## I. INTRODUCTION
One of the key features of the National Rural Health Mission (NRHM) is to provide a trained female community health worker i.e., Accredited Social Health Activist (ASHA) to every Indian village (1). An ASHA acts as a bridge between the rural people and the health service outlets, and plays a central role in achieving the national health and population policy goals. An ASHA is expected to provide antenatal, natal and postnatal services to women, give primary medical care (using her kit), assist in the control of diseases with the help of proper information, education and surveillance, counsel people (especially women) on family planning, safe abortion, child immunization, Vitamin A supplementations, appropriate breastfeeding, birth spacing, sex discrimination, child marriage, girls' education, and care of the child (especially newborn), help in household surveys, collaborate with health functionaries working for the community disease control, create awareness on health and its determinants, support the people in utilizing the existing health services etc. (1).
The performance of ASHAs is, therefore, crucial for the success of NRHM.
The objective of this work is to assess the knowledge levels of the ASHAs, with regard to various aspects of maternal and child health, in a rural area of Gomati District, Tripura.
For understanding the knowledge levels of ASHAs, the binomial tests have been done at $5\%$ level of significance.
Before undertaking this study, a brief literature survey has been conducted. However, no study dealing with knowledge evaluation of ASHAs of Gomati District of Tripura, on maternal and child health, has been found.
## II. MATERIALS AND METHODS
It is a cross-sectional study, conducted between April 2017 and July 2017, on 232 ASHAs working in Ompi CHC (Community Health Centre), Killa PHC (Primary Health Centre) and Atharabula PHC. These centres (i.e., two PHCs and one CHC) are located in Ompi RD (Rural Development) Block and Killa RD Block; these two blocks have been selected by the simple random sampling method from the eight RD blocks of the Gomati District of Tripura.
All ASHAs working in the aforesaid centres, during the study period, who have given informed consent regarding participation in this study, have been included; only those ASHAs who are not willing to participate even after knowing the purpose of the study, have been excluded from the study. It may be noted here that, at the very beginning, the purpose and the objective of the study have been clearly discussed with the prospective participants, and they have been given the option to participate or quit at any time.
Data have been collected with the help of a pre-designed, pre-tested and semi-structured questionnaire. ASHAs have been visited on ASHA Varosa Divas of each centre, and interviewed face-to-face using the questionnaire. All the collected data have been tabulated, and utilized to perform binomial tests (2), and the results of the tests have been subsequently interpreted.
The formula (3,4) for calculating the p-value (p1), pertaining to the binomial test, is given in equation-1:
$$
p 1 = 2 (n! / ((n - X)! X!)) p ^ {X} q ^ {(n - X)} \dots 1
$$
where, $n =$ total number of ASHAs participating in the study=232;
$X = n / 2 = 116$
p=proportion of ASHAs who have given correct answer, in response to a question;
q=proportion of ASHAs who have given incorrect answer, in response to the same question.
If $p1 < 0.05$, for a question, then it can be inferred that a significant number of ASHAs have correct knowledge with regard to the topic associated with the question; otherwise, the number of ASHAs, having correct knowledge, is not significant.
The values of $p1$ are calculated for all the questions associated with a particular subject, and subsequently averaged (using the formula for arithmetic mean) to get $p1\min$. If $p1\min < 0.05$, for a subject, then it can be inferred that a significant number of ASHAs have correct knowledge with regard to the particular subject; otherwise, the number of ASHAs, having correct knowledge, is not significant.
If $p < 0.5$ (and consequently, $q > 0.5$ ), then the value of $p1$ may generate erroneous inference regarding significance. Hence, in these cases (where $p < 0.5$ and $q > 0.5$ ), $p$ and $q$ are both taken as 0.5 only for the sake of calculating $p1$.
Since the data have been collected for purely academic purpose, and the permission for data collection has been obtained from the CMOH (Chief Medical Officer of Health) of the Gomati District, and also the MOICs (Medical Officers in Charge) of the respective centres, there is no chance of any kind of exploitation involved in this study.
The necessary research and ethical clearances have been taken from the author's institution.
The method used in this work, is shown in fig.-1.
