The recent COVID-19 pandemic highlighted the challenges in healthcare settings due to the scarcity of medical resources like hospital beds and healthcare professionals to manage critical cases. During this critical period, healthcare professionals emphasized on saving lifethreatening cases, including moderate to severe COVID-19 cases, as they might need either ventilators or treatment in intensive care units. As a result, the national and international health policymakers, including WHO, suggested managing the suspected or confirmed COVID-19 patients without symptoms or having mild symptoms at home to reduce the burden on hospitals and trained healthcare professionals. Hence, we aimed to conduct a telephone-based pilot study to examine the feasibility before conducting a large-scale study on home-care treatment and management of the confirmed or suspected COVID-19 Bangladeshi patients, either asymptomatic or mild-symptomatic, during the home quarantine period.
## I. INTRODUCTION
For more than a century, human history tackled several significant infectious diseases outbreaks, including the first worldwide flu pandemic (1729-1730), the "Spanish flu" as the first pandemic of the $20^{\text{th}}$ century, and the "H1N1 pandemic of 2009" in the $21^{\text{st}}$ century [1]. A recent addition was the Coronavirus Disease 2019 (COVID-19) outbreak acknowledged by the World Health Organization (WHO) on March 11, 2020, as a global pandemic due to its worldwide distressing levels of spread and severity related to morbidity and mortality [2]. Globally, more than 645 million confirmed cases of COVID-19, including more than six million deaths, were reported on December 11, 2022 [3].
Before the initiation of the recent COVID-19 pandemic in Wuhan, China, in December 2019, caused by the novel coronavirus "Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2)", two more highly contagious coronaviruses (CoVs) belonged to the Coronaviridae family emerged in the $21^{\mathrm{st}}$ century to lead an outbreak. One was the Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) which appeared first in southern Foshan, China, before spreading to more than 30 countries from 2002 to 2003. After ten years, the Middle East Respiratory Syndrome Coronavirus (MERS-CoV) emerged in Saudi Arabia and affected two dozen countries from 2012 to 2016 [4]. Though these three highly pathogenic and deadly human coronaviruses were more or less similar [5] and are primarily spread through the respiratory droplet route, and direct contact [6], SARS-CoV2 is much more transmissible and communicable. Hence, this latest coronavirus is responsible for a global outbreak and health disaster [7].
Even though the world faced the SARS-CoV and MERS-CoV outbreaks early, these experiences did not contribute much to improving the healthcare system, particularly the public health practice, to mitigate the devastating impact of COVID-19. Instead, this pandemic identifies the health inequalities and challenges the healthcare system of both developed and developing countries [8, 9]. The COVID-19 pandemic not only severely affected the access and healthcare service utilization of non-COVID-19 health issues like maternal health [10], mental health [11], and non-communicable diseases [12] due to having a fear of being contaminated with COVID-19 infection while receiving treatment in healthcare facility settings; it also affected the treatment and management of asymptomatic and mild COVID-19 patients in the healthcare settings due to shortage of medical resources like hospital beds and healthcare professionals to manage the critical cases [13]. Due to inaccessibility to timely healthcare services and difficulty in accessing treatment, asymptomatic or mild symptomatic COVID-positive patients had to depend on home-based treatment.
During this critical period, more emphasis was given to saving life-threatening cases, including moderate to severe COVID-19 cases, through reshaping the healthcare facilities [14] as these infective patients might need either ventilators or treatment in intensive care units. Besides, to prevent the spread of this deadly viral infectious disease, one of the effective preventive strategies was lockdown which restricted human mobility as it slowed down the spread of this infectious disease mainly by direct contact [15]. Throughout the COVID-19 pandemic period, more than 140 countries around the globe enforced this movement restriction to slow down the rapid spread of coronavirus [16], which also affected healthcare-seeking behaviours. Studies conducted in developed countries like New Zealand and Germany found that lockdowns negatively affected healthcare-seeking behaviour; respondents delayed seeking healthcare, leading to fewer consultations and hospital admissions [17, 18].
As the lack of sufficient medical resources and movement restrictions destructively and undesirably affected healthcare utilization in a formal setting, it initiated the continuity of healthcare at home. To reduce the burden on hospitals and trained healthcare professionals, the WHO suggested managing suspected or confirmed COVID-19 patients without symptoms or who have mild symptoms at home [19]. The Directorate General of Health Services (DGHS) under the Ministry of Health & Family Welfare, Bangladesh, also developed the national guideline to manage the clinical cases of COVID-19 where they suggested treating and managing the asymptomatic and mild COVID-19 patients at home [20]. Until November 27, 2022, there were 2,036,527 confirmed COVID-19 cases, including 29,431 deaths in Bangladesh, one of the most affected countries. Half of the reported cases were from Dhaka, the capital city and $62\%$ were from the Dhaka division [21].
Bangladesh has an inadequate and inequitable medical workforce (only five physicians and two nurses serve on average every 10,000 population) [22]; besides, low-quality medical equipment like masks and personal protective equipment was provided to the Bangladeshi health front liners to manage the pandemic situation in healthcare facility settings [23]. Subsequently, many medical professionals suffered from COVID-19-related morbidity and mortality. Bangladesh has one of the highest medical professional mortality rates globally [24]. This workforce crisis and suffering also limited the healthcare-seeking behaviour of Bangladeshi COVID-19-positive patients. As a result, it was found that $79\%$ of patients preferred to stay at home to get treatment [23].
It becomes essential to investigate the home-care management of confirmed COVID-19 Bangladeshi patients, especially what kinds of treatment regimen they used to receive to recover while staying at home, whether they consulted with any qualified doctors or not, which kinds of medicine they received, either allopathic (science-based modern medicine) or alternative or supplementary medicine, whether they took any precautionary measures to prevent the spread of infection in addition to the treatment regimen. Hence, we aimed to conduct a telephone-based pilot study to examine the feasibility before conducting a large-scale study to contribute to the development of healthcare policy to strengthen the institutional and community support systems to provide the best home-care treatment and management to the confirmed COVID-19 Bangladeshi patients during the home quarantine period. It also targets to develop an effective protocol for home-based treatment for asymptomatic and mild-symptomatic COVID-19 patients, who can stay at home during their illness & home quarantine period. It can reduce the burden on hospitals where healthcare professionals can dedicate their services to save the lives of moderate to severe symptomatic, even very critical patients.
## II. MATERIALS AND METHODS
Study design & study population: We conducted a cross-sectional telephone-based pilot study combining a mixed-methods approach between June 10, 2020, and August 30, 2020, during the lockdown period. Our trained data collectors, who were junior doctors, obtained informed verbal consent before the initiation of each interview; they also informed the study respondents about their right to withdraw or stop the interview at any point in time, as their participation is voluntary. We also assured the respondents about the confidentiality of the data they provided as it will not be disclosed to anyone except the research team, and their de-identified data will be presented in an aggregated form to ensure the anonymity of their information.
Under the quantitative component, we collected data using a structured questionnaire from 101 adult COVID-19 patients, both male and female, who received treatment at home after being diagnosed as COVID-19 positive. In addition, we conducted a qualitative study, especially in-depth interviews, using a semi-structured guideline (Supplementary document: S1) and collected data from healthcare providers who provided consultancy to these patients. Besides, we composed two case studies.
Data collection: We aimed to collect data from all eight administrative divisions (Dhaka, Barisal, Chattogram, Khulna, Mymensingh, Rajshahi, Rangpur, and Sylhet) of Bangladesh.
Researchers used the snowball technique to collect the contact numbers of the study population. Initially, we received the cooperation of the Divisional Public Health Expert Advisors' team, who were appointed by the Ministry of Health and Family Welfare (MOHFW) and attached to the Directorate General of Health Services (DGHS). We used purposive sampling to select a few indexes of COVID-19 patients receiving treatment at home. Then, by snowball technique, we collected the name and contact numbers of their family members, friends, relatives, and neighbors who were adults aged 18 years and above, Bangladeshi citizens, had mobile phones, and were taking home-based treatment. Thus, we created a list of 287 eligible respondents and considered this list as the sampling frame. Our trained and experienced data collectors, who were doctors, contacted the eligible participants over the telephone and invited them to join the study. In some cases, we made prior appointments before collecting data. Our trained data collectors made a phone call to these 287 patients an average of three times. Finally, 101 respondents, who were residing in four administrative divisions (Dhaka, Barisal, Mymensingh, and Sylhet), completed the interview.
We developed the structured questionnaire for the quantitative component of the study based on the national guideline for the management of COVID-19 and WHO recommendations [19, 20]. It mainly consisted of close-ended questions with only one open-ended question related to social issues, including stigma. We developed the questionnaire in English and then translated it into the local language, Bangla. Two content experts reviewed both versions for content validation in the Bangladesh context. Later, we conducted a mini-pilot study with 10 adult COVID-19 patients before we finalized the questionnaire. We also developed a semi-structured guideline to conduct the in-depth interview with healthcare professionals, which was submitted as a Supplementary document.
Statistical analysis: We performed the descriptive analysis and presented the study findings in frequency and percentage. We analysed the data using version 4.0.3 of the R program, an open-source software. Qualitative data were analysed under themes and sub-themes.
