


I. INTRODUCTION
Incessant sudden power failures at Nigerian and other LMIC healthcare facilities, especially the special care baby units (SCBU) of the tertiary hospitals, are endemic and this has been associated with high mortality rates in the countries[1 - 4]. The failures lead to abrupt cessation of the operation of all life-support devices from which many patients had died. However, this contributor to the causes of death is not usually reported in the associated end-of-life file documents. This kind of situation where technology failure becomes a significant contributor to the cause-of-death has been described as a powerful mortality factor that are hardly reported in a deceased-patient's file in Nigeria, but dwells only in the minds of practicing doctors and nurses who continually witness this[5]. Apart from the immediate impact on patients who are directly under machine support, there are many other patients and carers who could have been injured, especially at night owing to the sudden unexpected darkness that engulfs the environment. This includes accidents such as patients being given the wrong medication, duty staff bumping into each other and hitting themselves against harmful stationary items around the SCBU and the walkways, costly errors on patients whilst neonatal line-setting procedure is being performed, etc. Total facility light blackouts, though common in Nigeria, has such a demoralising effect on the clinical and nursing team as they struggle to carry on with makeshift handheld mobile lamps such as mobile-phone torchlight. There may not be any empirical quantification of Nigeria's annual death rate associated with poor facility lighting; however, this might present a terrifying figure if computed.
Observably, staff on duty tend to exhibit some levels of reluctance whenever the clinical need arises to stay longer at work during such night periods with blackouts. Many publications have emphasised the need for Nigeria's power sector to improve its power supply reliability, but this has not yielded any result [1, 2, 6]. Therefore, there is an urgent need to create a suitable alternative for a reliable lighting technology for tertiary hospital neonatal centres other than the present quality of grid electricity in Nigeria and other similar LMICs. This worrisome lighting situation is happening at centres in big LMICs cities; hence, the more precarious situations at rural towns can only be dreadfully imagined. This clearly explains one of the fundamental reasons why many rural hospitals are characteristically unable to provide adequate survival support to prevent the deaths of nearby neonates. The recent proposal and demonstration of the neonatal-rescue-scheme (NRS) of Amadi et al. (2022), which revolves around the concept of reversing the neonatal traffic, by "taking our medicine to the needy neonates where they are", will be impossible to achieve at LMICs without decisive independent and locally sustainable lighting solution [7]. Such a system should be low-cost to install, have reliable frugal technology, and with minimal maintenance requirements. In this article, we describe the materials selection, trialling, and four years usage outcome of an LMICs-facility lighting solution-the Polite Light Bank (PLB) system, an aspect of the NRS technologies- currently in use at five neonatal facilities in Nigeria.
II. MATERIALS AND METHODS
The set objectives of the project were defined to include but are not limited to: (a) to make the new system an independent installation from any existing powerbank backup system that supplies the sockets for powering the incubators and other essential equipment in the Unit. (b) the system should be operated on low dc power with artificial intelligence to know when there is sufficient daylight or conventional electric power to enable its automatic switching (ON/OFF) as necessary. (c) the system's total power storage should be sufficient to support all light-points throughout the dark periods of the night and cloudy day. (c) the system should sufficiently rely on solar panels for the recharging of its batteries so that it could be reliable as the only source of lighting a facility in a typical remote village of Nigeria without grid electricity.(d) the light-points should be as maintenance free as possible with high reliability and great illumination intensity. (e) the illumination intensity of each light-point should be powerful enough to enable a staff team to carry out neonatal 'line-setting' procedure at night-time without the need for extra lighting support. (f) the battery storage requirement should be easily sourced locally within the nearest urban town market to avoid prolonged downtime when a replacement is needed.
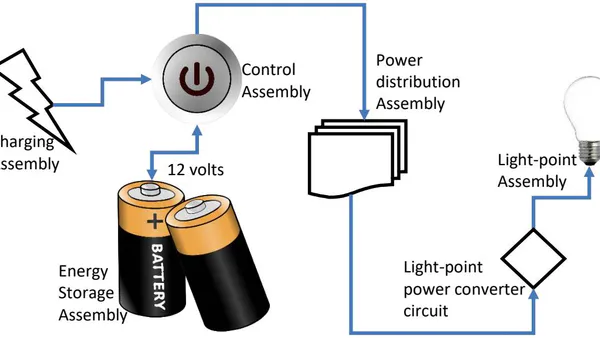
A concept was designed in which four constituent assemblies of the proposed system were identified (Figure 1). A choice of creating outright fresh designs of these assemblies to the highest standards as required could take many years to accomplish, too sophisticated, too expensive, and may not yield the desired accuracy and quality. Therefore, the commercial products morphing and grouping technique, as described previously in the literature, was adopted to create each assembly as close as possible to desired high standards [8].
