


I. INTRODUCTION
Before the COVID 19 pandemic, Tuberculosis(Tb) had been the most fatal infectious disease in the world for many years. In 2021, according to the Global tuberculosis report 2022, an estimated 10.6 million people contracted TB and 1.6 million died from TB. Miliary tuberculosis occurs more frequently in extremes of age and those with a weakened immune system with non-specific symptoms that may be obscure till later in the disease. Since December 2019 the SARS-CoV-2 virus spread worldwide causing significant global public health and economic problems(1). It creates varied clinical phenotypes ranging from asymptomatic to life-threatening respiratory disease in all ages
Hormonal changes during pregnancy, especially oestrogen and progesterone changes is said to inhibit the immune function of lymphocytes and reduce the resistance of the mother to infections(2). This case report aims at highlighting the possibility of a lingering immune dysregulation in the post covid phase that may increase the susceptibility to infectious diseases.
II. CASE REPORT
A 40-year-old multipara, an unvaccinated healthcare worker of Indian origin working in a region non endemic to tuberculosis, developed mild COVID symptoms at 8 weeks of pregnancy which was confirmed to be a SARS-CoV-2 infection by quantitative real time polymerase chain reaction from throat swab. She was managed at a primary care facility with oral Azithromycin following which she had no significant symptoms. By the time she completed 31 weeks of gestation she developed a low-grade fever with occasional cough without expectoration. Over 4 weeks, it progressed to intermittent high-grade fever associated with chills and rigors and she was treated with multiple antibiotics from various facilities and she got admitted in our hospital for evaluation of persistent fever.
On admission she continued to have intermittent high-grade fever as high as with no symptoms of localizing value. She had PR of 130 and a BP of hg with RR of 28. The routine blood tests results showed that her white blood cell count was with neutrophil ratio and lymphocyte ratio , CRP was and ESR was . Peripheral Smear revealed normocytic normochromic blood picture with relative neutrophilia. Work up for infective causes including RT-PCR for SARS-COV 2, sputum CBNAAT for Tb and Mantoux test were negative. Work up for an autoimmune/inflammatory disease was also unremarkable. Respiratory examination revealed scattered crepitations over all lung fields, so a shielded Xray was taken which showed only the normal changes in pregnancy (Fig1). Transthoracic echocardiography and abdominal ultrasound were insignificant and MRI whole body diffusion study was attempted but the patient could not tolerate supine position due to dyspnea. The patient was empirically started on broad spectrum antibiotics. However, she continued to have continuous fever spikes daily with worsening shortness of breath. Over 48 hours following admission she developed dyspnea on rest and her oxygen saturation dropped from to with increased oxygen requirement from 2L/min via nasal prongs to 6L/min via a simple face mask.
Considering the deterioration in her general condition, an informed decision to terminate the pregnancy was made as the patient was in her third trimester and had crossed 35 completed weeks. Induction and vaginal delivery were preferred over caesarean delivery due to concerns over delayed wound healing as an infective pathology was still among the differentials. She continued to be febrile and was started on oral misoprostol 25 mcg. After 2 doses she started having mild uterine contractions and labour was augmented with oxytocin. As the intensity of her contractions increased, she started desaturating, her saturation dropped to which mandated an emergency intubation. Category I LSCS was performed and she delivered a baby with APGAR 6 at 1' requiring bag and mask ventilation. Her placenta had to be manually removed since it was focally adherent and was sent for histopathology. After termination of pregnancy, fever spikes that had persisted for over a month ceased.
She developed moderate adult respiratory distress syndrome (ARDS) and was put on mechanical ventilation, she had elevated plateau pressures and required high PEEP of 14 and 100 percent Fio2 to ventilate and maintain adequate oxygenation. She was initiated on volume control mode - low tidal volume ventilation. The patient was initiated on Methylprednisolone in view of worsening ARDS. Prone ventilation could not be done due to post op status and drains in situ. Post operative chest radiographs revealed infiltrates suggestive of miliary mottling (fig1). Fundoscopy showed fine punctuate choroid tubercles suggestive of TB retinal manifestations. Her IGRA was sent which came positive. Initial bronchoalveolar lavage (BAL) cultures and smear for acid fast bacilli were still negative. Bone marrow biopsy was also done but was negative for miliary TB.
