## I. INTRODUCTION
affect social participation Cardiovascular diseases (CVD) are a global problem in adulthood and old age due to the inversion of the population pyramid [1,2]. According to the International Classification of Functioning, these CVDs can cause mainly motor deficiencies due to amputation, paresis, plegia, visual, auditory, cognitive, language, and disabilities when they affect social participation [3,4,5,6,7]. CVDs are those diseases that arise from physiologic disturbances of the heart and blood vessels and include coronary heart disease, stroke, peripheral vascular disease, heart failure, and heart disease; these are more prevalent in Western consumer societies, due to common preventable risk factors such as arterial hypertension, alcohol consumption, dyslipidemia, diabetes mellitus, obesity, smoking, sedentary lifestyle, high salt intake; inadequate therapeutic adherence and hypovitaminosis D[8.9,10,11,12,13,14,15,16,17,18].
The disability affects the nutritional balance, which depends on the balanced intake of food and its physiological, biochemical, and metabolic use, and leads to malnutrition (body mass index less than 25 kg/m2) due to low intake of macronutrients and vitamins; or overweight (25-29.9 kg/m2) and obesity (greater than 30kg/m2) due to associated complications such as a sedentary lifestyle, sarcopenia, swallowing disorders, among others [19,20,21,22,23]. Malnutrition increases the risk of osteoporosis, falls, fractures, sarcopenia, limited transfers, immobilization, spasticity, joint contractures, pressure ulcers, cognitive deficits, institutionalization, prolonged hospital stay, high health cost, feeding difficulties, dysphagia, use of a nasogastric tube, loss of well-being, years of productive life lost due to disability; mood disorder, low self-esteem, poverty, social exclusion and mortality [4,9,12,13,23,24].
In the world, close to 1,000,000,000 people have disabilities, and 200,000,000 have functional and nutritional alterations; this situation is more prevalent in southern countries $^{2}$; the region of the Americas reports high rates of productive years of life lost due to disability due to CVD [25] and mortality due to CVD with 18,000,000 per year (33%) [26]. In Colombia, by 2021, 1,555,708 people with disabilities were reported [27], and the Situational Chamber attributes 15% of morbidity in this population to nutritional and endocrine-metabolic pathologies; there are no nutritional classification data [28].
The World Health Organization (WHO) invites us to understand this problem through the approach of social determinants in health [29,30,31,32,33]. Colombia has implemented this guideline through the community-based rehabilitation strategy [7,34] although a preventive nutritional evaluation is necessary [4,29,35,36,37] under the approach of specialties such as family medicine and nutrition based on the care model primary care in health, the ecological theory of systems and the regulatory framework of health care for people with disabilities[7,38,39,40,41,42,43,44,45,46]. The study's objective was to describe the nutritional status of the adult population with deficiencies and disability associated with CVD between January and December 2021, based on the hypothesis that patients with disability associated with CVD frequently have malnutrition.
## II. MATERIALS AND METHODS
An observational, cross-sectional, descriptive quantitative study was carried out. The total population was 11 adults with deficiencies or disabilities secondary to CVD. One person was not included because informed consent was not requested. The patients were located by the databases of the mayor's office and the Motavita Health Center. The data was collected in the period from January to December 2021.
Inclusion criteria: people with deficiencies and disabilities secondary to CVD according to the domains of the International Classification of Functioning (mobility, hearing, vision, cognitive, language, and personal care); age from 29 to 59 years, inhabitants of Motavita-Colombia.
Exclusion criteria: Patients with terminally ill, in palliative care, with a gastrostomy tube for enteral nutrition, not signing the informed consent to participate in the research.
Variables and data analysis: 1. Nutritional practices: there are no validated questionnaires on nutritional requirements for adults; therefore, a structured nutritional questionnaire (designed by the researcher) was prepared and applied, validated after a pilot study.
2. Washington Questionnaire, to define the type of disability and functional limitations 3. Anthropometric
nutritional, medical assessment, assessed with body mass index and percentage of body fat (CUN-BAE formula and skin folds); and physical test evaluated with the short physical performance battery (SPPB). For the analysis, a calibrated tape measure, adipometer, and digital scale, a chair, and a stopwatch were used.