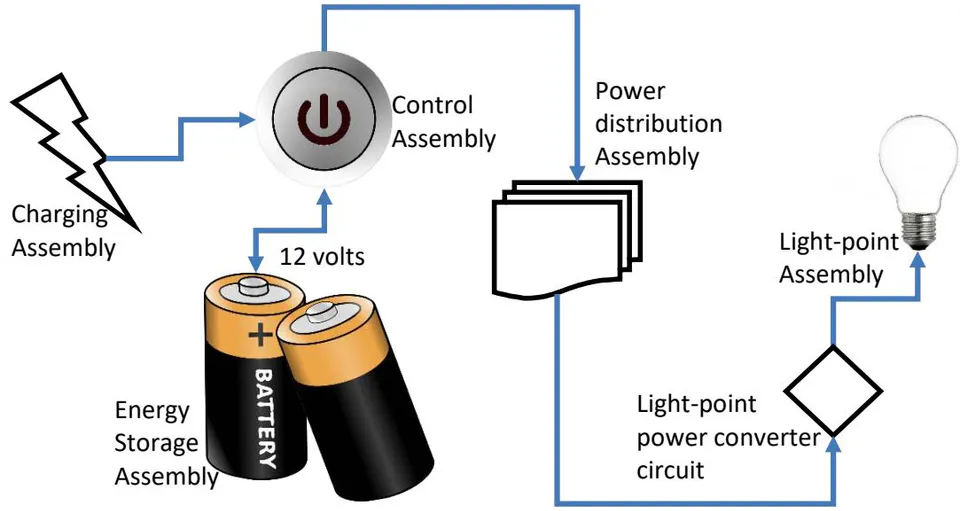
Material selection for building the Charging Assembly was based on tested reliability of locally available (within the Nigerian upstream market) solar panels with ratings of 12 volts, 170 watts photo-voltaic cells, all assembled in parallel with the aim of delivering up to 12 volts, 15 amperes of charging current to the control assembly during the peak of sunlight intensity. The capacity of the energy Storage Assembly was determined by the total number of the light-points to be installed as adjusted by any possible voltage drops along the distribution line assembly. The storage capacity, in turn, is applied to determine the number of required panels of the Charging Assembly to guarantee sources shine around it. This addition enhanced the system's automatic switching capability. The 12 volts DC Distribution Assembly used a parallel cabling technique applying pure copper cables to supply each light-point. The light-point was designed by obtaining four different types of regularly available LED chips assemblies, with a minimum intensity rating of 1000 lumens. These were experimentally tested for efficiency, durability, and weathering by exteriorly mounting and continuously powering these in a typical Nigerian village under rain and sunshine for eight months. The best of the light-point products was chosen and re-morphed to operate via the designed distribution assembly of the polite-light-bank. The initial steps of the morphing technique involved the disassembling of the commercial light-point to study its circuitry, carrying out tests, and taking note of its absolute powering voltage and power consumption rate. The outcomes were later applied in the design of a new power-converter circuit for the re-morphed light-point. Hence, the re-morphing was carried out in two steps - powering circuit re-engineering and structural encasement re-engineering.