## III. RESULTS
In this study, 101 respondents were interviewed; most of the respondents were young adults with mean and median ages of $32 \pm 10$ years and 29 years [minimum 17 years to maximum 65 years], respectively. Slightly more than half (54%) were male, and almost two-thirds (71%) were married. Almost all respondents (93%) were Muslim, and more than half (63%) of the respondents completed their graduation. The majority (83%) of the respondents were residing in the peripheral divisions, considered semi-urban and rural residence places. Slightly more than one-third (37%) of the respondents were service holders working either in government or private sectors; 22% were healthcare professionals consisting of doctors, nurses, and health workers. Only 13% were housemakers, and 15% were students. More than half (58%) had a monthly income of 30K Bangladesh Taka (BDT) and above (286US$, at the rate of 105BDT/US$), though 7% did not want to share their income with researchers.
We also analysed the socio-demographic characteristics of study respondents by sex and place of residence. We did not find substantial variations between males and females regarding socio-demographic characteristics except for their occupations. There were more employed male participants (64%) than female participants (52%); the majority (38%) of them worked in the government sector, followed by the private sector (13%). Among the female respondents, almost one-third (28%) were homemakers. Besides, the most common profession of the employed female respondents was health professionals (33%), followed by government employees (15%).
Regarding the place of residence, we found variation between those who lived in rural areas and those who lived in urban areas; only $17\%$ lived in urban areas. The detailed socio-demographic characteristics of the study respondents are presented in Table 1 under three categories: overall, by sex, and place of residence.
Table 1: Socio-demographic characteristics of study respondents
<table><tr><td rowspan="3">Socio-demographic characteristics</td><td rowspan="2">Total (n =101)</td><td colspan="2">Sex</td><td colspan="2">Place of Residence</td></tr><tr><td>Male (n=55)</td><td>Female (n=46)</td><td>Urban (n=17)</td><td>Rural (n=84)</td></tr><tr><td>Number (%)</td><td>Number (%)</td><td>Number (%)</td><td>Number (%)</td><td>Number (%)</td></tr><tr><td>Age</td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Mean (±SD)</td><td>32 (±10)</td><td>32 (±10)</td><td>31 (±11)</td><td>35 (±10)</td><td>31 (±10)</td></tr><tr><td>Median [Min, Max]</td><td>29 [17, 65]</td><td>30 [18, 65]</td><td>28 [17, 62]</td><td>32 [25, 55]</td><td>29 [17, 65]</td></tr><tr><td>20 years and below</td><td>7 (7%)</td><td>2 (4%)</td><td>5 (11%)</td><td>0 (0%)</td><td>7 (8%)</td></tr><tr><td>21 to 40 years</td><td>78 (77%)</td><td>44 (80%)</td><td>34 (74%)</td><td>12 (71%)</td><td>66 (79%)</td></tr><tr><td>41 years and above</td><td>16 (16%)</td><td>9 (16%)</td><td>7 (15%)</td><td>5 (29%)</td><td>11 (13%)</td></tr><tr><td>Sex</td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Male</td><td>55 (54%)</td><td></td><td></td><td>9 (53%)</td><td>46 (55%)</td></tr><tr><td>Female</td><td>46 (46%)</td><td></td><td></td><td>8 (47%)</td><td>38 (45%)</td></tr><tr><td>Marital status</td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Unmarried</td><td>25 (25%)</td><td>12 (22%)</td><td>13 (28%)</td><td>5 (29%)</td><td>20 (24%)</td></tr><tr><td>Married</td><td>72 (71%)</td><td>41 (75%)</td><td>31 (67%)</td><td>11 (65%)</td><td>61 (73%)</td></tr><tr><td>Widow/Widower/Divorce</td><td>3 (3.0%)</td><td>1 (2%)</td><td>2 (4%)</td><td>1 (6%)</td><td>3 (3.0%)</td></tr><tr><td>Missing</td><td>1 (1.0%)</td><td>1 (1.8%)</td><td>0 (0%)</td><td>0 (0%)</td><td>1 (1%)</td></tr><tr><td>Religion</td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Islam</td><td>94 (93%)</td><td>51 (93%)</td><td>43 (93%)</td><td>15 (88%)</td><td>79 (94%)</td></tr><tr><td>Hindu</td><td>5 (5%)</td><td>3 (5%)</td><td>2 (4%)</td><td>2 (12%)</td><td>3 (4%)</td></tr><tr><td>Catholic</td><td>2 (2%)</td><td>1 (2%)</td><td>1 (2%)</td><td>0 (0%)</td><td>2 (2%)</td></tr><tr><td>Education</td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>SSC/O Level and below</td><td>15 (15%)</td><td>7 (13%)</td><td>8 (17%)</td><td>1 (6%)</td><td>14 (17%)</td></tr><tr><td>HSC/A Level</td><td>21 (21%)</td><td>16 (29%)</td><td>5 (11%)</td><td>1 (6%)</td><td>20 (24%)</td></tr><tr><td>Graduate</td><td>51 (50%)</td><td>26 (47%)</td><td>25 (54%)</td><td>10 (59%)</td><td>41 (49%)</td></tr><tr><td>Post graduate</td><td>13 (13%)</td><td>5 (9%)</td><td>8 (17%)</td><td>5 (29%)</td><td>8 (10%)</td></tr><tr><td>Missing data</td><td>1 (1%)</td><td>1 (2%)</td><td>0 (0%)</td><td>0 (0%)</td><td>1 (1%)</td></tr><tr><td>Place of residence</td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Urban/Central division</td><td>17 (17%)</td><td>9 (16%)</td><td>8 (17%)</td><td></td><td></td></tr><tr><td>Rural/Periphery division</td><td>84 (83%)</td><td>46 (84%)</td><td>38 (83%)</td><td></td><td></td></tr><tr><td>Division of residence</td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Dhaka [urban, central division]</td><td>17 (17%)</td><td>9 (16%)</td><td>8 (17%)</td><td>17 (100%)</td><td>0 (0%)</td></tr><tr><td>Chattogram[rural, periphery division]</td><td>2 (2%)</td><td>1 (2%)</td><td>1 (2%)</td><td>0 (0%)</td><td>2 (2%)</td></tr><tr><td>Mymensingh [rural, periphery division]</td><td>11 (11%)</td><td>5 (9%)</td><td>6 (13%)</td><td>0 (0%)</td><td>11 (13%)</td></tr><tr><td>Rangpur [rural, periphery division]</td><td>65 (64%)</td><td>36 (65%)</td><td>29 (63%)</td><td>0 (0%)</td><td>65 (77%)</td></tr><tr><td>Sylhet [rural, periphery division]</td><td>6 (6%)</td><td>4 (7%)</td><td>2 (4%)</td><td>0 (0%)</td><td>6 (7%)</td></tr><tr><td>Occupation</td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Government service</td><td>28 (28%)</td><td>21 (38%)</td><td>7 (15%)</td><td>4 (24%)</td><td>24 (29%)</td></tr><tr><td>Private sector service</td><td>9 (9%)</td><td>7 (13%)</td><td>2 (4%)</td><td>0 (0%)</td><td>9 (11%)</td></tr><tr><td>Health professional (doctors, nurses, health workers)</td><td>22 (22%)</td><td>7 (13%)</td><td>15 (33%)</td><td>7 (41%)</td><td>15 (18%)</td></tr><tr><td>Student</td><td>15 (15%)</td><td>8 (15%)</td><td>7 (15%)</td><td>1 (6%)</td><td>14 (17%)</td></tr><tr><td>Homemakers/housewives</td><td>13 (13%)</td><td>0 (0%)</td><td>13 (28%)</td><td>3 (18%)</td><td>10 (12%)</td></tr><tr><td>Others</td><td>14 (14%)</td><td>12 (22%)</td><td>2 (4%)</td><td>2 (12%)</td><td>12 (14%)</td></tr><tr><td>Income</td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Less than 30K BDT</td><td>36 (36%)</td><td>22 (40%)</td><td>14 (30%)</td><td>3 (18%)</td><td>33 (39%)</td></tr><tr><td>30K-60K BDT</td><td>39 (39%)</td><td>20 (36%)</td><td>19 (41%)</td><td>3 (18%)</td><td>36 (43%)</td></tr><tr><td>61K -100K BDT</td><td>9 (9%)</td><td>3 (5%)</td><td>6 (13%)</td><td>2 (12%)</td><td>7 (8%)</td></tr><tr><td>More than 100K BDT</td><td>10 (10%)</td><td>4 (7%)</td><td>6 (13%)</td><td>9 (53%)</td><td>1 (1%)</td></tr><tr><td>Did not want to share</td><td>7 (7%)</td><td>6 (11%)</td><td>1 (2%)</td><td>0 (0%)</td><td>7 (8%)</td></tr></table>
In this study, half (50%) of the COVID-19-infected participants reported having signs and symptoms within 7-15 days; this finding is more or less the same between male and female respondents and among those who lived in urban and rural areas. Of the total participants, $44\%$ had symptoms within seven days or less, i.e., they became asymptomatic within a week. We found that more females $(48\%)$ and those who lived in rural areas $(46\%)$ became asymptomatic within seven days or less. Only $7\%$ had prolonged symptoms as they remained symptomatic for more than 15 days, mainly those who were male (9%) and lived in urban areas (18%) (Table -2).