4. Sociodemographic.
5. Cardiovascular risk factors and CVD. To carry out the descriptive statistical analysis, the Excel program was used. The variables were classified, and the measures of central tendency, dispersion, relative frequencies (\%) for the qualitative variables, and standard deviations (SD) for the quantitative ones were calculated.
## III. ETHICAL CONSIDERATIONS
This research was previously authorized by the Ethics Committee of the Pedagogical and Technological University of Colombia, following medical bioethical principles, Colombian regulations (Resolution 008430/1993, article 6, literal e), and confidentiality regulated by the Law on Data Protection (Law 1581/2012, Decree 1377/2013) [47,48,49]. All participants were informed about the objectives, methodology, risks, voluntary and anonymous participation, and the right to withdraw from the study at any time.
## IV. RESULTS
Ten adults with deficiencies and secondary disability to CVD from Motavita-Colombia were included during the collection period. The sociodemographic characteristics showed a median age of 58 years (48-59 years), female $(80\%)$, living in rural areas $(70\%)$, unemployed $(70\%)$, with subsidized health insurance $(60\%)$ and with a low educational level, being primary the most frequent level $(80\%)$. Secondary the highest level reached $(20\%)$. Table 1 describes other sociodemographic characteristics.
Table 1: Sociodemographic characteristics of the study population.
<table><tr><td colspan="2">Variable</td><td>Absolute frequency (n= 10)</td><td>Relative frequency (%)</td></tr><tr><td rowspan="2">Civil status</td><td>Single</td><td>2</td><td>20%</td></tr><tr><td>Married</td><td>7</td><td>70%</td></tr><tr><td></td><td>Divorced</td><td>1</td><td>10%</td></tr><tr><td rowspan="2">Economic income</td><td>Own income</td><td>4</td><td>40%</td></tr><tr><td>Family income</td><td>5</td><td>50%</td></tr><tr><td></td><td>Subsidy income</td><td>1</td><td>10%</td></tr><tr><td rowspan="3">Living place</td><td>Own living place</td><td>6</td><td>60%</td></tr><tr><td>Family living place</td><td>3</td><td>30%</td></tr><tr><td>Geriatric home</td><td>1</td><td>10%</td></tr><tr><td rowspan="2">Social security</td><td>Stated subsidy</td><td>9</td><td>90%</td></tr><tr><td>Contributory</td><td>1</td><td>10%</td></tr></table>
