Mammogram screening (MS) is the most effective method for the early detection of breast cancer (BC), yet uptake of MS is low in Saudi Arabia, especially in traditional regions. This cross-sectional study examined 400 women in Aljouf Province in Saudi Arabia from September 2022 to February 2023 regarding BC knowledge, attitudes toward MS, and perceived barriers to participating in MS. Of the women surveyed, 56.3% had low to medium levels of knowledge of BC, which was significantly related to higher education levels and a history of BC in the family. Most notable barriers to participating in MS included fear of BC diagnosis (50.8%), fear of examination procedures, and cultural issues, notably, becoming embarrassed.
## I. INTRODUCTION
Breast cancer (BC) is the leading neoplastic condition of women globally, and in 2022 had almost 2.4 million new diagnoses and 685,000 deaths, the leading cause of cancer-related death in women in 157 out of 185 countries [1]. Morbidity is predominantly important in developed nations where 1 out of 12 women will get BC in her lifetime, though more than $90\%$ survival if detected early [2]. On the other hand, low Human Development Index (HDI) LMICs have incommensurately elevated rates of BC mortality, where 1 woman dies out of 48 due to BC in comparison to 1 woman dying out of 71 in wealthy countries [3]. By 2040, projections anticipate a $40\%$ increase in new BC cases to over 3 million annually, with deaths potentially rising from 685,000 to 1 million, driven by LMICs' population aging, lifestyle changes, and limited access to screening and treatment [1]. Interestingly, over $70\%$ of new BC cases and $81\%$ of deaths occur in women aged over 50, for whom targeted screening among them is therefore vitally necessary [4].
In the Kingdom of Saudi Arabia (KSA), BC is the leading cancer in women, reflecting global trends but augmented by region-specific determinants such as increasing obesity, physical inactivity, and cultural shift towards Westernized lifestyles [5]. The KSA Ministry of Health (MOH) has adopted stringent policies to fight this burden and provides free mammogram screening (MS) to women between 40-50 years every two years and annually or biennially to women between the ages of 51-69 years, with earlier screening advised in women with a family history of BC [6]. Mammography continues to be the gold-standard method for early BC detection, proven to reduce mortality through facilitating timely intervention and reducing treatment costs [7]. Poor uptake of MS has, however, been documented by epidemiological surveys, particularly in conservative regions like Aljouf Province, where modesty and privacy aspects dominate disengagement [8].
MS cultural and psychological barriers are not unique to Saudi Arabia but cross other conservative societies, such as Bangladesh, where 20,000-30,000 new BC cases and 13,000 deaths present annually [9]. In Bangladesh, $80\%$ of patients with BC die due to late presentation, usually by greater than six months' delay, and $70\%$ of presentations involve alternative therapies such as homeopathy before receiving allopathic treatment [9]. These universal obstacles in these environments include shyness, fear of diagnosis, mistrust of the health system, and a culture that prioritizes family responsibilities over individual health [10]. Parallel obstacles-fear of BC diagnosis, shame during investigations, and inadequate communication from the health sector-exist in Saudi Arabia, as do issues of prolonged waiting lists and taking work leave [8,11].
At the international level, awareness of BC mortality is high, with poor knowledge about risk factors and screening, particularly among Asian and African women compared to Western women [12]. For instance, a study conducted in New Delhi, India, reported $50\%$ awareness of BC component among women, with only $7\%$ who had utilized MS, the majority of which was attributed to low socioeconomic status and education levels [13]. In Malaysia, high-risk profiles are seen in only half of eligible women for MS, with higher uptake observed among older women and those counseled by physicians [14]. This emphasizes the role of education, as well as access to healthcare, in enhancing screening rates.