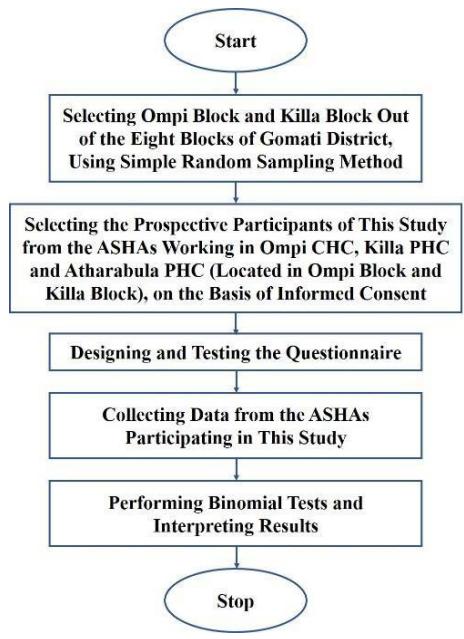 Fig.-1: Flowchart depicting the method
## III. RESULTS
The knowledge levels of ASHAs with regard to antenatal care, postnatal care, breastfeeding, child health, immunization and family planning, are shown respectively in tables- 1-5.
Table-1: Knowledge of ASHAs regarding antenatal care (ANC) (n=232)
<table><tr><td>Serial Number</td><td>Question</td><td>Number of Correct Answers</td><td>Number of Incorrect Answers</td><td>p1</td></tr><tr><td>1.</td><td>What is the optimal time for registration of pregnant women?</td><td>222 (95.7%)</td><td>10 (4.3%)</td><td>0</td></tr><tr><td>2.</td><td>What is the minimum number of ANC check-ups required?</td><td>220 (94.8%)</td><td>12 (5.2%)</td><td>0</td></tr><tr><td>3.</td><td>Is early pregnancy diagnosis to be done by testing urine, stool or blood?</td><td>181 (78.0%)</td><td>51 (22.0%)</td><td>1.1549X10-20</td></tr><tr><td>4.</td><td>What is the purpose of Nischay kit?</td><td>198 (85.3%)</td><td>34 (14.7%)</td><td>1.8090X10-36</td></tr><tr><td>5.</td><td>How many times should the pregnant women (primi) be given tetanus toxoid (TT) injection?</td><td>210 (90.5%)</td><td>22 (9.5%)</td><td>0</td></tr><tr><td>6.</td><td>What is the implication if after blood test, haemoglobin concentration level is found to be less than 7.0 gm/dl?</td><td>168 (72.4%)</td><td>64 (27.6%)</td><td>5.4158X10-13</td></tr><tr><td>7.</td><td>Is there any necessity to give women more food during pregnancy?</td><td>219 (94.4%)</td><td>13 (5.6%)</td><td>0</td></tr><tr><td>8.</td><td>Should women carry out heavy manual labour during pregnancy?</td><td>102 (44.0%)
116 (50.0%) (for calculating p1)</td><td>130 (56.0%)
116 (50.0%) (for calculating p1)</td><td>0.1046</td></tr><tr><td>9.</td><td>What is the minimum period for which all pregnant women must take IFA (iron and folic acid) tablet (1 tablet daily) to prevent anaemia?</td><td>139 (59.9%)</td><td>93 (40.1%)</td><td>1.0111X10-3</td></tr><tr><td>10.</td><td>What are the side effects of IFA tablet?</td><td>151 (65.1%)</td><td>81 (34.9%)</td><td>1.5910X10-6</td></tr><tr><td>11.</td><td>What are the potential danger signs during pregnancy which prompt immediate referral?</td><td>196 (84.5%)</td><td>36 (15.5%)</td><td>2.8340X10-34</td></tr><tr><td>12.</td><td>Is it the duty of an ASHA to escort the pregnant women to the hospital for institutional delivery?</td><td>229 (98.7%)</td><td>3 (1.3%)</td><td>0</td></tr><tr><td>13.</td><td>What should an ASHA do if, after home delivery, mother reports excessive vaginal bleeding or severe abdominal pain?</td><td>151 (65.1%)</td><td>81 (34.9%)</td><td>1.5910X10-6</td></tr><tr><td>14.</td><td>What is the meaning of birth-preparedness?</td><td>178 (76.7%)</td><td>54 (23.3%)</td><td>1.2826X10-18</td></tr></table>
Table-2: Knowledge of ASHAs regarding postnatal care (PNC) $(n = 232)$
<table><tr><td>Serial Number</td><td>Question</td><td>Number of Correct Answers</td><td>Number of Incorrect Answers</td><td>p1</td></tr><tr><td>1.</td><td>What is the meaning of postnatal period?</td><td>138 (59.5%)</td><td>94 (40.5%)</td><td>1.4699×10-3</td></tr><tr><td rowspan="2">2.</td><td rowspan="2">What is the minimum number of postnatal check-ups required?</td><td>99 (42.7%)</td><td>133 (57.3%)</td><td rowspan="2">0.1046</td></tr><tr><td>116 (50.0%) (for calculating p1)</td><td>116 (50.0%) (for calculating p1)</td></tr><tr><td>3.