The most frequent CVD risk factors were arterial hypertension (100%) and dyslipidemia (60%); Table 2 shows other CVD risk factors. The entire population had stroke-type CVD, and some patients had aortic aneurysm (10%) and peripheral arterial disease (10%). With the Washington questionnaire, it was found that all the patients can execute the functions of walking, vision, hearing, language, and mental processes; personal care and communication, although they do it with difficulty; the cognitive (100%) and visual (50%) domains being the most affected (Figure 1). In the levels of independence to carry out the feeding process, no patient requires total assistance, and the highest proportion can feed themselves (80%).
Table 2: CVD risk factors in the study population.
<table><tr><td colspan="4">CVD risk factors</td></tr><tr><td colspan="2">Variable</td><td>Absolute frequency (n=10)</td><td>Relative frequency (%)</td></tr><tr><td rowspan="2">Type 2 Diabetes</td><td>Yes</td><td>1</td><td>10%</td></tr><tr><td>Not</td><td>9</td><td>90%</td></tr><tr><td rowspan="2">Chronic kidney disease</td><td>Yes</td><td>2</td><td>20%</td></tr><tr><td>Not</td><td>8</td><td>80%</td></tr><tr><td rowspan="2">Previous problematic alcohol use</td><td>Yes</td><td>3</td><td>30%</td></tr><tr><td>Not</td><td>7</td><td>70%</td></tr><tr><td rowspan="2">Ex -smoking</td><td>Yes</td><td>1</td><td>10%</td></tr><tr><td>No</td><td>9</td><td>90%</td></tr></table>
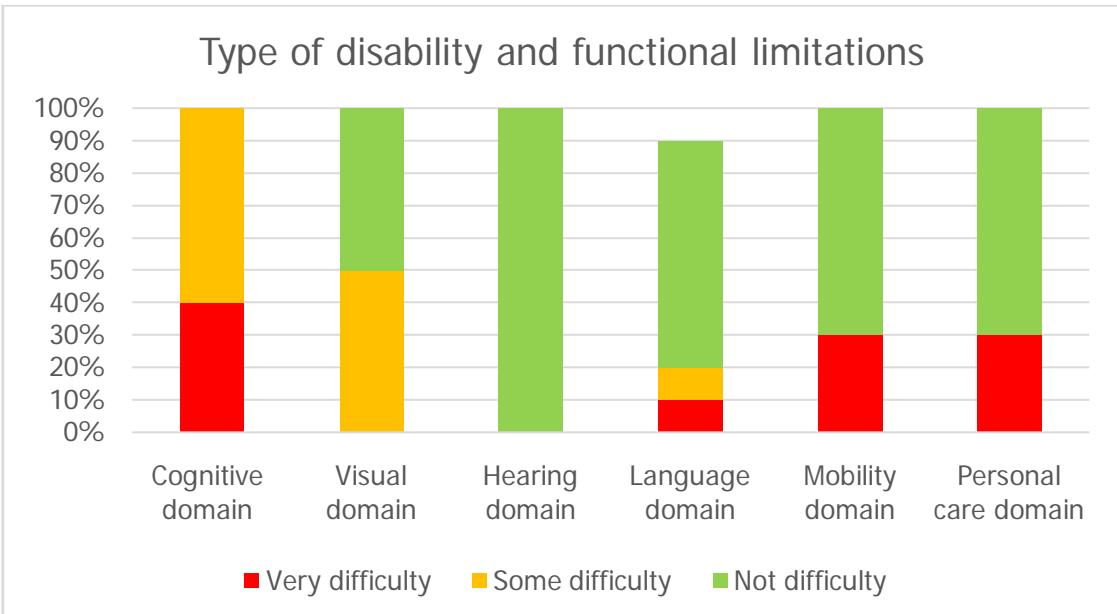 Figure 1: Washington scale of domains and functional limitation in the target population.
Source: own elaboration, direct collection.