On average, study respondents received their COVID-19 test results within seven days, except those residing in urban areas; they received their results within
4-5 days. The study also found a wide range of durations to receive the confirmed test results, ranging from one day to 19 days. Additionally, $8\%$ of the respondents, mainly females $(13\%)$ residing in rural areas $(8\%)$, could not recall when they received the test results.
Table 2: Duration of signs and symptoms of COVID-19-positive persons and duration of COVID-19 test confirmation
<table><tr><td></td><td>Total</td><td>Male</td><td>Female</td><td>Urban</td><td>Rural</td></tr><tr><td></td><td>(n=101)</td><td>(n=55)</td><td>(n=46)</td><td>(n=17)</td><td>(n=84)</td></tr><tr><td>Duration of Symptoms (%)</td><td>Number (%)</td><td>Number (%)</td><td>Number (%)</td><td>Number (%)</td><td>Number (%)</td></tr><tr><td><7 days</td><td>44 (44%)</td><td>22 (40%)</td><td>22 (48%)</td><td>5 (29%)</td><td>39 (46%)</td></tr><tr><td>7-15 days</td><td>50 (50%)</td><td>28 (51%)</td><td>22 (48%)</td><td>9 (53%)</td><td>41 (49%)</td></tr><tr><td>>15 days</td><td>7 (7%)</td><td>5 (9%)</td><td>2 (4%)</td><td>3 (18%)</td><td>4 (5%)</td></tr><tr><td colspan="6">Duration of COVID-19 Test confirmation</td></tr><tr><td>Mean (±SD),days</td><td>7.1 (3.7)</td><td>7.0 (3.5)</td><td>7.1 (4.1)</td><td>4.7 (3.0)</td><td>7.6 (3.7)</td></tr><tr><td>Median [Min, Max], days</td><td>7.0 [1.0, 19]</td><td>6.0 [2.0, 16]</td><td>7.0 [1.0, 19]</td><td>4.5 [1.0, 13]</td><td>7.0 [2.0, 19]</td></tr><tr><td>Could not remember</td><td>8 (8%)</td><td>2 (4%)</td><td>6 (13%)</td><td>1 (6%)</td><td>7 (8%)</td></tr></table>
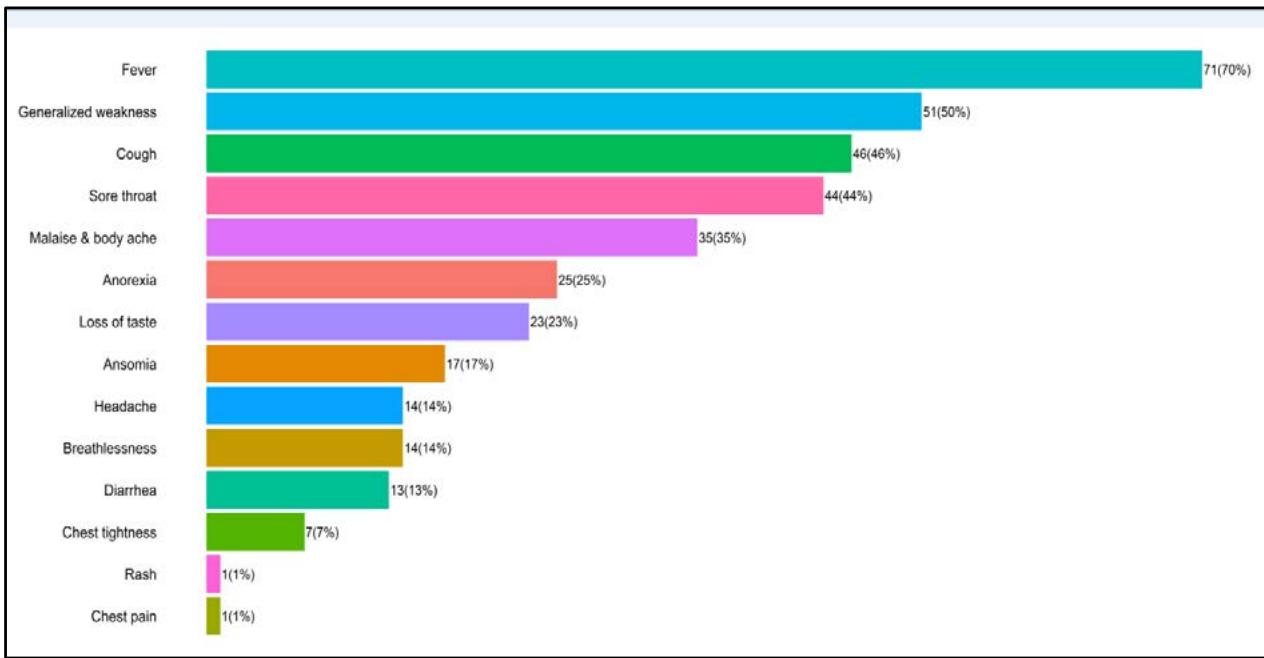
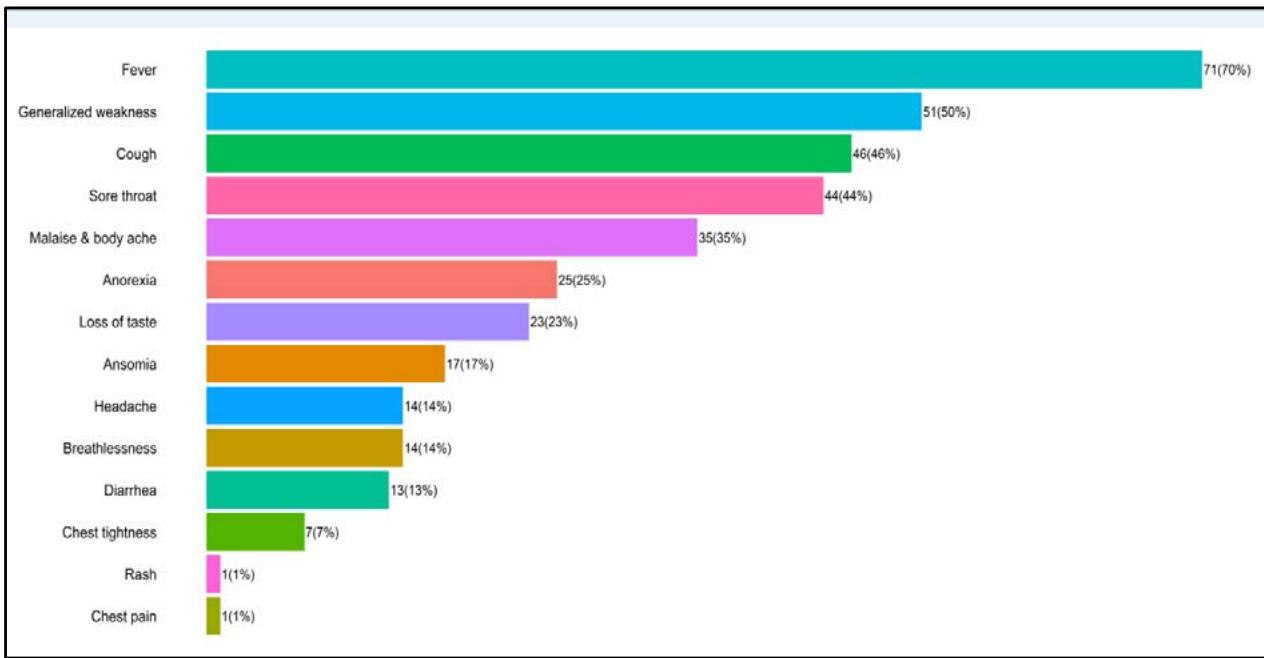 Fig. 1: Signs and symptoms of the respondents during COVID-19 infection
Fever was the most frequent symptom reported by respondents; less than two-thirds (70%) had a fever during their illnesses. The second most common symptom was generalized weakness (50%), followed by cough (46%), sore throat (44%), and malaise & body ache (35%). One-fourth of the respondents complained about anorexia, and less than one-fourth (23%) lost their taste. In our study, less than one-fourth (21%) had severe symptoms like breathlessness (14%) and chest tightness (7%), yet, they continued to stay at home even after knowing that their health conditions could be critical at any point in time due to these symptoms (Fig 1).
Though the respondents continued treatment at home, slightly more than half (52%) of the respondents made face-to-face consultations with doctors before starting the home-based treatment, and 38% consulted with doctors over the telephone. Only 6%, who were doctors, started taking the treatment by themselves. Most of the respondents (90%) depended on allopathy medicine (science-based modern medicine). On average, respondents took six medicines for the COVID-19 treatment. However, there was no variation between males and females, and was found that urban respondents took more medicines (seven medicines) than rural respondents. On average, respondents spent
22,000 BDT (USD 209, at the rate of 105BDT/US$) to buy medicines during their illnesses (Table 3); we found that male respondents spent more than female
respondents, though there was no variation between urban and rural respondents.