Even though MS is available for free, Saudi Arabia has not started MS use widely, so it is important to find out what is getting in the way and what is misunderstood. This research looks at northern Saudi women aged 40-69 in Aljouf, a place known for its conservatism, and where little is known about how BC is screened. Gathering information about BC risk factors, attitudes toward MS, and perceived barriers is meant to help this study find out what influences low MS use and then suggest targeted actions to deal with them. What we learn from this research can be relevant to other conservative countries like Bangladesh, since they share the same cultural and systemic challenges, supporting global steps to decrease BC risk by applying better screening measures.
## II. METHODOLOGY
### a) Study Design and Setting
From September 2022 to February 2023, the research was carried out throughout Aljouf Province in northern Saudi Arabia. Being one of KSA's conservative provinces, Aljouf provides an advantageous setting to research why women in this region avoid getting mammograms. A cross-sectional design was selected because it provides one instant view of knowledge, attitudes and barriers, making it both affordable and easy to use for creating and checking hypotheses and estimating how common these problems are in the population. It is useful for this study since not many data are available on BC screening routines in Aljouf. The study was limited to Saudi women aged 40-69, matching the MS guidelines from the KSA Ministry of Health (MOH) which prescribe screening in this age group [6]. It was necessary for participants to be Saudi, have access to life in Aljouf, be able to read and write Arabic and willingly give informed consent. To be sure the sample was the same as the community, expatriates, non-residents of Aljouf and women who couldn't complete the questionnaire due to language or reading problems were excluded.
### b) Sampling
We estimated the sample size using Cochran's equation for large populations, a method regularly applied in epidemiological studies to avoid small samples \[16\]:
$$
n _ {0} = \frac {Z ^ {2} p q}{e ^ {2}}
$$
Where:
- $n_0$: Sample size
- Z: Z-score corresponding to the desired confidence level (1.96 for 95% confidence)
- $p$: Estimated proportion of the attribute in the population (set at 0.5 to assume maximum variability, as no prior data on MS uptake in Aljouf were available)
- $q$: (1-p) (0.5)
- e: Margin of error (0.05 for 5%)
To meet these parameters, a minimum of 385 sample participants was needed. This figure was increased to 400 since some people may not respond or finish their questionnaires. Since there is high variation in learning and access to MS in heterogeneous populations, the Cochran formula was chosen [16]. Eligible women were recruited using convenience sampling, which is easy in places such as parks, shopping malls, and mosques. We invited every 10th woman to join the study to aid in diversifying the group by age, education, and socioeconomic status. Those recruited were introduced to the study by trained research assistants with Arabic skills who presented the same information about it.
### c) Data Collection
An approved Arabic-language form, originally developed by Abdel-Salam et al. [8], was employed to gather the data and was checked in a pilot with 30 women from Aljouf. Small changes to explain medical jargon in simpler language were made to fit readers with different educational levels. The three sections of the questionnaire included: (1) sociodemographic factors (age, marital status, education, employment status, income, place of residence and family background with BC); (2) knowledge of BC and MS health education (14 items); and (3) perceived barriers to MS (e.g., fear of cancer, diagnosis, pain, radiation, embarrassment, constraints related to work or family and dissatisfaction with healthcare communication, indicated by 19 statements). An easy-to-understand 5-minute guide on BC, MS, and the objectives of the study was provided to every participant, with trained female assistants on hand to help them answer the 15-20-minute questionnaire without a name.
### d) Data Analysis
All statistical analyses were completed with SPSS version 21, from the IBM Corporation in Armonk, NY, USA. Lots of care was given to the first round of data cleaning, resulting in only $2\%$ of responses on some Likert-scale items needing to be filled in using the mean. Results for frequencies and percentages were reported for all participants' characteristics, knowledge levels and responses. Applying the Shapiro-Wilk test, we found that data lacked normal distribution (with a P-value of less than 0.05), allowing us to proceed with non-parametric statistical analyses.