At the healthy practices, the nutritional test found an inappropriate intake of macro and micronutrients (Figure 2) and a dietary regimen based on high consumption of carbohydrates and lipids (100% and 90%, respectively) and low protein consumption (10%). In addition, the consumption of calcium, iron, and fiber did not meet the nutritional requirements in the majority of the population (80%, 90%, and 100% respectively), a similar situation with vitamins, since the most significant proportion did not meet the nutritional requirements of vitamins A either. (80%) D, E, K (90%), B and C (100%); In addition, the most significant proportion does not meet the daily requirements for water consumption (80% distributed as follows: 50% consume less than 30ml/kg/day and 30% consume more than these requirements). Some patients consume drugs that induce overweight (30%).
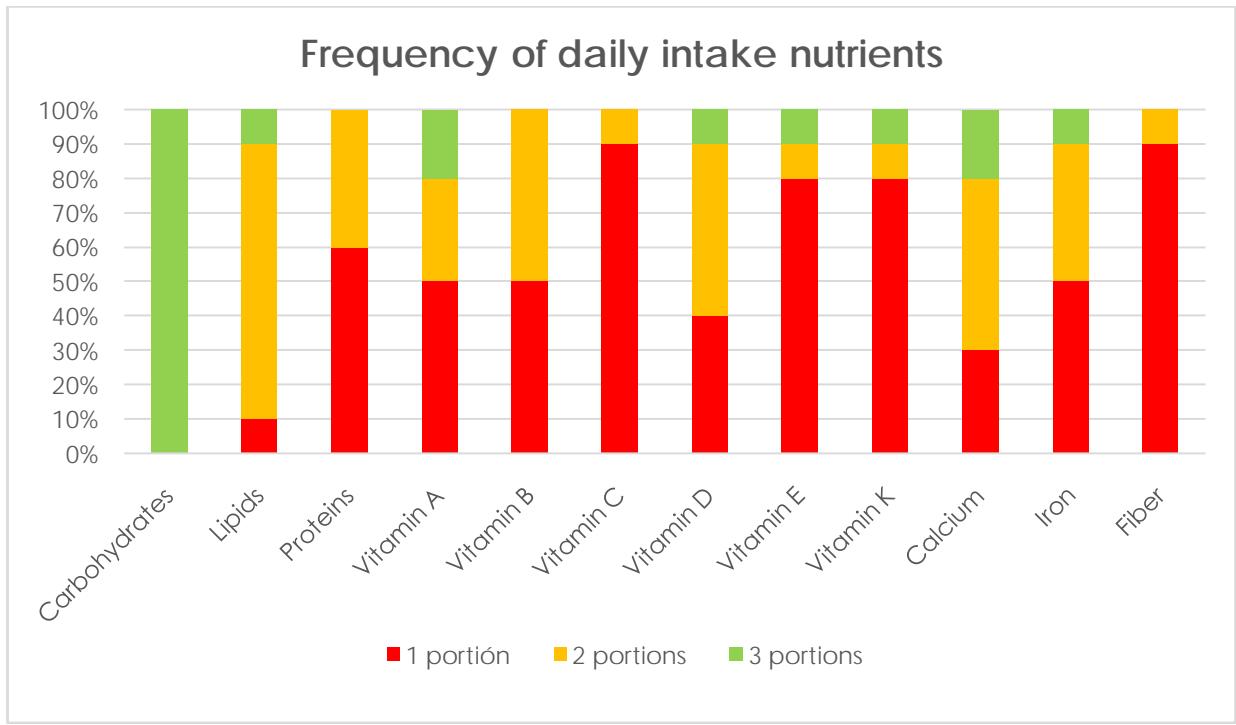 Figure 2: Frequency of daily consumption of nutrients in the target population.
Source: own elaboration, direct collection.
In the anthropometric tests, the average weight was $67.02 + / - 8.56$ (range: 53 to $81.5\mathrm{kg}$ ), and the median height was 1.58 (range: 1.48-1.62), the median BMI was overweight (BMI: 27.59; range: 20.2-32.65), and the median percentage of body fat by CUN-BAE formula and by summation of skin folds was obesity (CUN-BAE: 40.32; range: 24.9-46.29; skinfolds: 39.05; range: 24.7-45.7). In addition, the majority of patients had malnutrition of the sarcopenic obesity type in all the tests applied (Figure 3); With the Sheldon somatotype, most patients were classified as having an endomorph profile $(70\%)$, followed by an ectomorph profile $(20\%)$; with BMI, the highest proportion was overweight $(30\%)$ or obese $(30\%)$; with the CUN-BAE formula and with skin folds, the majority of patients had a high $(40\%)$ and very high $(50\%)$ percentage of body fat; with waist circumference, the highest proportion had abdominal obesity $(90\%)$ and with calf circumference, half of the population had sarcopenia.
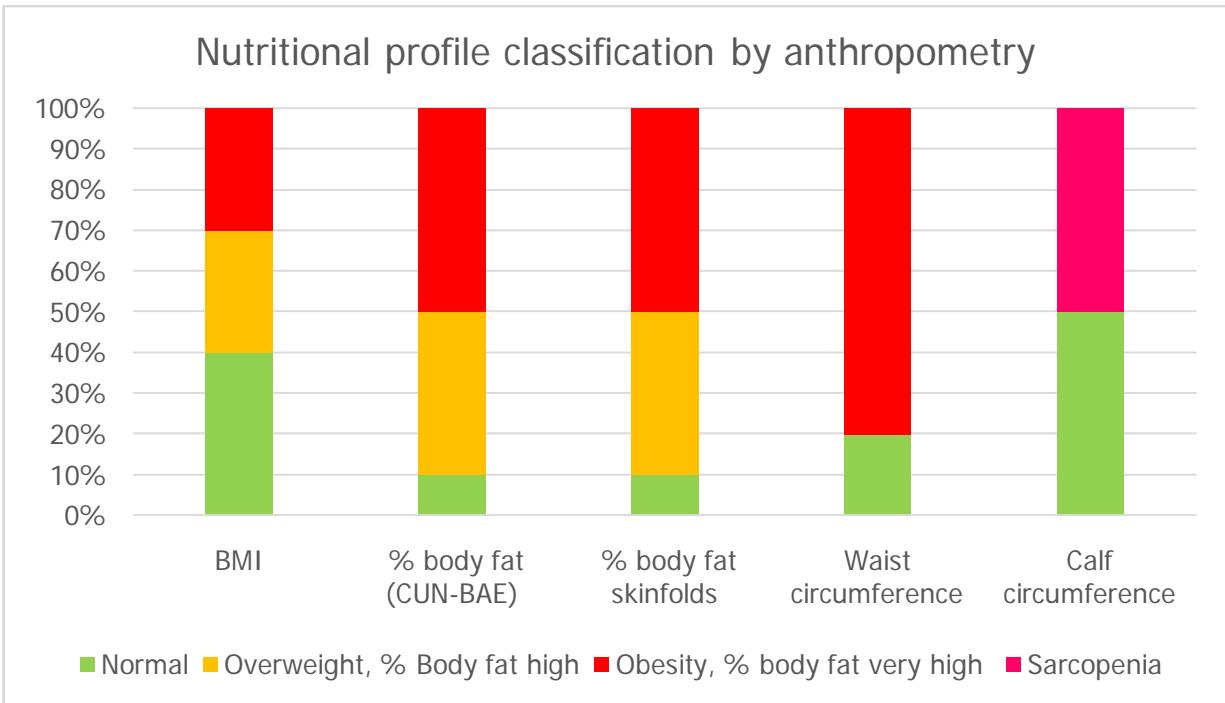 Figure 3: Classification of the nutritional profile of the population studied by anthropometry.