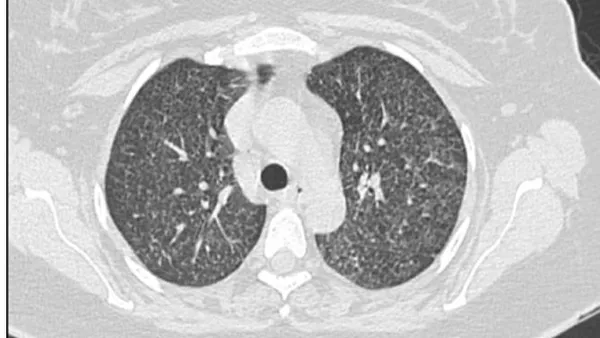
On the third post operative day, she was initiated on anti-tubercular therapy with a combination of Rifampicin, Isoniazid, Pyrazinamide, Ethambutol and Pyridoxine. Repeat BAL smear for acid fast bacilli was positive after 48 hours of initiating antitubercular therapy. CBNAAT done on the same sample was positive for Mycobacterium tuberculosis and there was no evidence of Rifampicin resistance. But she developed mild drug induced liver injury and anti-tubercular therapy was modified. The baby was also initiated on Rifampicin, Isoniazid and Pyridoxine. Soon, infiltrates on chest radiograph started improving, oxygen requirement and PEEP reduced with improvement in peak pressures and plateau pressures. The patient continued to improve, tolerating pressure support ventilation and was extubated on post operative day 8. Regular antitubercular medications were restarted following normalization of liver function tests. She also developed thrombosis of deep veins of the calf, popliteal vein and superficial femoral vein which required therapeutic anticoagulation. CT thorax was done on post operative day 20 and it revealed diffuse distribution of miliary nodules in bilateral lung parenchyma with conglomeration of few nodules in the left apico-posterior segment (fig 2).
The placental biopsy showed early crowding of the vessels with congestion of the villi, focal villous agglutination and intramural fibrin deposition within wall of large foetal vessel with calcification. There was also increased focal perivillous fibrin deposition occupying more than of the total parenchyma, intervillous thrombi, along with acute villitis and intervillositis with neutrophilic abscess and necrosis, but there were no bacilli on Ziehl-Neelsen stain.
She was discharged after 31 days of hospital stay and resumed activities of daily living. She is under close follow up on an outpatient basis and is afebrile without limitation of ordinary physical activity.
III. DISCUSSION
The change from a cell mediated immunity to a humoral immunity along with the Th2 bias seen in pregnancy affects the systemic immune responses to infection and increases vulnerability to coronaviruses and Mycobacterium Tuberculosis(3). There has also been speculations that SARS-CoV-2 infection may increase the propensity for an active Tb infection(4). Moreover following a COVID-19 infection it is now speculated that one-fifth of patients have long term persistence of symptoms despite the apparent clearance of infection which has been hypothesized to be due to persistence of virus or alterations in humoral immunity(5).
In this case we have a woman in her third trimester without a history of prior Tb infection developing military tuberculosis that rapidly progressed to ARDS which is a rare fatal presentation of military Tb(6). During pregnancy the diagnosis of Tb can be a challenge as symptoms maybe masked by the pregnancy symptoms and also due to limited imaging(7). Her initial tests for tuberculosis were negative except a positive IGRA. It was the presence of choroid tubercles seen on the fundus that helped clinch the diagnosis of miliary Tb(8), then again she had a negative bone marrow biopsy report.
The two most intriguing factors in this case were the rapid resolution of her febrile episodes soon after the caesarean and the pathology of the placenta. The placenta showed features of maternal and fetal vascular malperfusion with increased focal perivillous fibrin deposition and additionally acute villitis and intervillositis with neutrophilic abscess and necrosis These features are suggestive of a covid placentitis as studies on SARS-CoV-2 infected placentas have shown increased rates of maternal vascular malperfusion features and intervillous thrombi, suggesting an abnormal maternofetal circulation(9). Though miliary tuberculosis can cause changes in the placenta with a cluster of acute villitis and intervillitis, an abundance of acid-fast mycobacteria has been reported(10) which was absent in our case.
The persistence of placental changes due to a mild COVID-19 infection could be an indicator of a persistence of other systemic changes following the infection. Further studies to explore this concept would help in determining the vulnerability of pregnant women to infectious diseases which would help in timely diagnosis and treatment to prevent the incidence of morbidity and mortality from these diseases in the post pandemic era.
ACKNOWLEDGEMENTS
We thank Dr Megha Isac for her contributions in the interpretation of data and material support.
Conflict of Interest
The authors declare that they have nothing to disclose.