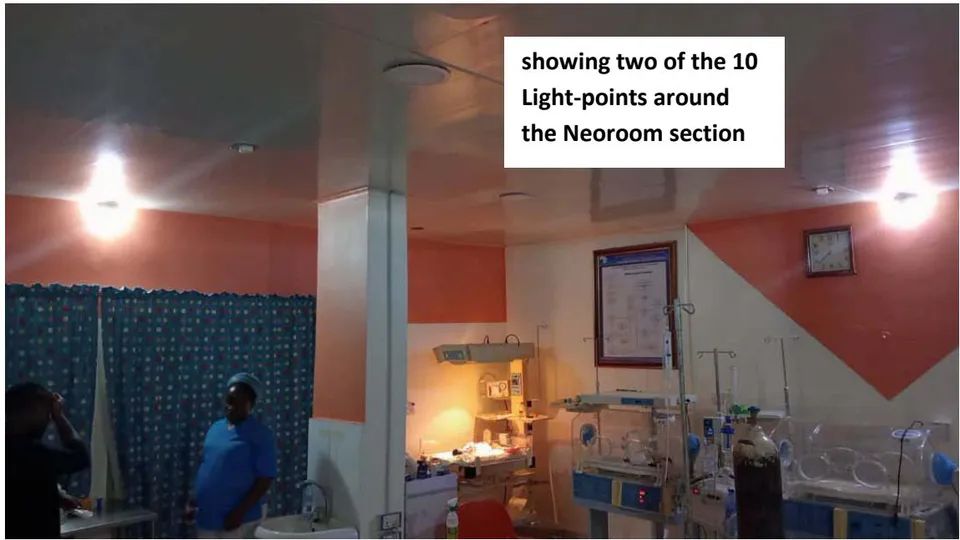
These were carefully executed to ensure minimal alteration of its original aesthetic values. The final product was replicated for powering a PLB system capacity of 19 light-points at the neonatal section of General Hospital Minna, Nigeria (the Amina-centre) in 2019, distributed across with a total two-core cabling length of about 560 metres. A few other centres later heard about the PLB at Minna. They decided to install the PLB as well, including the Federal Medical Centre Owerri with 24 light-points and the Neoroom-section at Calabar Women and Children Hospital (CWCH) with 10 light-points [9, 10]. Final qualitative assessments were independently presented by one major referral centre in northern Nigeria and one Neoroom (miniaturised neonatal centre) in southern Nigeria as these were the only centres that demonstrated their prospective log notes to qualify for assessment submission (Figure 2). Each hospital carried out their assessment via a questionnaire and led by the Ward-manager of the Centres - Matron M Usman and Mr G Adim, respectively.
III. RESULTS/DISCUSSION
System performance assessment at two centres (Amina-centre Minna and CWCH Calabar) was prospectively carried out by capturing the inclusive periods of PLB switch-on and switch-off for 44 and five months, respectively, until the end of March 2023 (Table 1). Illumination performance and practice impacts were qualitatively assessed against the benchmark of ease of carrying out neonatal line-setting procedures without requiring additional or brighter light as duty demanded. The CWCH Neoroom, in their qualitative report, declared that the use of their new PLB-technology currently saves
of their usual operational costs per neonate. This being the proportion of the treatment charge per neonate, which went into fusil fuel and maintenance costs of the power-generator whenever a neonate was on admission. This amount is saved in addition to the elimination of long hours of noise and air pollution of the environment by the power generator, the report continued: "therefore, the staff of this Neoroom are conscious of our high score ratings for our PLB because the system is just as we have assessed it based on our five months' usage experience".