</td><td>What are the common major complications which can happen during the postpartum period?</td><td>193 (83.2%)</td><td>39 (16.8%)</td><td>5.3545×10-31</td></tr><tr><td>4.</td><td>What should be the minimum spacing between two live child births?</td><td>213 (91.8%)</td><td>19 (8.2%)</td><td>0</td></tr><tr><td>5.</td><td>Which women are more at the risk of developing complications during delivery?</td><td>158 (68.1%)</td><td>74 (31.9%)</td><td>8.7765×10-9</td></tr><tr><td>6.</td><td>What is the time interval following delivery, after which the placenta usually comes out?</td><td>171 (73.7%)</td><td>61 (26.3%)</td><td>1.5836×10-14</td></tr></table>
Table-3: Knowledge of ASHAs regarding breastfeeding (n=232)
<table><tr><td>Serial Number</td><td>Question</td><td>Number of Correct Answers</td><td>Number of Incorrect Answers</td><td>p1</td></tr><tr><td>1.</td><td>Why is colostrum necessary for a newborn baby?</td><td>206 (88.8%)</td><td>26 (11.2%)</td><td>0</td></tr><tr><td>2.</td><td>When should a newborn be put to breast, after birth?</td><td>221 (95.3%)</td><td>11 (4.7%)</td><td>0</td></tr><tr><td>3.</td><td>At least how many times should a newborn be breastfed per day?</td><td>195 (84.1%)</td><td>37 (15.9%)</td><td>3.1401X10-33</td></tr><tr><td>4.</td><td>What are the indications of inadequate breastfeeding to a baby?</td><td>170 (73.3%)</td><td>62 (26.7%)</td><td>4.8518X10-14</td></tr><tr><td>5.</td><td>What should be the duration of exclusive breastfeeding, according to WHO (World Health Organization)?</td><td>210 (90.5%)</td><td>22 (9.5%)</td><td>0</td></tr><tr><td>6.</td><td>What is the age at which, complementary food is necessary for a baby?</td><td>225 (97.0%)</td><td>7 (3.0%)</td><td>0</td></tr></table>
Table-4: Knowledge of ASHAs regarding child health (n=232)
<table><tr><td>Serial Number</td><td>Question</td><td>Number of Correct Answers</td><td>Number of Incorrect Answers</td><td>p1</td></tr><tr><td>1.</td><td>What is the minimum body weight of a normal baby at birth?</td><td>226 (97.4%)</td><td>6 (2.6%)</td><td>0</td></tr><tr><td>2.</td><td>When should a baby be considered to have low birthweight (LBW)?</td><td>128 (55.2%)</td><td>104 (44.8%)</td><td>0.0296</td></tr><tr><td>3.</td><td>What are the signs of a high risk baby?</td><td>148 (63.8%)</td><td>84 (36.2%)</td><td>1.0664X10^5</td></tr><tr><td>4.</td><td>What are the signs/symptoms due to which, an ASHA should advise the mother/family to take a baby to the hospital immediately?</td><td>182 (78.4%)</td><td>50 (21.6%)</td><td>2.4879X10^21</td></tr><tr><td>5.</td><td>What are the signs/symptoms which indicate severe dehydration of a baby in case of diarrhoeal disease?</td><td>183 (78.9%)</td><td>49 (21.1%)</td><td>3.4374X10^-22</td></tr><tr><td>6.</td><td>Should a baby be given bath immediately after birth?</td><td>203 (87.5%)</td><td>29 (12.5%)</td><td>0</td></tr><tr><td>7.</td><td>When can the body temperature of a newborn baby be considered as less than normal?</td><td>190 (81.9%)</td><td>42 (18.1%)</td><td>4.8999X10^-28</td></tr><tr><td>8.</td><td>How many times should an ASHA undertake home visit, in case of institutional delivery?</td><td>186 (80.2%)</td><td>46 (19.8%)</td><td>1.4319X10^-24</td></tr><tr><td>9.</td><td>How many times should an ASHA undertake home visit, in case of home delivery?</td><td>205 (88.4%)</td><td>27 (11.6%)</td><td>0</td></tr></table>