Reference values: \*\*BMI: body mass index. \*\*WHO criteria for BMI classification: malnutrition: $< 18.5\mathrm{kg / m2}$, normal weight: 18.5-24.9 kg/m2, overweight: 25-29.9 kg/m2, grade I obesity: 30- 34.9 kg/m2, grade II obesity: 35-39.9 and grade III obesity: $>40$ kg/m2. \*\*Body fat percentage (by CUN-BAE formula and by skinfolds): In women aged 40 to 59: low: less than $23\%$; normal: 23-33.9%; high: 34-39.9%; very high: $>40.0\%$. In men 40 to 59 years: low: $< 11\%$; normal: 11-21.9%; high: 22-27.9%; very high: $>28.0\%$. [50,51,52,53,54] Source: Own elaboration. Information adapted from direct collection To evaluate physical performance, the short physical performance battery was applied, which allows classifying the degree of limitation as minimal (10-12 points), mild (7-9), moderate (4-6), or severe (0- 4), and optimal muscle status (>8 points) or sarcopenia (<8). [53,55,56,57,58,59]. In this study, the average score was $7.7 + / - 2.3$ (range: 3-10); the highest proportion of physical limitation was mild $(40\%)$ and minimal $(30\%)$ and the least amount of those affected had severe physical restriction $(10\%)$; in addition, half of the population had sarcopenia. Although the most significant proportion reported doing some daily physical activity $(70\%)$, none of them have a structured exercise plan or comply with the physical activity recommendations of the American College of Sports Medicine. In addition, no patient had nutritional consultation or received nutritional supplements in the last year.
Finally, a nutritional care plan was prepared for each patient to improve the situation of sarcopenic obesity and reduce the risk of anemia, osteoporosis, and metabolic dysfunction; this included the intervention of all the variables studied based on the social determinants of health found, the fundamental nutritional requirements (the healthy plate), care practices for the promotion and maintenance of nutritional health and general recommendations for physical activity of safely following the current algorithm of the American College of Sports Medicine.
## V. DISCUSSION
In this study, obesity-type malnutrition (60-90%) sarcopenic (50%) was found in the majority of patients with all the tests applied and nutritional regimens that exceeded the nutritional requirements of carbohydrates (100%) and lipids (90%)., with a deficit in protein intake (60%) micronutrients and vitamins [46,60,61], which increases the risk of musculoskeletal and endocrine-metabolic complications [62,63,64,65]; This percentage is higher compared to the result of the meta-analysis by Su Y et al. (2020), in which they compiled cross-sectional and observational studies that recorded 42% of sarcopenic obesity [66].
