as a clinically untrained sociologist in researching the management of medically unexplained symptoms (MUS) (47). On the one hand, she lacked specific expertise that she could organize for herself by employing support from trained supervisors and drawing on the expertise of practitioners involved in the project. On the other hand, she was freed from seemingly shared self-understanding and could legitimately ask questions that seemed outlandish at first but went further - because they enabled a new framing. Familiar with the subject matter to be researched, also from her own experience, she was able to act as an interpreter between the internal and external viewpoints, developing her terminology in the process. Wheeler reflects excellently on how conceptual presuppositions had a structuring - and in some cases limiting - effect on data collection and analysis and how she was able to correct the limitations partly based on contrasting findings of her own. Finally, she describes a research process that culminates in a condensed result ("bricolage"). The result is a personally formed Gesamtkunstwerk in which the author expresses his or herself with a specific attitude to the world and a characteristic style, which at the same time bears witness to a social practice shaped by many people.
VI. SUMMARY
Our health care system is considered to lack comprehensible orientation. Instead of a fundamental orientation towards enabling health, the defense, administration, and alleviation of illness dominate our actions. The fundamental question should relate to what it is worth to be "healthy" and to what our health-related actions may once have been good.
As for the specific field of action in family medicine, it is tough to convince medical students and graduates of its positive aspects. People often criticize that general practitioners act very differently and that there is a lack of a shared professional self-image. However, there is unanimous agreement that family medicine relates to people in their health and illness, i.e. it is person-centered.
The present paper assumes that a "hermeneutical approach to the case" could create common ground for a more explicit profession-related self-concept. According to the German Society for General and Family Medicine (DEGAM), the hermeneutic understanding of cases is characteristic of general practice. However, there is no operational definition, so this is not part of education and training. The presentation refers to the discussion of "The Patient as Text", which is put up, especially in English-speaking and Scandinavian countries.
Family medicine is relation-based and can be understood as a series of interpretative actions. Thus, family medicine is part of a hermeneutical venture. Consultation is based on a dialogue - not always formulated in language - and thus a co-creative act in which something new can be generated. One of the cases that need to be understood is the doctor himself. Our analysis depicts tacit knowledge in (social and medical) practice based on the individual experiences of those involved and their ancestors. These prior experiences may have settled into routines and institutional rules. Turning tacit knowledge into explicit knowledge would encourage a common ground for a clearer self-concept of family practice both as a practice and as a science. Scientifically accompanied (interdisciplinary) quality circles are suitable for this. They function as further training and research instruments in participatory research and implementation. Quality circles contribute to making hermeneutic case understanding teachable and learnable.
Person-centered medicine - understood as care of persons for persons by persons and with persons - requires that all participants engage as subjects. In this participatory process, traditional roles can and must be redefined. This also concerns researchers.
Regarding my work, I give examples of person-centered research and the difficulties concerning implementing the desiderata of subject-centeredness and participation in institutional contexts.
Health and illness are, at the same time, profoundly personal and social affairs and require a dialogue-mediated self-assurance of the members of society about their central values.
Conflicts of interest: Nothing to declare.
ACKNOWLEDGMENTS
My comments draw on experiences from several medical sociology and general practice projects. I sincerely thank the more than 100 primary care providers and more than 2000 patients involved, without whose trusting support this would not have been possible. I would also like to thank my colleagues of many years standing, with whom I have been able to walk parts of the path together and learn with them. I would like to make special mention of (in alphabetical order) Heinz-Harald Abholz, Martin Beyer, Ralf in der Beek, Atie van den Brink-Muinen, Ferdinand Gerlach, Susanne Heim, Karl-Heinz Henze, Eberhard Hesse, Vera Kalitzkus, Anja Klingenberg, Michael Kohle, Martin Konitzer, Peter Matthiessen, Helmut Muller, Michael Peltenburg, Thomas Ripke, Joachim Szecsenyi, Gernot Ruter, Iris Veit, Peter Verhaak, Stefan Wilm, and Georg Bernhard Wüstenfeld. I owe many suggestions to my advisors (in chronological order) Hannes Friedrich, Jürgen Wilhelm, Eckart Sturm, Wolfram Fischer, Gisela Fischer, and Bruno Hildenbrand.
The studies were partly self-financed and made possible by specific project funding programs. I would like to thank
- The European Commission (Eurocommunication study; BIOMED-II- research pro of the European Commission, contract no BMH4-CT96-1515);
- The AOK Bundesverband (promoting the model project Salutogenetic Orientation in Family Practice - Health Promoting Practices) and
- The Federal Ministry of Education and Research (funding the project Review dialogues to promote patient orientation and improve the quality of primary care treatment for people in chronic conditions (BILANZ); grant number 01GX1030A-C).