Table-5: Knowledge of ASHAs regarding immunization and family planning (n=232)
<table><tr><td>Serial Number</td><td>Question</td><td>Number of Correct Answers</td><td>Number of Incorrect Answers</td><td>p1</td></tr><tr><td>1.</td><td>What are the disease/diseases against which BCG (Bacillus Calmette-Guérin) vaccine provides protection?</td><td>225 (97.0%)</td><td>7 (3.0%)</td><td>0</td></tr><tr><td>2.</td><td>What are the disease/diseases against which DPT* vaccine provides protection?</td><td>192 (82.8%)</td><td>40 (17.2%)</td><td>4.6920X10-30</td></tr><tr><td>3.</td><td>What is the minimum interval between two doses of Vitamin A?</td><td>182 (78.4%)</td><td>50 (21.6%)</td><td>2.4879X10-21</td></tr><tr><td rowspan="2">4.</td><td rowspan="2">Up to what time interval after pregnancy, is abortion legal?</td><td>108 (46.6%)</td><td>124 (53.4%)</td><td rowspan="2">0.1046</td></tr><tr><td>116 (50.0%) (for calculating p1)</td><td>116 (50.0%) (for calculating p1)</td></tr><tr><td>5.</td><td>What is a condom (nirodh)?</td><td>129 (55.6%)</td><td>103 (44.4%)</td><td>0.0242</td></tr><tr><td rowspan="2">6.</td><td rowspan="2">What is an oral contraceptive pill (OCP)?</td><td>92 (39.7%)</td><td>140 (60.3%)</td><td rowspan="2">0.1046</td></tr><tr><td>116 (50.0%) (for calculating p1)</td><td>116 (50.0%) (for calculating p1)</td></tr><tr><td>7.</td><td>What are the ways through which HIV (human immunodeficiency virus) can pass from one person to other persons?</td><td>151 (65.1%)</td><td>81 (34.9%)</td><td>1.5910X10-6</td></tr></table>
For table-5, p1min=0.033. Hence, it may be concluded that a significant number of ASHAs (66.5%) have correct knowledge regarding immunization and family planning.
At the end of each table, the percentage for the significant number of ASHAs has been calculated by averaging the percentages corresponding to the number of correct answers, in the corresponding table.
The values of p1 in tables- 1-5 show that a significant number of ASHAs have correct knowledge regarding the topic associated with each of the questions, except question number-8 of table-1, question number-2 of table-2, and question numbers-4 and 6 of table-5.
## IV. DISCUSSIONS
From tables- 1-5, the following inferences can be drawn:
- A significant number of ASHAs (working in the aforesaid centres) have correct knowledge with regard to various aspects of the subjects of antenatal care (78.9%), postnatal care (69.8%), breastfeeding (88.2%), child health (79.1%), immunization and family planning (66.5%).
- A significant number of ASHAs do not have correct knowledge on each of the following topics: (a) whether women should carry out heavy manual labour during pregnancy $(56.0\%)$, (b) the minimum number of postnatal check-ups required $(57.3\%)$, (c) the time interval after pregnancy, up to which abortion is legal $(53.4\%)$, and (d) what an oral contraceptive pill (OCP) is $(60.3\%)$.
- All ASHAs should have correct knowledge about all aspects of all of the aforesaid subjects (viz., antenatal care, postnatal care, breastfeeding, child health, immunization and family planning). But, the situation is quite far from the reality. Hence, there is no room for complacency, and immediate arrangements should be made for proper and adequate training of the ASHAs, particularly with regard to the four aforesaid topics, pertaining to each of which, a significant number of ASHAs do not have correct knowledge.