Table 3: COVID-19 treatment and its cost related information
<table><tr><td></td><td>Total</td><td>Male</td><td>Female</td><td>Urban</td><td>Rural</td></tr><tr><td></td><td>(n=101)</td><td>(n=55)</td><td>(n=46)</td><td>(n=17)</td><td>(n=84)</td></tr><tr><td>Source of treatment information (%)</td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>In-person consultation with Doctor</td><td>53 (52%)</td><td>30 (55%)</td><td>23 (50%)</td><td>5 (29%)</td><td>48 (57%)</td></tr><tr><td>Telephonic consultation with Doctor</td><td>38 (38%)</td><td>20 (36%)</td><td>18 (39%)</td><td>10 (59%)</td><td>28 (33%)</td></tr><tr><td>Self</td><td>6 (6%)</td><td>4 (7%)</td><td>2 (4%)</td><td>2 (12%)</td><td>4 (5%)</td></tr><tr><td>ShaysthoBatayon</td><td>1 (1%)</td><td>0 (0%)</td><td>1 (2%)</td><td>0 (0%)</td><td>1 (1%)</td></tr><tr><td>Advice from Doctor at any social media</td><td>1 (1%)</td><td>1 (2%)</td><td>0 (0%)</td><td>0 (0%)</td><td>1 (1%)</td></tr><tr><td>Missing</td><td>2 (2%)</td><td>0 (0%)</td><td>2 (4%)</td><td>0 (0%)</td><td>2 (2%)</td></tr><tr><td>Types of treatment</td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Allopathy</td><td>91 (90%)</td><td>46 (84%)</td><td>45 (98%)</td><td>16 (94%)</td><td>75 (89%)</td></tr><tr><td>Ayurveda</td><td>2 (2%)</td><td>2 (4%)</td><td>0 (0%)</td><td>0 (0%)</td><td>2 (2%)</td></tr><tr><td>Homeopathy</td><td>6 (6%)</td><td>5 (9%)</td><td>1 (2%)</td><td>1 (6%)</td><td>5 (6%)</td></tr><tr><td>Missing</td><td>2 (2%)</td><td>2 (4%)</td><td>0 (0%)</td><td>0 (0%)</td><td>2 (2%)</td></tr><tr><td>Number of Medicine consumed</td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>(Mean (±SD)</td><td>5.6 (2.2)</td><td>5.7 (2.4)</td><td>5.5 (2.1)</td><td>7.2 (2.6)</td><td>5.3 (2.0)</td></tr><tr><td>Median [Min, Max]</td><td>5.0
[1.0, 12]</td><td>5.0
[1.0, 12]</td><td>5.0
[1.0, 11]</td><td>6.0
[4.0, 12]</td><td>5.0
[1.0, 11]</td></tr><tr><td>Treatment cost</td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>(Mean (±SD) in Taka</td><td>22000
(30000)</td><td>26000
(38000)</td><td>16000
(13000)</td><td>21000
(16000)</td><td>22000
(32000)</td></tr><tr><td>Median [Min, Max] in Taka</td><td>15000
[3000,
150000]</td><td>15000
[3000,
150000]</td><td>13000
[3000,
55000]</td><td>15000
[6000,
55000]</td><td>12000
[3000,
150000]</td></tr><tr><td>Did not want to share</td><td>19 (19%)</td><td>12 (22%)</td><td>7 (15%)</td><td>3 (18%)</td><td>16 (19%)</td></tr><tr><td>Did not spend any money for treatment</td><td>11 (11%)</td><td>4 (7%)</td><td>7 (15%)</td><td>0 (0%)</td><td>11 (13%)</td></tr></table>
Among allopathy medicine, paracetamol was the commonest; $80\%$ of respondents took it. Most participants also reported taking vitamin C $(77\%)$ and Zinc $(72\%)$. More than half of the participants $(65\%)$ consumed the Azithromycin antibiotic, while a smaller proportion (only $17\%$ ) used Ivermectin.
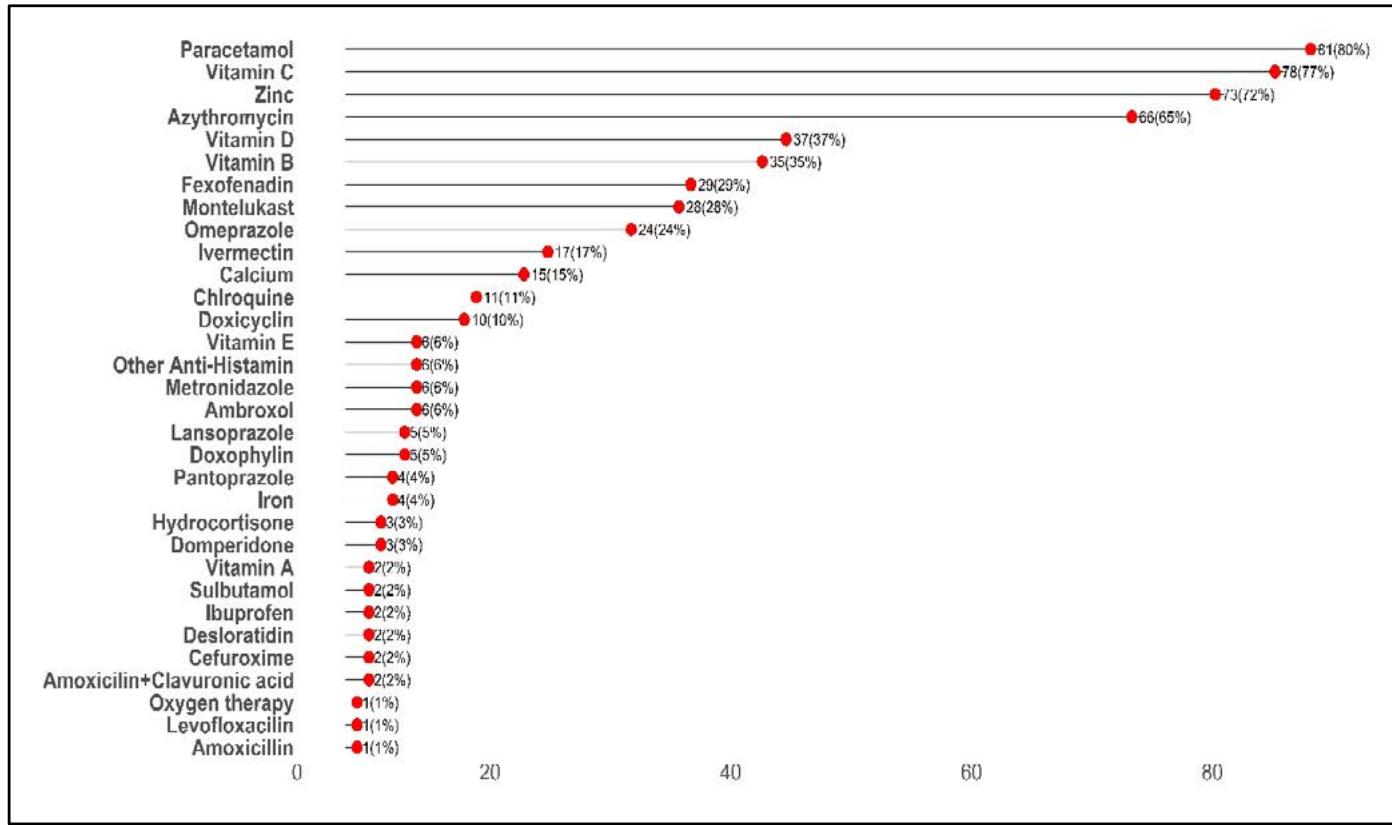 Fig. 2: Medicines consumed by the respondents during COVID-19 infection in%
Respondents also consumed different kinds of supplementary foods as recommended by local physicians, relatives, and friends; $92\%$ took extra lemon to get rid of this disease, $89\%$ consumed a high protein diet as they believed that it would be beneficial for them, and $83\%$ had taken ginger to counteract the deadly disease. More than half of the respondents also added
other supplement food items in their diets, such as spice tea (70%), fruits (62%), nigella seeds (55%), cardamom (54%), cloves (54%), cinnamon (52%), and lemon tea (51%). While comparing between males and females, we found that male respondents took slightly more additional supplements than female respondents. (Table 4).