Spearman correlation test was applied to analyze how learning changes correlate with the perceived recognition and learning barriers scores and rho was used to describe the type and intensity of the correlation. The knowledge scores from the survey were changed to a binary grouping of high and low or medium, to find out what helps people remember the benefits of cervical cancer. The independent variables we used were age, education, marital status, income, residence and if the person had a family history of BC. To overcome confounding, we relied on aORs matched with $95\%$ CIs after correcting for important factors such as education and family history, as noted in the scientific literature [12]. We considered results to be statistically significant when $\mathsf{P} < 0.05$ with two-tailed tests. For this analysis, model fit was confirmed by testing it with the Hosmer-Lemeshow test $(\mathsf{P} > 0.05)$, which stated the model is suitable for fitting the data.
### e) Ethical Considerations
The ethics committee of Qurayyat Health Affairs at the KSA MOH (registration number H-13-S-071) approved the study protocol and confirmed it followed the Declaration of Helsinki [18]. Candidates received a clear explanation of the study's aims, the importance of BC, and what MS tests involve. A written form of informed consent told everyone about their rights, including the right to leave anytime they like. Personally identifiable information was not gathered since all questionnaires were anonymized. All data were kept on password-protected devices that only members of the research team could access. Using women as assistants and interviewing in private, away from family, made it less awkward for participants to talk about birth control.
## III. RESULTS
### a) Participant Characteristics
Two hundred and thirty-three (58.3%) of the 400 women in the survey were between 40 and 49 years old, 351 (87.8%) were married, and 266 (66.5%) had a university-level education. Insufficient income was felt by 237 (59.3%) of the individuals who had less than 7,000 Saudi Riyals monthly (23,874.5 USD annually), and 163 (40.7%) reported monthly earnings of over 7,000 SAR. The majority of participants (341 people or 85.3%) lived