| S/N | Criteria (Score: 0% - 100%) | Details of criteria and Scoring benchmarks | The Amina-centre, General Hospital Minna | The Neoroom, Calabar Women and Children Hospital | |
| 1 | Usage till date | How long has the centre been using the PLB till date? | 3 years and 8 months | 5 months | |
| 2 | Lighting coverage | The walkways | By how much satisfaction does the PLB illumination sufficiently cover walking around safely without need of extra lighting? No illumination (0%) - extremely sufficient (100%) | 100 | 100 |
| Inner wards/SCBU | 100 | 100 | |||
| 3 | By what amount has anxiety over lighting failure dropped? | You know how worried you can get as the ward manager when you have a patient, but there is a grid power failure and no fuel to run the generator. The PLB must have removed some of the worries you normally faced in such situations, such as possible accidents whilst walking around or patient care mistakes whilst working in the dark. By how much has the PLB relieved you of this worry? [still as anxious as ever (0%) - completely relieved of this anxiety (100%)] | 100 | 100 | |
| 4 | Light-point intensity for work | What is the satisfaction rate for PLB light-point intensity for carrying out high precision procedures such as neonatal line-setting? | 90 | 100 | |
| 5 | All night lighting coverage | During all night blackout, what percentage of the night (dusk-to-dawn) does your PLB retain its full illumination?[Goes off <1 hr after (0%) - lasts till daybreak without failure (100%)] | 100 | 100 | |
| 6 | System automatic control | The PLB is completely self-operating. What is your satisfaction rate for the efficiency of this automation?[Manual support needed always (0%) - never ever had cause for manual control(100%)] | 100 | 100 | |
| 7 | System reliability | What is your fair score on the reliability of the PLB? | 100 | 100 | |
| 8 | Light-point failures since installation | Based on the total light-points of your PLB, how many of these have ever failed to come on as at when expected since installation? | 1 out of 19. This happened after 3 years of usage | none out of 10 | |
| 9 | Overall satisfaction | What is your overall satisfaction of your night lighting problem as solved by the PLB till date? | 99 | 97 | |
| 10 | Comments and Concerns | CWCH: (a) wished for PLB extended to cover the laboratory section and save further power cost (b) wished for light-points installed in two other important rooms of the Unit. Amina-centre: wished for PLB light-points installed in additional four rooms at the Centre. | |||
The strategy of developing a low-cost rural healthcare lighting system for keeping neonatal facility illuminated during the night with high intensity lightpoints was set to achieve some primary objectives, which initially seemed impossible. This challenge emanated from the pressure experienced at the neonatal intensive care section of the Minna General Hospital Nigeria (the Amina-centre), where we discovered that the installed 2400 AH storage capacity inverter-controlled power-bank was being drained in quick time by the conventional 220 volts, 9 watts light bulbs that were linked to this. The essential life-support gadgets such as the incubators would hence poweroff in quick time because of the 'battery-low' inverter warning and switch off. The power off often happened some midway into the night during prolonged night blackouts. However, the battery energy could last up to three times longer than this whenever the 220 volts light bulbs were disconnected. Hence, it became necessary to seek to develop an independent system for lighting the facility only – and free from supplying power to the sockets, such that this could supply maximum illumination for all night long around and within the neonatal facility.
The implementation of our design followed the outcome of our selections based on reliability and the testing of existing commercial products, which were later re-morphed to achieve the hybrid construct of polite-light-bank. The developed system was affordable with ease of installation at the centres and has been assessed with a very high success rating in its four years of operation. The overall system satisfaction score was from the two centres, where the PLB was reported to have created a sharp night contrast during blackouts, between the neonatal centre and the rest of the hospital complex, respectively. The consistency of the PLB operations in the last four years at the Amina-centre is noticeable, with nostalgic appreciation that a certain section of the Minna General Hospital complex would always remain aglow all night long even during power blackouts that may last for many days. The PLB at the Amina-centre was a technology beyond expectation in terms of reliability and longevity as perceived at Minna General Hospital setting; hence, earning this facility the nickname of "the centre that never sleeps". The PLB is a breakthrough in the sourcing and development of relevant technologies for taking neonatal care into the hinterlands where the significant volume of the needy neonate dwell [7]. The high success rate, as reported from the hospitals, demonstrates that the PLB-technology could be a conclusive answer to the question of facility lighting for actualising the neonatal-rescue-scheme concept of Amadi et al. 2022 as proposed in the literature[7].
IV. RECOMMENDATIONS
We wish to, with no hesitation, request the LMICs governments, supervisory authorities and individual philanthropist organisations who wish to positively reverse the trends of neonatal indices to urgently deploy this aspect of the NRS concept and save these precious lives.
ACKNOWLEDGEMENTS
We wish to thank the staff and particularly the ward mangers at the Amina neonatal care centre, Minna and the Calabar Women and Children Hospital, Mrs Maryam Usman and Mr Gabriel Etim Adim, for sharing their experiences, supervisions and assessments via our questionnaires. We appreciate all technical supports from Mr Jude Nzerem and Mr Jerry Okoye. We thank Mrs Owanari Donald Duke and Professor Martin Meremikwu for their partnership. This research was primarily supported by the Neonatal Concerns for Africa, a subsidiary of the Mastermind group Nigeria. The Hornchurch Baptist Church, Essex England, United Kingdom supports Professor H Amadi's medical outreach in Nigeria.
Conflicts of Interest
We do not have any conflicts of interest to declare.