Table 4: Frequency of different supplements taken by overall, male and female participants
<table><tr><td></td><td>Overall</td><td>Male</td><td>Female</td></tr><tr><td></td><td>N=101</td><td>N=55</td><td>N=46</td></tr><tr><td>Lemon</td><td>93(92%)</td><td>48(48%)</td><td>45(45%)</td></tr><tr><td>High protein diet(Egg/Meat/Fish)</td><td>90(89%)</td><td>50(50%)</td><td>40(40%)</td></tr><tr><td>Ginger</td><td>84(83%)</td><td>46(46%)</td><td>38(38%)</td></tr><tr><td>Spice tea</td><td>71(70%)</td><td>39(39%)</td><td>32(32%)</td></tr><tr><td>Fruits</td><td>63(62%)</td><td>35(35%)</td><td>28(28%)</td></tr><tr><td>Nigella seeds</td><td>56(55%)</td><td>31(31%)</td><td>25(25%)</td></tr><tr><td>Cardamom</td><td>55(54%)</td><td>30(30%)</td><td>25(25%)</td></tr><tr><td>Clove</td><td>55(54%)</td><td>26(26%)</td><td>29(29%)</td></tr><tr><td>Cinnamons</td><td>53(52%)</td><td>27(27%)</td><td>26(26%)</td></tr><tr><td>Lemon tea</td><td>52(51%)</td><td>29(29%)</td><td>23(23%)</td></tr><tr><td>Honey</td><td>45(45%)</td><td>22(22%)</td><td>23(23%)</td></tr><tr><td>Bay leaves</td><td>34(34%)</td><td>14(14%)</td><td>20(20%)</td></tr><tr><td>Garlic</td><td>34(34%)</td><td>20(20%)</td><td>14(14%)</td></tr><tr><td>Black pepper</td><td>26(26%)</td><td>13(13%)</td><td>13(13%)</td></tr><tr><td>Tulsi leaves</td><td>7(7%)</td><td>3(3%)</td><td>4(4%)</td></tr><tr><td>Mustard oil</td><td>5(5%)</td><td>3(3%)</td><td>2(2%)</td></tr><tr><td>Turmeric</td><td>3(3%)</td><td>0(0%)</td><td>3(3%)</td></tr><tr><td>Green tea</td><td>2(2%)</td><td>0(0%)</td><td>2(2%)</td></tr><tr><td>Others</td><td>18(18%)</td><td>9(9%)</td><td>9(9%)</td></tr></table>
In addition to medicine and supplementary foods, respondents also provided information on multiple precautionary measures they practiced during their sickness period (Fig 3). Among them, hot water gurgling $(84\%)$, steam inhalation $(79\%)$, and drinking hot water $(76\%)$ were the three most frequently reported precautionary measures. Over half $(66\%)$ of the respondents stayed in a separate room and used a
separate toilet during isolation. Respondents also engaged in different kinds of exercise as a precautionary measure; breathing exercise (35%) was the most common, as it is very effective in maintaining proper oxygen concentration at the tissue level. This precautionary measure was mainly practiced by female participants (46%) compared to male participants (25%).
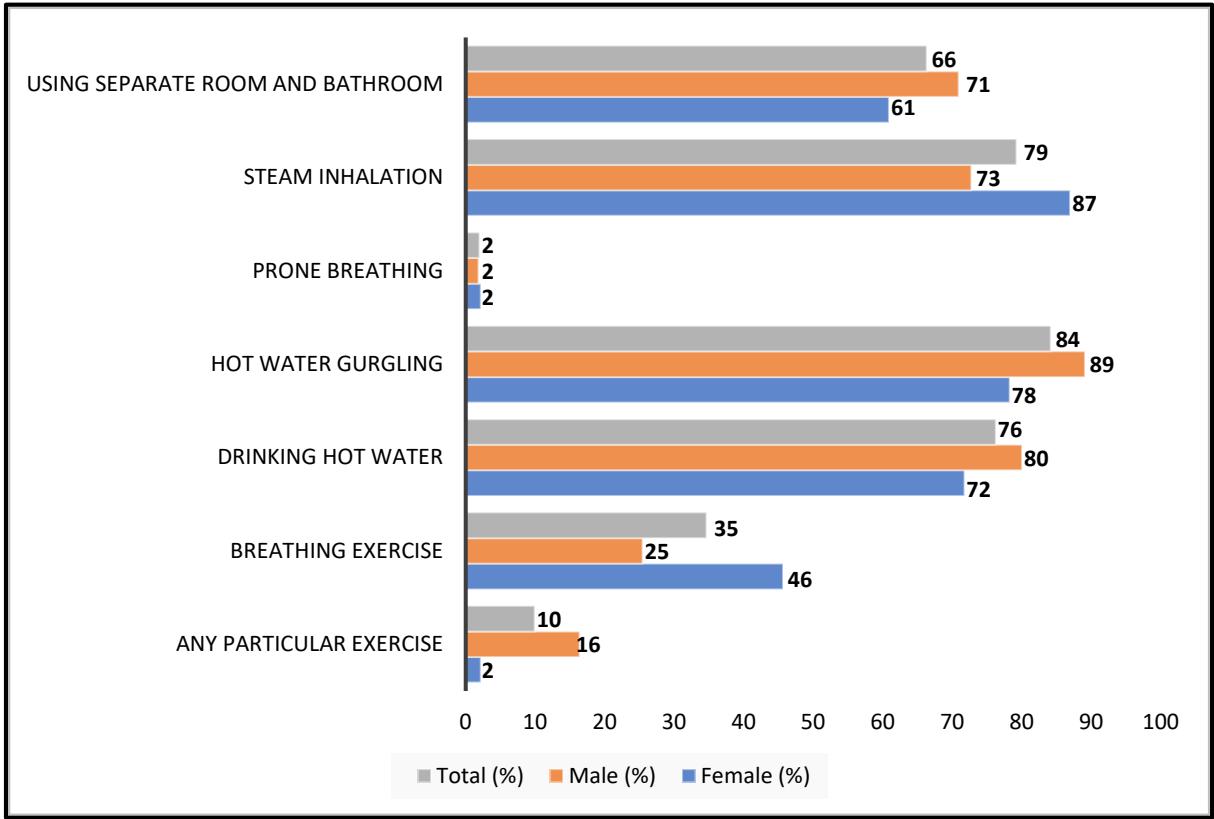 Fig. 3: Precautionary measurement taken by the respondents by overall, male and female participants
Qualitative study findings on social issues, including stigma: Almost all respondents $(92.4\%)$ did not want to disclose to their neighbors, friends, and even family members that they were infected and taking medicines at home. All of their household members, who learned that the study respondents were infected, were scared that they might become infected at any time. To avoid spreading the infection and reduce fear and anxiety, the infected persons stayed inside their rooms and used a separate toilet during isolation. The respondents, who did not have the opportunity to stay in a separate room, used separate beds and tried not to go close to the other family members. During this time, respondents wore face-mask even if they were staying inside the room to curb the transmission of the virus.
In the case of 12 positive patients, Government officials hung a small red flag on the front wall of their houses. This government act raised local level fear, and the community people started making further negative comments about the infected persons. This situation was not at all appreciated by the COVID-19-patients and their relatives. Besides, by seeing the red flag in front of the house, the community people came to know about the infected person who did not go out during their illness periods. It also initiated rumours. One of the common negative comments made by the community was that the COVID-19 infection was the outcome of some sins made by the infected person. Community people were aware that this disease was highly contagious, and as such, they deliberately stay away
from the sick person, which turned out to be a good practice, particularly in maintaining social distancing.
### Study findings of in-depth interview
According to the study protocol, we interviewed three doctors in-depth. Two doctors were working in Government Hospitals and one in a private Medical College Hospital; they were assigned to manage the COVID-19 patients by their respective hospital authorities. They knew that many COVID-19 patients had to stay at home, where they recovered without facing any problems. Very few patients wanted to visit hospitals for admission and treatment during June-August 2020 as they were scared of exposure to COVID-19 infection. This situation was different in April – June 2020; at that time, many patients visited hospitals during the pandemic's earlier phase as they were unaware of the highly contagious nature of COVID-19 infection.
During the in-depth interview, we collected data that covered the following three themes: a) signs, symptoms, and complaints of the COVID-19 patients who visited hospitals; b) what kind of medicines were taken by the COVID-19 patients before admission; c) co-morbidities of the COVID-19 patients who visited hospitals. The study findings of the in-depth interview are presented below:
a) Signs, symptoms, and complaints of the COVID-19 patients who visited hospitals: Most COVID-19 patients gave a history of fever a couple of days before visiting hospitals, and some visited with a fever. Most of them had a dry cough, irritation in the throat, and sore throat. Many were asymptomatic but visited hospitals as they had positive COVID-19 test results. Almost all of them had tension, anxiety, and fear that their health situation might turn serious quickly within a short time. Most of them complained of generalized weakness and a lethargic feeling. A small percentage complained of loss of taste and anosmia. Very few persons (5% to 10%) complained of tightness in the chest, shortness of breath, difficulty breathing, and a smaller percentage had hypoxia. Many COVID-19 patients presented their CT scan chest reports with findings of having pneumonia. Most patients visited of their own interest, while very few were referred by private practitioners or some smaller hospitals/clinics. b) Types of medicines taken by the COVID-19 patients before admission: Almost all COVID-19 patients took Azithromycin, Doxycycline, and other broad-spectrum antibiotics, and in some cases, they took two antibiotics together. In the pandemic's earlier phase, COVID-19 patients had taken Hydroxychloroquine; in the recent phase, COVID-19 patients have taken Ivermectin. Almost all patients had started taking an antihistamine in tablet form and cough syrup. Very few patients started
Favimipramid, prednisolone, and blood thinner/low-dose heparin. Many patients, along with allopathic medicines, opted to use herbal medicines such as Tulsi, Nigel seeds, lemon, and honey. They regularly drank warm water and gargled with warm water several times during the day; this was the common practice among many patients.
c) Co-morbidities of the COVID-19 patients who visited hospitals: Diabetes was the most common comorbidity among the COVID-19 patients who visited hospitals. Followed by the common co-morbidities were hypertension, heart disease, asthma, kidney disease, arthritis, and cancer of different organs. Very few patients $(2\% - 3\%)$ became critically ill and had to be transferred to ICU.