in urban areas, and 49 (12.3%) reported having relatives with breast cancer as shown in Figure 1. Among the 400 people, 192 (48.0%) were working, and the rest were unemployed or kept home. Most participants live in urban areas and have at least some educations, yet some rural participants (14.7%) shared information from Second Amendment organizations based in their communities.
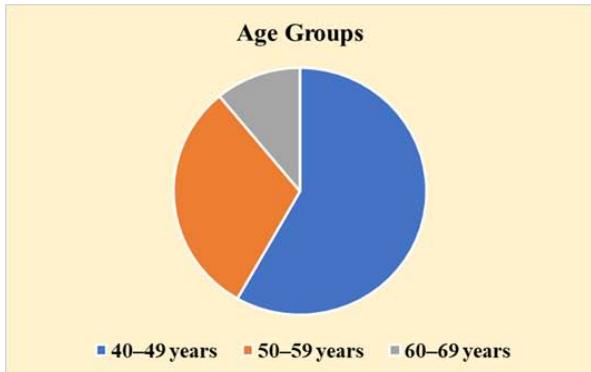
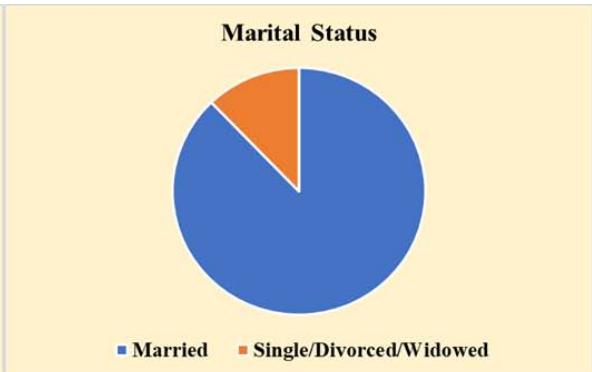
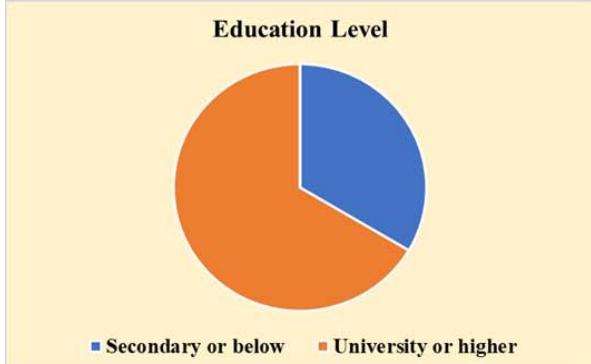

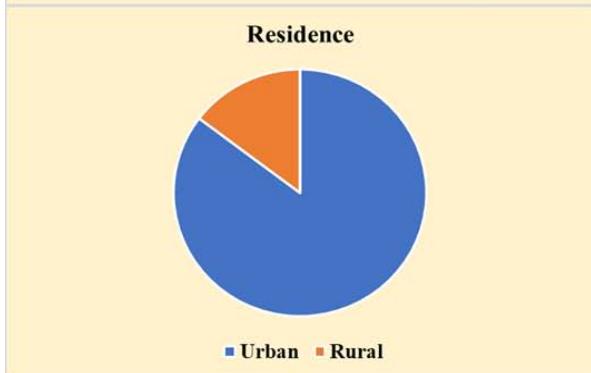
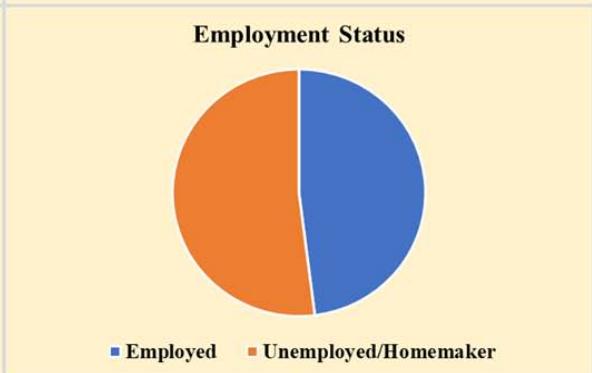
 Figure 1: Sociodemographic Characteristics of Participants (N=400)
### b) Knowledge of BC and MS
MS is the main tool for early BI detection, but only $40.0\%$ realized they could receive free MS as per KSA MOH directions. Using the cut-offs from Bloom's taxonomy, 135 learners $(33.8\%)$ had low knowledge, 90 $(22.5\%)$ had medium knowledge, and 175 $(43.8\%)$ had high knowledge. A total of 225 $(56.3\%)$ had limited knowledge of the subject, which is a substantial gap in this group.
### c) Barriers to MS Uptake
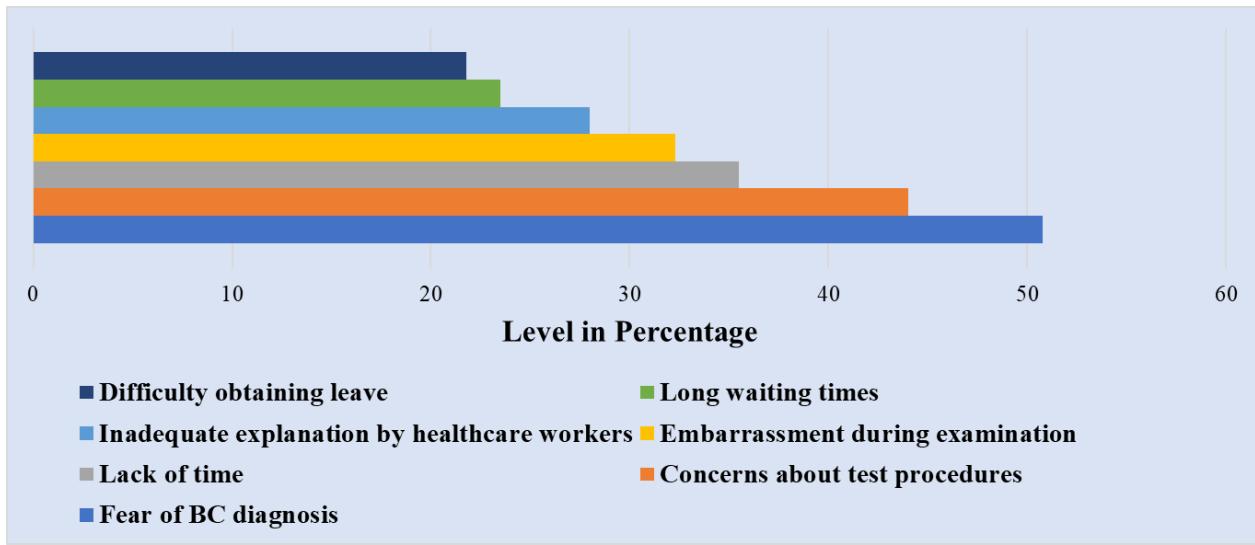
The top three reasons people didn't get MS were fear of BC, worry about what the tests could involve, and not knowing much about MS (203, $50.8\%$; 176, $44.0\%$; 163, $40.8\%$ ). Other serious difficulties for respondents were not enough time (142, $35.5\%$ ), feeling embarrassed during breast exams (129, $32.3\%$ ), poor explanations from medical staff (112, $28.0\%$ ) and logistical hurdles like very long waiting times (94, $23.5\%$ ) and difficulty off from work (87, $21.8\%$ ). Living away from screening services was a bigger problem for rural participants $(54.2\%)$ than urban participants $(18.2\%)$. The totals for barrier scores were classified as being low $(180,45.0\%)$, medium $(136,34.0\%)$, or high $(84,21.0\%)$, with a mean of 19.8 and a standard deviation of 7.2. Figure 1 shows the breakdown of primary obstacles.
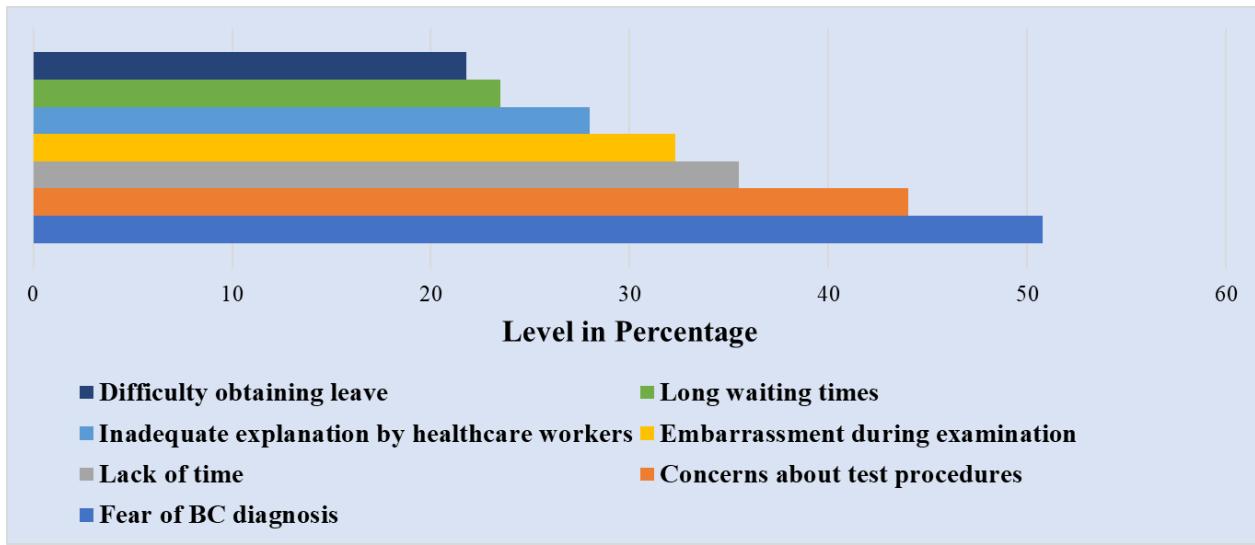 Figure 2: Primary Barriers to Mammogram Screening Uptake