Now, a brief review of the outcomes of some of the other studies on ASHAs, may help in understanding the relevance of this work.
A study undertaken by Garg et al. shows that in some villages of rural Haryana, majority of ASHAs knew about assisting in immunization (100%), accompanying women for delivery (98%), and providing antenatal care (96.10%) and family planning (96.40%) services, as a part of their duty (5). In the current study also, it has been found that a significant number of ASHAs have thorough knowledge about antenatal care (78.9%), immunization and family planning (66.5%).
Fathima et al. conducted a survey on ASHAs of some parts of Karnataka, and found that a significant number of ASHAs $(>80\%)$ were involved in home visits, and counselling with regard to antenatal care, breastfeeding and immunization, but only a small proportion $(<25\%)$ of ASHAs gave advice on the use of contraceptives (6). These observations, except the one concerning contraceptives, are similar to those of the current study, where it has been found that a considerable number of ASHAs have good knowledge about antenatal care $(78.9\%)$, breastfeeding $(88.2\%)$, immunization and family planning $(66.5\%)$. However, in the present study, $55.6\%$ of the ASHAs know what a condom (nirodh) is (though only $39.7\%$ of them know what an oral contraceptive pill (OCP) is).
Guha et al. worked on the ASHAs of some villages of Maharashtra (Wardha), and observed that though majority of the ASHAs undertook home visits and assisted in antenatal care and postnatal care, only a few of them were aware of their roles in facilitating breastfeeding and the use of contraceptives (7). Regarding antenatal care and postnatal care, their findings are similar to those of the present study which indicates good knowledge among significant number of ASHAs about antenatal care (78.9%) and postnatal care (69.8%). But, unlike their observations about breastfeeding and contraceptives, the present study indicates that a considerable number of ASHAs are knowledgeable about breastfeeding (88.2%) and condom (nirodh) (55.6%). (However, according to the current study, only 39.7% of the ASHAs know what an oral contraceptive pill (OCP) is.)
Taksande et al. studied the ASHAs of selected villages of Maharashtra (Wardha), and found that $48\%$ of them were aware of the antenatal care registration in clinic (8). This outcome is not quite in agreement with the finding of the current study that $78.9\%$ of the ASHAs have good knowledge about antenatal care.
Panda et al. undertook a study on ASHAs working in some parts of Odisha, and found that $100\%$ of the ASHAs helped in immunization, and $98\%$ of them knew about family planning activities (9). Their observations are similar to that of the current study that majority of the ASHAs $(66.5\%)$ have correct knowledge about immunization and family planning.
Sugandha et al., after conducting a study on the ASHAs of Mysuru (Karnataka), noted that $51.5\%$ of them had average knowledge about antenatal care, $86.1\%$ had good knowledge regarding postnatal care, and $90.5\%$ had thorough knowledge about contraception (10). With regard to postnatal care and contraception, there are similarities between their outcomes and those of the current study, since the present study indicates correct knowledge, among significant number of ASHAs, in the fields of postnatal care $(69.8\%)$, immunization and family planning $(66.5\%)$. However, in contrast to their observation about antenatal care, the current study shows that a considerable number of ASHAs (78.9%) have good knowledge about antenatal care.
Chaurasiya et al., after analyzing relevant information regarding the services provided by the ASHAs, collected from their beneficiaries (i.e., mothers having child up to 2 years of age), in some villages of a district of western Uttar Pradesh, observed that ASHAs escorted $43.5\%$ of the beneficiaries $\geq 4$ times to the hospital/health centre for antenatal care visit, and performed $\geq 6$ home visits for postnatal care for $57.2\%$ of the beneficiaries (11). These observations indicate that majority of the ASHAs have good knowledge about postnatal care, but not antenatal care. However, in the present study, significant number of ASHAs have been found to have thorough knowledge regarding both antenatal care $(78.9\%)$ and postnatal care $(69.8\%)$.
Bhattacharya et al. worked on how the pregnant women utilized services of the ASHAs in some villages of the West Tripura District of Tripura, and found that the ASHAs helped $76.69\%$ of the women to have adequate antenatal check-ups (12). This finding indicates that majority of the ASHAs have good knowledge about antenatal care, and hence, is similar to the outcome of the current study that $78.9\%$ of the ASHAs have thorough knowledge about antenatal care.