Case Study-1: Tension, anxiety, and fear almost killed Shafi (not the real name): Shafi works in a trading agency. One day, while returning home, he felt his head was heavy and feverish. Immediately, he thought about the dreaded virus, Corona, as it was spreading around. He decided to isolate himself from the other family members. He noticed the worry on his wife's face; children were asking whether their father would be recovered, and his old father was worried about his son. Anxiety and fear started to mount gradually. After two days, he went to give his sample for the RT-PCR test. While waiting for the results, he developed weakness and body aches; simultaneously, he noticed a loss of taste for all his favourite foods. Waiting for the result was the most challenging time to pass. A few days later, he received his COVID-19 positive result. Then, he started to take the treatment; he took lots of tablets and a capsule after consulting a doctor over the phone. He also received suggestions and advice from friends and well-wishers but decided to stick to the doctor's prescription.
He started drinking "masala" tea three times daily, which soon became tedious. He also maintained a physical distance from everyone and stayed isolated in his room. At the same time, he was taken a few preventive measures, such as washing his hands, gargling with hot water, and wearing a mask. He felt all these measured as a burden; he was not enjoying while continuing it. He started to have sleepless nights. The thought of providing how to support his family was constantly bothering him. Will there be a layoff? Will he be able to go back to his job? He continuously counted the days; meanwhile, only 14 days passed, which he felt as 14 months. Finally, his stressful period gradually came to an end. He started to feel better, and his symptoms started to go away. He thanked Allah for not developing any complications, which he had heard of so much from others. The actual relief came in his and his family's life when he tested COVID-19 negative on the $20^{\text{th}}$ day.
Case Study-2: Tender loving care and mental support are the winning points: Sheer simplicity and small happenings leave us spellbound and mesmerized. Such is the story of a young couple Parul and Ahmed (not their real names), living in a village about 2 kilometers away from the Upazilla Head Quarters with two children. Parul's husband, a shopkeeper, tested positive for COVID-19. They could not find the source from where he became infected with the virus. He sent his two children with their grandfather and grandmother to their uncle's house. His wife, Parul, did not want to leave her husband. Neighbors and community people warned that she would be infected too, but she stayed there with her husband and kept her vows. When we wanted to know the reasons, she replied with a smile, "where would I go, he's my everything". Soon her husband developed diarrhea and became very weak. Parul played the role of a real nurse. The whole illness period was about 18 days until he fully recovered, and during this period, the couple stayed at their residence. Parul not only nursed her husband but also cooked food and did everything that she could do. By the Grace of Almighty Allah, Parul never became sick and tested COVID-19 negative when she did her test with her husband, who went to repeat his test on day 18, at the end of his illness period. Ahmed said this was all possible by the Almighty's blessings on Parul, who was just an angel to him.
## IV. DISCUSSION
The COVID-19 pandemic provides an invaluable lesson to international and national health policymakers by highlighting the weakness of public healthcare and healthcare systems around the world in managing the different spectrum of COVID-19 patients, starting from asymptomatic suspected or confirmed to critical cases due to limited capacity, lack of medical forces and resources in the healthcare system in addition to the absence of effective antiviral therapeutics or vaccine [25]. During the early stage of the pandemic, when intense virus circulation was leading to high morbidity and mortality rates, many developed countries even faced difficulty in managing the high patient load in hospitals as patients were admitted with critical clinical features and often required ventilation support [26-29]. This sudden and unexpected increase in COVID-19 hospitalized patients played a critical role in enhancing anxiety, depression, burnout, and stress among healthcare professionals and affected the quality of care [30-35].
The COVID-19 pandemic not only burdens the healthcare system due to a lack of resources and shortage of healthcare professionals; it emphasizes the necessity for more extensive reinforcement of healthcare services. As it was not possible to increase the hospital bed capacity and the number of healthcare
professionals with appropriate expertise and skill during the crisis period instantly to cope with the pandemic demand, international and national health policymakers gave emphasis on the management of asymptomatic or mild symptomatic COVID-19 patients at home, and accordingly they developed the clinical management guideline [36]. A similar situation was observed in Bangladesh, where $79\%$ of the COVID-19 patients underwent home-based treatment according to the national clinical management guideline [23].
Our study found that fever was the most common symptom, followed by generalized weakness, cough, sore-throat, malaise & body ache, anorexia, and loss of taste. This study finding is supported by a systematic review investigating the clinical manifestations of 41,409 COVID-19-confirmed patients in 23 countries [37]. We also found that less than one-fourth (21%) of our study respondents could not visit COVID-19-designated hospitals to seek treatment even after developing severe symptoms like breathlessness and chest tightness due to a shortage of hospital beds. This kind of situation not only happened in low-resource countries like Bangladesh but also in Korea, where overcrowded patients and limited hospital resources forced the confirmed patients to stay at home [38].
COVID-19 is caused by a virus and there were antiviral medicines (Nirmatrelvir with Ritonavir (Paxlovid) and Remdesivir (Veklury) which can halt this virus to grow inside the body, and can diminish the risk of hospitalization and death [39, 40]. But in our study, we did not find any respondents who had taken these antiviral medicines; instead, they have taken antibiotics that are needed to manage bacterial infection, such as $66\%$ had taken Azithromycin, followed by Ivermectin $(17\%)$, Doxycycline $(10\%)$ and Chloroquine $(9\%)$. Very few patients had taken other antibiotics such as Amoxicillin, Levofloxacin, and Amoxicillin plus Clavulanic acid. A similar situation has been noticed in the African region, where 10 countries used antibiotics unreasonably to treat a viral disease [41]. Though, a five-day course of Ivermectin, an antiparasitic drug, was found harmless and effective in treating mild COVID-19 patients in Bangladesh [42]. On average, respondents had to spend 22,000 BDT (USD 209, at the rate of 105BDT/US$) to buy medicines during their illnesses and faced financial burdens as the pharmacists took unjustifiable benefit of the situation to make a considerable turnover. A similar situation was found in Ghana, where COVID-19 patients had to pay high for home-based treatment [43].
Our study respondents also consumed different kinds of supplementary foods, including herbal products and home-based remedies to counteract the deadly viral disease. We also discussed this issue with Bangladeshi herbal medicine specialists; they recommended these supplementary foods, such as Nigella seeds. Different studies also found that these supplementary products had an inhibitory effect on preventing human coronavirus[44-46]. Studies found that these home-based certain supplementary foods have protective effects, mainly to boost the immune system, against the COVID-19 infection [47-49].
In addition to food, our respondents also had taken multiple precautionary measures, which they practiced at home during their sickness period. Among them, hot water gurgling, steam inhalation, and drinking hot water were the three most frequently reported precautionary measures. Another Bangladeshi study also reported similar findings regarding these precautionary measures, though they did not find any impact of these measures on COVID-19 recovery phases [50]. There is insufficient evidence to support these precautionary measures to treat and prevent COVID-19 [51]; hence further studies are needed. Our study respondents also stayed in a separate room and used a separate toilet during isolation, and this measure is also suggested by the Centres for Disease Control and Prevention (CDC), the national public health agency of the United States [52]. Social distancing is also proven to be highly effective in alleviating the COVID-19 spread [53].
They also did breathe exercises, which effectively maintained proper oxygen concentration at the tissue level. Evidence supports our study finding that breathing exercises serve as pulmonary rehabilitation and aid in the recovery of COVID-19-positive patients.
We also found how our study respondents' home-based treatment is affected by social stigma, and this is not uncommon in other low and middle-income countries, including India, Pakistan, Nepal, and Indonesia [56-59]. The government needs to develop culturally sensitive strategies to improve knowledge of the community and reduce the mental stress of COVID-19 patients.
Based on the study findings, we would like to propose a few suggestions. Though this is a pilot study, in the large-scale study, the authors would like to collect substantial information on the use of medicines to contribute to revising the National COVID-19 Case Management guideline. More emphasis should be given to identifying a few safe medicines which can be prescribed for home-based treatment. Patients had to purchase medicine at a high cost as the pharmacists took undue advantage of the situation and made a considerable profit. The government should emphasize this aspect and strengthen supervision and monitoring so that patients do not suffer.
Regarding dietary supplements, we found that respondents consumed lots of lemon and citrus fruits; in this case, they should only take a few of the vitamins, particularly Vit. C and certain food, such as Nigella seeds. We also recommend making the use of breathing or respiratory exercise mandatory. Besides, all COVID-19-positive patients should receive psychological and mental support through counselling over the telephone to overcome the social stigma.
## V. LIMITATIONS
This study is not free from limitations. Although all four data collectors were doctors, they faced minor and major challenges as they collected data when the COVID-19 pandemic was at its highest transmission level. The major challenge was to collect the complete addresses and telephone numbers of COVID-19-positive cases as the authors used the snowball technique to collect this information. This difficulty may happen as interviewing anybody over the telephone when both ends people are not known to each other, it leads to a big challenge. Though the Public Health Expert Advisors provided support to collect the details of the patients, the study interviewers had to call the respondents 3 – 4 times to elicit information.