### d) Statistical Associations
Binomial logistic regression modeling found important factors associated with high scores in local knowledge. Those with university-level education had a higher chance (nearly 2.5 times) of high knowledge than those with secondary education or less (aOR 2.35; $95\%$ CI 1.61–3.13; $P = 0.008$ ). BC family history was linked to a 3.66 higher risk among those with good knowledge (aOR, 3.66; $95\%$ CI, 1.94–5.49; $P < 0.001$ ). Age, marital status, income and residence ( $P = 0.214$, $P = 0.387$, $P = 0.162$, $P = 0.091$ ) did not predict whether the disease was present. There was a good match between the model predictions and actual results (Hosmer-Lemeshow test with a P-value of 0.672). It was found that there was a significant negative connection ( $rho = -0.389$, $P < 0.001$ ) between how much people know and how many perceived barriers. The assessment showed rural participants scored lower on knowledge (mean=8.2, SD=2.9) than urban participants did (mean=9.7, SD=3.1) in terms of p-values ( $P = 0.012$ ).
## IV. DISCUSSION
Results of this study show that northern Saudi women report various knowledge gaps and more than half (56.3%) have low to average understanding of BC risk and MS. Better awareness and higher education are strongly related (aOR, 2.35; 95% CI, 1.61–3.13) and this is supported by research from all over the world [11,12]. Specifically, Saeed et al. observed that those Pakistani women with a tertiary education were better informed about BC than women with less schooling [19]. In the same way, having a family history of BC made subjects better informed (aOR, 3.66; 95% CI, 1.94–5.49), possibly from direct exposure to the disease, as also seen by Akhigbe et al. with cases in Nigeria [23]. Knowledge and barriers to screening are negatively correlated (rho $= -0.389$, P\<0.001), implying that women who are knowledgeable about screening see lower barriers, which has been noted in India and Malaysia [14,20].
Most participants stated that avoiding a BC diagnosis because of fear (reported by $50.8\%$ ) mainly showed the strong psychological and cultural concerns that exist in conservative societies. Because modesty and privacy are important in Saudi Arabia, women often find embarrassment when they have to have their breasts examined $(32.3\%)$, as past studies have pointed out (8). In