## V. CONCLUSIONS
The work has attempted to assess the knowledge levels of the ASHAs, with regard to various aspects of maternal and child health, in a rural area of Gomati District, Tripura. On the basis of the results of the binomial tests, it can be concluded that a significant number of ASHAs, associated with Ompi CHC, Killa PHC and Atharabula PHC, have correct knowledge regarding various aspects of the subjects of antenatal care, postnatal care, breastfeeding, child health, immunization and family planning, except certain topics viz., heavy manual labour by women during pregnancy, minimum number of postnatal check-ups, time-limit of abortion after pregnancy, and oral contraceptive pill (OCP). However, since all ASHAs need to become aware of all the relevant details with respect to the aforesaid subjects, there is an urgent need for proper and adequate training of the ASHAs, especially with regard to the four abovementioned topics.
A more comprehensive idea about the ASHAs of Tripura could have been had, if data were collected from other districts also. Besides, a more detailed questionnaire might have been helpful in judging the ASHAs' knowledge levels regarding various aspects of maternal and child health, to a greater degree. If possible, these tasks may be taken up in future.
### ACKNOWLEDGEMENTS
The author is deeply indebted to Dr. Shantanu Jamatia, PGDPHM student (session: 2016-17), AliH & PH, Kolkata, for collecting the data and helping in the analysis.
Besides, the author is grateful to the ASHAs (who have participated in this study) associated with Ompi CHC, Killa PHC and Atharabula PHC, for their cooperation in the data collection process.
Source of Funding: Personal Source
Conflict of Interest: The author certifies that there is no conflict of interest, involved in this study.
Generating HTML Viewer...
References
13 Cites in Article
Rajat Khanna (2021). Contribution of Accredited Social Health Activist (ASHA) under the Community Health Model of National Health Mission, India.
(2022). Binomial Distribution.
S Mitra,B Chakraborty (2020). A Study on the Socio-Demographic and the Clinical Profiles, Along with Some Management Indicators, of the MDR TB Patients at the Domjur Block, Howrah District, West Bengal, India.
S (2). Available from.
R Van Den Berg (2022). Binomial Test -Simple Tutorial.
P Garg,A Bhardwaj,A Singh,S Ahluwalia (2013). An Evaluation of ASHA Worker's Awareness and Practice of Their Responsibilities in Rural Haryana.
F Fathima,M Raju,K Varadharajan,A Krishnamurthy,S Anathkumar,P Mony (2015). Assessment of 'Accredited Social Health Activists'-A National Community Health Volunteer Scheme in Karnataka State, India.
Ishita Guha,Abhishek Raut,Chetna Maliye,Ashok Mehendale,Bishan Garg (2018). Qualitative Assessment of Accredited Social Health Activists (ASHA) Regarding their roles and responsibilities and factors influencing their performance in selected villages of Wardha.
Vaishali Taksande,Priyanka Ashtankar,Chetna Bansod,Ashwini Bawane,Pratiksha Burchunde,Diksha Dudhe,Madhavi Gawande (2021). To Assess the Job-Related Difficulties and Dissatisfaction of Asha Workers in Selected Rural Area.
Mayadhar Panda,Sikata Nanda,Rama Giri (2019). A study on the work profile of ASHA workers in a district of Odisha in eastern India.
B Sugandha,P Jagannath (2019). Knowledge of ASHA Workers About Maternal and Child Health Services in Mysuru.
S Chaurasiya,N Singh,S Shukla,P Bajpai,D Mathew (2020). Assessment of the Services of ASHA Workers on Antenatal and Postnatal Care in a District of Western Uttar Pradesh, India.
Himadri Bhattacharya,Nimaichand Luwang,Mousumi Sarkar,Tanusree Chakraborty,Subrata Baidya (2015). Utilization of ASHA services by the pregnant women of rural Tripura, India.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Dr. Sampa Mitra. 2026. \u201cKnowledge Evaluation of Accredited Social Health Activists (Ashas) on Maternal and Child Health, in a Rural Area of Gomati District, Tripura\u201d. Global Journal of Medical Research - K: Interdisciplinary GJMR-K Volume 22 (GJMR Volume 22 Issue K6).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