After putting in a substantial amount of effort, only 101 respondents joined the study. These respondents hesitated to give an interview over the telephone, even though the data collectors explained the background, purpose, and use of the information that would be collected for the study. We could not collect the information of the treating physicians as none of the respondents wanted to tell the name of the doctors who had given a prescription to the respondents. In the case of some female respondents, the male members of their families brought the medicines, and as such, they did not even know the name of their doctors. In addition, many respondents consulted more than one doctor, so they could not tell the name of a particular doctor. While collecting data, the data collectors felt that the respondents were taking more medicines than they mentioned, and it was not possible to collect the correct information. The data collectors faced challenges in collecting data from healthcare professionals during the in-depth interviews, as they did not have time to provide information while managing COVID-19 patients. As a result, we were only able to collect data from three doctors.
## VI. CONCLUSION
To our knowledge, this is the first study conducted in Bangladesh. This pilot study was conducted when the COVID-19 pandemic just started, and most of the science of the infection was not known clearly to the scientists. Many people were dying, and the element of fear was increasing day by day. Despite all odds, the respondents stayed at home, which is evidence of their helpless situation. Almost all respondents did not want to tell their neighbors, friends, and family members that they were infected and took medicines at home to avoid the social stigma, which was supported by the qualitative findings of healthcare professionals.
This pilot study provides necessary information on home management of COVID-19-positive Bangladeshi patients, which includes taking many food supplements. These findings also provided information on the feasibility of conducting a large-scale study, which needs to be conducted before making suggestions to revise the National COVID-19 Case Management Guideline about taking proper medicines, effective supplementary foods, and precautionary measures to counteract the deadly viral disease and to reduce morbidity and mortality.
The World Health Organization recently announced that COVID-19 is no longer a global public health emergency. However, the risk remains as new variants may emerge, which may cause new surges in morbidity and mortality. Before facing any new pandemic, Bangladeshi health policymakers need to develop an effective protocol for home-based treatment for asymptomatic and mild-symptomatic COVID-19 patients, who can stay at home during their illness & home quarantine period, and this paper will significantly contribute to this purpose.
List of Abbreviation
BDT: Bangladesh Taka
BHW: Bangladesh Health Watch
CDC: Centres for Disease Control and Prevention
COVID-19: Coronavirus Disease 2019
DGHS: Directorate General of Health Services
MERS-CoV: Middle East Respiratory Syndrome Coronavirus
MOHFW: Ministry of Health and Family Welfare
SARS-CoV: Severe Acute Respiratory Syndrome Coronavirus
SARS-CoV-2: Severe Acute Respiratory Syndrome Coronavirus-2
WHO: World Health Organization
### Statements and Declarations
Acknowledgment: The authors wanted to acknowledge and extend heartfelt gratitude to Prof. Saidur Rahman of Bangabandhu Sheikh Mujib Medical University (BSMMU), who supported the research team from the beginning until the end. With due regard, they wanted to mention the all-out support Dr. Khairul Islam of Water Aid provided at all stages of the study. The authors acknowledged with a deep appreciation of the financial support the Bangladesh Health Watch (BHW) provided to recruit junior doctors (Dr. Nawsheen Nazia, Dr. Shushmita Fairuz, Dr. Anika Tasnim, and Dr. Aneela Parvez) as dedicated interviewers for data collection, which helped the authors to get quality data and information. Finally, the authors would like to thank the respondents, who mainly were convalescing after their recovery from the infection with COVID-19 and provided the data without which authors could not complete the study.
Competing/Conflicts of interest: The authors declare that they have no conflict of interest to announce. They did not receive any financial or non-financial benefits or will receive from any party directly or indirectly related to the subject of this article; hence, they have no relevant financial or non-financial interests to disclose.
Funding: Authors received a small grant as financial support from the Bangladesh Health Watch (BHW) only to collect data.
Data availability: All the data that were collected during this study are presented in the paper.
Authors' Contributions: All authors contributed to the conceptualization of the study and research design. NJ was involved in the statistical analysis. MF & AJF completed the original draft writing. All authors reviewed and edited the writing for approving the final version of the manuscript.
Generating HTML Viewer...
References
59 Cites in Article
J Esparza (2020). Lessons from history: what can we learn from 300 years of pandemic flu that could inform the response to COVID-19?.
D Cucinotta,M Vanelli (2020). WHO declares COVID-19 a pandemic.
(2022). Weekly national respiratory infection and COVID-19 statistical report 14 December 2022.
De Wit,E Van Doremalen,N Falzarano,D Munster,V (2016). SARS and MERS: recent insights into emerging coronaviruses.
Agnieszka Zeidler,Tomasz Karpinski (2020). SARS-CoV, MERS-CoV, SARS-CoV-2 Comparison of Three Emerging Coronaviruses.
Su Park (2020). Epidemiology, Virology, and Clinical Features of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2; Coronavirus Disease-19).
Zeinab Abdelrahman,Mengyuan Li,Xiaosheng Wang (2020). Comparative Review of SARS-CoV-2, SARS-CoV, MERS-CoV, and Influenza A Respiratory Viruses.
Anis Chowdhury,K Jomo (2020). Responding to the COVID-19 Pandemic in Developing Countries: Lessons from Selected Countries of the Global South.
Ruth Waitzberg,Cristina Hernández-Quevedo,Enrique Bernal-Delgado,Francisco Estupiñán-Romero,Ester Angulo-Pueyo,Mamas Theodorou,Marios Kantaris,Chrystala Charalambous,Elena Gabriel,Charalampos Economou,Daphne Kaitelidou,Olympia Konstantakopoulou,Lilian Vildiridi,Amit Meshulam,Antonio De Belvis,Alisha Morsella,Alexia Bezzina,Karen Vincenti,Gonçalo Figueiredo Augusto,Inês Fronteira,Jorge Simões,Marina Karanikolos,Gemma Williams,Anna Maresso (2021). Early health system responses to the COVID-19 pandemic in Mediterranean countries: A tale of successes and challenges.
M Goyal,P Singh,K Singh,S Shekhar,N Agrawal,S Misra (2021). The effect of the COVID-19 pandemic on maternal health due to delay in seeking health care: experience from a tertiary center.
Pablo Radusky,Nadir Cardozo,Mariana Duarte,Solange Fabian,Emilia Frontini,Omar Sued,Ines Aristegui (2021). Mental health, substance use, experiences of violence, and access to health care among transgender and non-binary people during the COVID-19 lockdown in Argentina.
A Hasan,Subir Das,Muhammad Islam,Mohaimen Mansur,Md. Shawon,Rashedul Hassan,Mohammad Chowdhury,Md. Mondal,Quazi Mohammad (2021). Impact of COVID-19 on hospital admission of acute stroke patients in Bangladesh.
Weike Zhou,Aili Wang,Xia Wang,Robert Cheke,Yanni Xiao,Sanyi Tang (2020). Impact of Hospital Bed Shortages on the Containment of COVID-19 in Wuhan.
Minyoung Her (2020). Repurposing and reshaping of hospitals during the COVID-19 outbreak in South Korea.
Frank Schlosser,Benjamin Maier,Olivia Jack,David Hinrichs,Adrian Zachariae,Dirk Brockmann (2020). COVID-19 lockdown induces disease-mitigating structural changes in mobility networks.
Feng Liu,Meichang Wang,Meina Zheng (2021). Effects of COVID-19 lockdown on global air quality and health.
Fiona Imlach,Eileen Mckinlay,Jonathan Kennedy,Megan Pledger,Lesley Middleton,Jacqueline Cumming,Karen Mcbride-Henry (2022). Seeking Healthcare During Lockdown: Challenges, Opportunities and Lessons for the Future.
Bernhard Michalowsky,Wolfgang Hoffmann,Jens Bohlken,Karel Kostev (2021). Effect of the COVID-19 lockdown on disease recognition and utilisation of healthcare services in the older population in Germany: a cross-sectional study.
(2020). Home care for patients with COVID-19 presenting with mild symptoms and management of their contacts: interim guidance, 17.
Anil Kumar (2020). A Perspective on India’s Fight against COVID - 19.
Sayem Chowdhury,Md. Islam,Md. Haque,Nikkon Das,Sajjad Hossain,Marufa Heya,Md. Rahman (2022). Exploring the Health Care Seeking Behavior of Rohingya Community during COVID-19 Pandemic.
Syed Ahmed,Md Hossain,Ahmed Rajachowdhury,Abbas Bhuiya (2011). The health workforce crisis in Bangladesh: shortage, inappropriate skill-mix and inequitable distribution.
Al-Zaman Ms (2020). Healthcare crisis in Bangladesh during the COVID-19 pandemic.
A Jahangir (2020). Bangladesh.
Sriram Shamasunder,Seth Holmes,Tinashe Goronga,Hector Carrasco,Elyse Katz,Raphael Frankfurter,Salmaan Keshavjee (2020). COVID-19 reveals weak health systems by design: Why we must re-make global health in this historic moment.