For the analysis of the results, the theory of social determinants in health was used; which are the conditions in which a person is born, lives, and develops. In individual sociodemographic determinants, the median age was 58, and the most affected sex was female (80%). These data are similar to the results of the European prospective study Mini Nutritional Assessment International Group et al., which registered many female patients with malnutrition (75.2%) [67]. This gender behavior may be due to the culture of self-care, which is higher in women than in men, as evidenced by Wallis (2017) in his cohort study [68] and Alvarez (2020) in their review article [69]; where they describe that men have less self-care and consult health services late, which decreases the survival rate
According to the meta-analysis by Gao et al. (2021) [70], the most critical risk factors for CVD are arterial hypertension $(\mathrm{OR} = 0.98,95\% \text{ CI: } 0.84 - 1.14)$ and hyperlipidemia $(\mathrm{OR} = 1.14,95\% \text{ CI: } 0.89 - 1.47)$, similar results to those found in this study (arterial hypertension: $100\%$; dyslipidemia: $60\%$ ). Other factors described were diabetes $(\mathrm{OR} = 1.40,95\% \text{ CI: } 1.18 - 1.66)$, chronic kidney disease $(\mathrm{OR} = 2.52,95\% \text{ CI: } 0.19 - 33.30)$, and smoking $(\mathrm{OR} = 1.20,95\% \text{ CI: } 1.10 - 1.21)$; all of them present in the population object of this study[71,72,73,74,75,76,77,78,79,80].
Of the CVDs, stroke was the most frequent (100%), and there was a low percentage of aneurysmal disease (10%) and peripheral arterial disease (10%); there were no patients with disability due to coronary artery disease; these data are heterogeneous compared to the literature [81,82,83,84,85,86], and those of the PAHO observatory (2021), which indicates that in 2019, in Colombia, stroke caused 625.5 years disability-adjusted life per 100,000 inhabitants; and ischemic coronary artery disease caused 1327.7 disability-adjusted life years per 100,000 inhabitants [87].
The type of disability is a risk factor for malnutrition [88]; In this study, with the Washington questionnaire, the most affected domains were cognitive (100%) and visual (50%); percentages higher than those found in the US Framingham cohort study by Hayes et al., who evaluated 220 stroke survivors and found a large proportion of patients with cognitive deficit such as aphasia (65%) followed by motor deficit (50%) and sensory (15%), which was one of the least affected domains [89]; however, the meta-analysis by Doyle et al., also reported a large percentage of involvement of the sensory domain (94%) in CVD survivors [90]. Cognitive sequelae limit understanding of the nutritional therapeutic plan, and visual and motor sequelae limit its execution [91].
In the anthropometric profile, malnutrition due to excess kilocalories was diagnosed with all the tests used. However, the rate was higher with waist circumference (90%: abdominal obesity), the percentage of body fat with the CUN-BAE formula and skinfolds (90%: high or very high) and lower with the Sheldon somatotype (70%: endomorph) and BMI (60% overweight or obese); these differences are similar to those found in the prospective cohort study by XiangfengCong et al. (2022), which reports 11.8% obesity with BMI (95% CI: 11.2-12.3%) and 40.1% obesity with waist circumference (95% CI: 39.2-41.0%) [92]. The percentage of muscle mass is a protective factor for cardiovascular disease, while the percentage of body fat is a risk factor for cardiovascular disease [51,54,92,93]; these percentages should be investigated in the nutritional medical consultation. In this study, participants had a higher risk nutritional classification with percentage body fat, calf circumference, and abdominal circumference compared with BMI.
With the circumference of the calf and short battery of physical performance; sarcopenic obesity was diagnosed in $50\%$ of the population; a percentage similar to the meta-analysis by Su Y et al. (2020) of cross-sectional and observational studies, which recorded a similar prevalence broken down by sex in women $(39\%; 95\% \text{Cl}: 25\%-55\%)$ and men $(45\%; 95\% \text{Cl}: 28\%-62\%)$ [66] Two factors that explain sarcopenia were identified: the metabolic state after the stroke and the low protein intake in the majority of the population studied $(90\%)$ [50,53,55,56,62,94,95]; these data are related to the meta-analysis by Negm (2022), which concludes that an adequate dietary protein intake or protein supplementation are the most effective interventions to improve muscle strength and physical performance in sarcopenia [96].
With the short battery of physical performance, a physical limitation was determined in all the patients; and it was mild (40%) and minimal (30%) in the majority, and to a lesser extent severe (10%); these data show one face of nutritional condition [59], as concluded in the cross-sectional study by Carvalho (2022), in which the risk of malnutrition was associated with low total scores with the short battery of physical performance (OR = 0.682, P = 0.011) [83]. In addition, a sedentary lifestyle causes sarcopenia due to decreased musculoskeletal mechanical stimulation, hypovitaminosis D, and osteoporosis [12,36,97,98,99]; In this study, the majority of participants reported doing daily physical activity such as short walks (70%), but none of them met the recommendations of the American College of Sports Medicine, the WHO, and didn't have a structured exercise plan [100,101,102,103,104, 105,106,107,108]. One strategy to improve physical performance is a structured exercise plan, according to the meta-analysis by Negm (2022), which included 3649 participants and 11 interventions and concluded that mixed exercise (aerobic and resistance) was the most effective intervention (93.94%) to increase muscle mass and physical performance [96].