Bangladesh, it is found that $70\%$ of women postpone diagnosis by over three months because of fear, timidity, and cultural beliefs about family duties [9]. Most patients with BC in Bangladesh lose their lives after their cancer has advanced, often because they relied on homeopathy before turning to traditional health services [9]. Test methods (scans and needles) are bothersome, so they refuse to get checked, much as D'almeida et al. found in India, with $57\%$ of women saying the same thing [10]. When healthcare workers do not communicate well enough $(28.0\%)$, global studies point out that spreading clear information encourages individuals to take part in screening [21].
More participants from rural areas had less knowledge and reported higher hurdles like living far from medical services (54.2% of cases) compared to urban participants. This is consistent with what happens globally in LMICs, as rural residents struggle more to obtain healthcare [3]. In comparison, the United Kingdom has a lower rate (82%) because the campaign isn't as strong and screening isn't easily accessible [22]. Based on Saudi Arabia and Bangladesh, it is evident that there is a need for healthcare approaches that fit conservatism and that aim to resolve fears about modesty by providing mobile services and female-led teams.
It is notable that this study had a large enough sample, the size of which was calculated using Cochran's formula and it used a questionnaire that is reliable (Cronbach's alpha=0.82). Being able to estimate numbers of cases is cheap, but the design makes it hard to tell if there is a link between knowledge and barriers. The results for Aljouf might be different in other KSA regions where the culture or socioeconomics are not the same. Biases, for example, remembering events differently or picking volunteers easily available, can skew the study's outcomes. When surveys are held in public, the women studied are usually from cities or can move easily, perhaps leaving out those who live in more remote areas. In the future, both interview-based research and studies including many sites should be used to better understand cultural and psychological barriers in such societies and make the findings general.