David Asch,Natalie Sheils,Md Islam,Yong Chen,Rachel Werner,John Buresh,Jalpa Doshi (2021). Variation in US Hospital Mortality Rates for Patients Admitted With COVID-19 During the First 6 Months of the Pandemic.
D Asch (2021). COVID-19 Mortality and Stress to the Hospital System from High Patient Load-Reply.
Theodore Lytras,Sotirios Tsiodras (2022). Total patient load, regional disparities and in-hospital mortality of intubated COVID-19 patients in Greece, from September 2020 to May 2021.
Alessandro Soria,Stefania Galimberti,Giuseppe Lapadula,Francesca Visco,Agata Ardini,Maria Valsecchi,Paolo Bonfanti (2021). The high volume of patients admitted during the SARS-CoV-2 pandemic has an independent harmful impact on in-hospital mortality from COVID-19.
Andreas Chatzittofis,Maria Karanikola,Kyriaki Michailidou,Anastasia Constantinidou (2021). Impact of the COVID-19 Pandemic on the Mental Health of Healthcare Workers.
Juan Delgado-Gallegos,Rene Montemayor-Garza,Gerardo Padilla-Rivas,Héctor Franco-Villareal,Jose Islas (2020). Prevalence of Stress in Healthcare Professionals during the COVID-19 Pandemic in Northeast Mexico: A Remote, Fast Survey Evaluation, Using an Adapted COVID-19 Stress Scales.
Niall Galbraith,David Boyda,Danielle Mcfeeters,Tariq Hassan (2021). The mental health of doctors during the COVID-19 pandemic.
Abraar Karan,Rishi Wadhera (2021). Healthcare System Stress Due to Covid‐19: Evading an Evolving Crisis.
Benjamin Tan,Nicholas Chew,Grace Lee,Mingxue Jing,Yihui Goh,Leonard Yeo,Ka Zhang,Howe-Keat Chin,Aftab Ahmad,Faheem Khan,Ganesh Shanmugam,Bernard Chan,Sibi Sunny,Bharatendu Chandra,Jonathan Ong,Prakash Paliwal,Lily Wong,Renarebecca Sagayanathan,Jin Chen,Alison Ng,Hock Teoh,Cyrus Ho,Roger Ho,Vijay Sharma (2020). Psychological Impact of the COVID-19 Pandemic on Health Care Workers in Singapore.
Dilaver Tengilimoğlu,Aysu Zekioğlu,Nurperihan Tosun,Oğuz Işık,Onur Tengilimoğlu (2021). Impacts of COVID-19 pandemic period on depression, anxiety and stress levels of the healthcare employees in Turkey.
R Mcfee (2020). COVID-19 medical management including World Health Organization (WHO) suggested management strategies.
Rosa Da,R Mesquita,Francelino Silva Junior,L,Santos Santana,F,Farias De Oliveira,T,Campos Alcântara,R,Monteiro Arnozo,G (2021). Clinical manifestations of COVID-19 in the general population: systematic review.
Peong Park,Chang Kim,Yoon Heo,Tae Kim,Chan Park,Choong-Hyo Kim (2020). Out-of-Hospital Cohort Treatment of Coronavirus Disease 2019 Patients with Mild Symptoms in Korea: an Experience from a Single Community Treatment Center.
Steve Chaplin (2022). Paxlovid: antiviral combination for the treatment of <scp>COVID</scp> ‐19.
A Naidu,K Reddy,G Swetha,T Reddy,A Sudheer,B Pradeepkumar (2022). Pfizer's inventive Nirmatrelvir/Ritonavir (PaxlovidTM): Another arrow in the quiver against SARS-CoV-2.
Y Adebisi,N Jimoh,I Ogunkola,T Uwizeyimana,A Olayemi,N Ukor (2021). The use of antibiotics in COVID-19 management: a rapid review of national treatment guidelines in 10 African countries.
Sabeena Ahmed,Mohammad Karim,Allen Ross,Mohammad Hossain,John Clemens,Mariya Sumiya,Ching Phru,Mustafizur Rahman,Khalequ Zaman,Jyoti Somani,Rubina Yasmin,Mohammad Hasnat,Ahmedul Kabir,Asma Aziz,Wasif Khan (2021). A five-day course of ivermectin for the treatment of COVID-19 may reduce the duration of illness.
Hamza Ismaila,James Asamani,Virgil Lokossou,Ebenezer Oduro-Mensah,Juliet Nabyonga-Orem,Samuel Akoriyea (2021). The cost of clinical management of SARS-COV-2 (COVID-19) infection by level of disease severity in Ghana: a protocol-based cost of illness analysis.
C Demeke,A Woldeyohanins,Z Kifle (2021). Herbal medicine use for the management of COVID-19: A review article.
Junqing Huang,Gabriel Tao,Jingwen Liu,Junming Cai,Zhongyu Huang,Jia-Xu Chen (2020). Current Prevention of COVID-19: Natural Products and Herbal Medicine.
Benjamin Nuertey,Joyce Addai,Priscilla Kyei-Bafour,Kingsley Bimpong,Victor Adongo,Laud Boateng,Kareem Mumuni,Kenneth Dam,Emilia Udofia,Nana Seneadza,Benedict Calys-Tagoe,Edem Tette,Alfred Yawson,Sari Soghoian,Gideon Helegbe,Rajesh Vedanthan (2022). Home-Based Remedies to Prevent COVID-19-Associated Risk of Infection, Admission, Severe Disease, and Death: A Nested Case-Control Study.
Souad Belhaj,Lahcen Zidane (2021). Medicinal plants used to boost immunity and decrease the intensity of infection caused by SARS-COV-2 in Morocco.
Giacomo Di Matteo,Mattia Spano,Michela Grosso,Andrea Salvo,Cinzia Ingallina,Mariateresa Russo,Alberto Ritieni,Luisa Mannina (2020). Food and COVID-19: Preventive/Co-therapeutic Strategies Explored by Current Clinical Trials and in Silico Studies.
Magaly Villena-Tejada,Ingrid Vera-Ferchau,Anahí Cardona-Rivero,Rina Zamalloa-Cornejo,Maritza Quispe-Florez,Zany Frisancho-Triveño,Rosario Abarca-Meléndez,Susan Alvarez-Sucari,Christian Mejia,Jaime Yañez (2021). Use of medicinal plants for COVID-19 prevention and respiratory symptom treatment during the pandemic in Cusco, Peru: A cross-sectional survey.
Abdullah Noman,Taufique Joarder,Md. Islam,Md. Hossain,Samia Sadaf,Md. Noman,Nazmus Sakib,Jannatul Ekra,Md. Islam,Rima Meem,Samiron Sana,Mohammad Rahman (2021). COVID-19 recovery measures and use of medications among COVID-19 patients at home: A cross- sectional study in Bangladesh.
Tmz Uy,Mcb Miranda,Sjv Aro,Mev Uy (2020). Should steam inhalation be used in the treatment and prevention of COVID-19.
Tteesstt Iy Isolation and Precautions for People with COVID-19.
G Milne,S Xie (2020). The effectiveness of social distancing in mitigating COVID-19 spread: a modelling analysis.
Tina Wang,Brian Chau,Mickey Lui,Giang-Tuyet Lam,Nancy Lin,Sarah Humbert (2020). Physical Medicine and Rehabilitation and Pulmonary Rehabilitation for COVID-19.
Mab Siddiq,F Rathore,D Clegg,J Rasker (2020). Pulmonary Rehabilitation in COVID-19 patients: A scoping review of current practice and its application during the pandemic.
R Aacharya,A Shah (2020). Ethical dimensions of stigma and discrimination in Nepal during COVID-19 pandemic.
Nazish Imran,Hadia Afzal,Irum Aamer,Ali Hashmi,Bilquis Shabbir,Aftab Asif,Saeed Farooq. (2020). Scarlett Letter: A study based on experience of stigma by COVID-19 patients in quarantine.
A Islam,D Pakrashi,M Vlassopoulos,L Wang (2021). Stigma and misconceptions in the time of the COVID-19 pandemic: A field experiment in India.
Wahyu Sulistiadi,Sri Slamet,Nanny Harmani (2020). Management of COVID-19 Public Stigma in Indonesian Society.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Dr. Abu Jamil Faisel. 2026. \u201cManagement of COVID-19-Positive Bangladeshi Patients at Home: A Telephone-based Pilot Study\u201d. Global Journal of Medical Research - F: Diseases GJMR-F Volume 23 (GJMR Volume 23 Issue F6): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
The recent COVID-19 pandemic highlighted the challenges in healthcare settings due to the scarcity of medical resources like hospital beds and healthcare professionals to manage critical cases. During this critical period, healthcare professionals emphasized on saving lifethreatening cases, including moderate to severe COVID-19 cases, as they might need either ventilators or treatment in intensive care units. As a result, the national and international health policymakers, including WHO, suggested managing the suspected or confirmed COVID-19 patients without symptoms or having mild symptoms at home to reduce the burden on hospitals and trained healthcare professionals. Hence, we aimed to conduct a telephone-based pilot study to examine the feasibility before conducting a large-scale study on home-care treatment and management of the confirmed or suspected COVID-19 Bangladeshi patients, either asymptomatic or mild-symptomatic, during the home quarantine period.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.