It is clear from these findings that special interventions are needed to improve MS uptake. Such interventions should include targeted education, highlight lifestyle risks and stress early screening using culturally appropriate workshops run by female healthcare professionals. Training should help healthcare professionals explain benefits and risks of MS with empathy, reduce worries about discomfort and radiation, and use models known in nations with top MS practices. Increasing access using mobile screening, flexible schedules, easier ways to get there, or screenings at the workplace is very important for those living in rural areas. Program developers should learn from places like Sweden and introduce information campaigns and a unified BC screening process. Moreover, making connections with local leaders and mosques allows highlighting MS and finding solutions that address ways modesty is often seen as a barrier by many communities. Such strategies could also be used in other conservative societies like Bangladesh, as the same barriers stop early detection there. For instance, $70\%$ of BC cases in Bangladesh are detected in private hospitals, and only $5\%$ of the public is aware of mammograms. This underlines that universal BC prevention and health care programs are important in Bangladesh [9].
## V. CONCLUSION
This research shows that both low understanding and tough barriers, for example, fear and related cultural issues, make it harder for northern Saudi women to access MS. The amount of information one knows about BC is mainly influenced by education and family history, and understanding at the HEP level tends to go up as challenges decline. The KSA MOH and health workers should offer appropriate guidance campaigns, strengthen connections, and secure equitable and culturally fitting screening programs for MS. Further mixed-methods studies that cover different areas should be done to understand qualitative barriers that might lead to new national strategies applicable in other conservative societies, such as Bangladesh.
### ACKNOWLEDGMENTS
We acknowledge the contributions the Qurayyat Health Affairs ethics committee and study participants for their support.
Generating HTML Viewer...
References
23 Cites in Article
J Ferlay,M Ervik,F Lam,M Laversanne,M Colombet,L Mery,M Piñeros,A Znaor,I Soerjomataram,F Bray (2025). Global Cancer Observatory: Cancer Today.
Isabelle Soerjomataram,Citadel Cabasag,Aude Bardot,Miranda Fidler-Benaoudia,Adalberto Miranda-Filho,Jacques Ferlay,Donald Parkin,Rama Ranganathan,Marion Piñeros,Ariana Znaor,Les Mery,Yvonne Joko-Fru,Rajesh Dikshit,Rengaswamy Sankaranarayanan,Rajaraman Swaminathan,Freddie Bray (2023). Cancer survival in Africa, central and south America, and Asia (SURVCAN-3): a population-based benchmarking study in 32 countries.
Ahmed Al Zomia,Ibrahim Al Zehefa,Lama Lahiq,Mohammed Mirdad,Abdullah Alshahrani,Turki Alshahrani,Nawaf Almahfuth,Mahmoud Mirdad,Albara Alqarni,Noor Alshareef,Ryan Al Qahtani,Mohammed Asiri,Mohammed Alshahrani,Ramy Ghazy,Ibrahim Tawhari (2024). Tracking the epidemiological trends of female breast cancer in Saudi Arabia since 1990 and forecasting future statistics using global burden of disease data, time-series analysis.
(2024). Breast cancer. Fact Sheets.
Mohammed Abdullah Alzahrani,Ramzi Alzahrani,Abdulaziz Alzahrani,Amal Faraj Hassan,Abdulaziz Alqahtani,Ibrahim Alarifi,Ahmed N Almutairi,Norah A Shayu,Ahmad Omar Taha,Yasir Ayidh Alharbi,Fatimah Howaidi,Mawtah Buayti (2025). Enhancing Symptom Management and Coordination of Breast Cancer Care at Secondary Hospitals in Saudi Arabia.
B Sprague,S Nowak,T Ahern,S Herschorn,P Kaufman,C Odde (2024). Long-term Mammography Screening Trends and Predictors of Return to Screening after the COVID-19 Pandemic: Results from a Statewide Registry.
Reem Alsalamh,Faisal Al-Harbi,Rawan Alotaibi,Omar Al-Harbi,Nada Alshahrani,Saleh Alfadhel,Eyad Fatani,Abdulaziz Al-Harbi,Razan Lasloom,Rayan Alzahrani (2024). Barriers to Breast Cancer Screening in Saudi Arabia: A Systematic Review and Meta-Analysis.
Mohammad Hoq,Shamima Jahan,Md. Mahmud,Md. Hasan,M Jakaria (2024). Breast cancer screening awareness, practice, and perceived barriers: A community‐based cross‐sectional study among women in south‐eastern Bangladesh.
T Kathrikolly,R Shetty,S Nair (2020). Opportunities and Barriers to Breast Cancer Screening in a Rural Community in Coastal Karnataka, India: A Qualitative Analysis.
Zunaira Shoukat,Ali Shah (2023). Breast Cancer Awareness and Associated Factors among Women in Pakistan: A Cross-Sectional Descriptive Study.
Victoria Peacey,Andrew Steptoe,Sigurlína Davídsdóttir,Adriana Baban,Jane Wardle (2006). Low levels of breast cancer risk awareness in young women: An international survey.
S Dey,A Mishra,J Govil,P Dhillon (2015). Breast Cancer Awareness at the Community Level among Women in Delhi, India.
N Abdullah,N Baharudin,M Mohamad,Mohamed-Yassin Ms (2022). Factors Associated with Screening Mammogram Uptake among Women Attending an Urban University Primary Care Clinic in Malaysia.
K Rothman,S Greenland (2008). Modern Epidemiology.
W Cochran (1977). Sampling Techniques.
B Bloom (1956). Taxonomy of Educational Objectives: The Classification of Educational Goals.
(2013). World Medical Association Declaration of Helsinki.
M Rehman,E Tahir,H Hussain,A Khalid,S Taqi,E Meenai (2024). Awareness regarding breast cancer amongst women in Pakistan: A systematic review and meta-analysis.
Angelina Joho,Mwajuma Mdoe,Theresia Masoi,James Yahaya (2024). Perceived barriers and factors influencing uptake of breast cancer screening among women: a population-based cross-sectional study.
Anietie Aliu,Robert Kerrison,Afrodita Marcu (2025). A Systematic Review of Barriers to Breast Cancer Screening, and of Interventions Designed to Increase Participation, Among Women of Black African and Black Caribbean Descent in the UK.
(2025). Summary of national statistics (Eurostat).
Maram Abbas,Mirza Baig (2023). Knowledge and Practice Concerning Breast Cancer Risk Factors and Screening among Females in UAE.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Dr. Kazi Mahmudul Hasan. 2026. \u201cKnowledge, Attitudes, and Barriers to Mammogram Screening Among Northern Saudi Women: A Population-Based Cross-Sectional Study\u201d. Global Journal of Medical Research - K: Interdisciplinary GJMR-K Volume 25 (GJMR Volume 25 Issue K3): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Mammogram screening (MS) is the most effective method for the early detection of breast cancer (BC), yet uptake of MS is low in Saudi Arabia, especially in traditional regions. This cross-sectional study examined 400 women in Aljouf Province in Saudi Arabia from September 2022 to February 2023 regarding BC knowledge, attitudes toward MS, and perceived barriers to participating in MS. Of the women surveyed, 56.3% had low to medium levels of knowledge of BC, which was significantly related to higher education levels and a history of BC in the family. Most notable barriers to participating in MS included fear of BC diagnosis (50.8%), fear of examination procedures, and cultural issues, notably, becoming embarrassed.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.