In the interpersonal determinants, the study found a low educational level (80%), which limits knowing nutritional requirements and adopting good eating practices and leads to malnutrition. Figueroa (2020), recognizes in their study that people with a low educational level (71%), little knowledge about healthy eating (78.4%), food groups (59.8%), exercise (50.5%), and comorbidities (58.8%), are more likely to be malnourished [109]; hence the importance of educating the patient about healthy nutritional and physical activity behaviors [110,111,112,113,114,115,116]. To achieve nutritional health goals, a family support network is necessary [117,118,119]. In this study, the most significant proportion had a household (70% married); this resource was investigated in the Australian study by Curryer (2018), and it was concluded that three characteristics must be identified for family support:
centrality, the experience of self-determination and limitations for selection and control, in addition, the environment of trust allows receiving guidance on choice and decision-making, which favors health objectives [120].
In addition, the doctor-patient-family relationship makes it possible to achieve these nutritional objectives [121]. In this study, no patient had nutritional consultation or received nutritional supplement formulation in the last year, although most have free health insurance (60%). Some causes described in the literature for this situation are a distant doctor-patient relationship, or perception of discrimination, as Moscoso refers. (2018), in their cross-sectional study, in which people with disabilities with a perception of discrimination avoid consulting health care services (78.8% in discriminated against vs. 86.1% in non-discriminated; PR = 1.15; 95% CI: 1.04-1.28) [122]
The level of independence to execute the feeding process determines the possibility of consuming food on time; in this study, no patient required total assistance, and the most significant proportion could feed themselves (80%); however, some require assisted feeding (10%); therefore, they have a greater need for family integration into the care plan [118, 120]. This degree of dependency is explained by Andrade Q. (2022) in his observational study, and he concludes that functional capacity is inversely proportional to the degree of family dependency; there is a mild dependence (100%) when the functional capacity is minimally compromised and severe (95.83%) when the usableability is highly compromised (p<0.001) [118]. Functional dependence and social restriction affect self-esteem and the sphere emotionally and negatively influences the nutritional situation[123,124,125,126,127, 128,129,130,131,132].
In the contextual determinants, people with disabilities have restricted participation [133,134,135], and a higher poverty rate [136,137,138,139, 140,141,142,143], this study shows these consequences in unemployment (70%) and economic dependence (60%), results similar to Mitra's findings (2018), where 20 studies from 10 high-income countries were analyzed and it was determined that the health cost is higher in people with severe disabilities or when they live alone or belong to small households, because they are economically dependent [144,145]. Pinilla (2018), studied the Multidimensional Poverty Index in families with and without people with disabilities in five Latin American countries and found that in all countries the households of people with disabilities had a higher incidence, intensity and levels of multidimensional poverty, due to the high health cost and economic dependence [146]. This limits the acquisition of nutrients, for this study there was a protein deficit (90%); calcium (80%), iron (90%), fiber (100%) and vitamins A (80%) D, E, K (90%), B and C (100%); all of them of high economic value within the family basket [4,60,63,147,148,149,150].
A limitation of the study is the sample size, because this limit making statistical association and calculating prevalence. However, the findings correspond to the complete population to investigate according to inclusion and exclusion criteria. This study differs from the case series because its intervention was based on diagnostic exploration.
## VI. CONCLUSIONS
This innovative study concludes that the adult population with disabilities secondary to CVD has a profile of sarcopenic obesity with all the diagnostic tools applied, with excess kilocalories and deficit in the consumption of proteins, micronutrients, vitamins, fiber, and water; it also makes it possible to demonstrate the expression of vulnerability of the population with disabilities.
To evaluate the nutritional condition in patients with disabilities, it is necessary to use pragmatic outpatient nutritional tools, such as abdominal circumference or the CUN-BAE formula, to assess abdominal fat percentage and calf circumference or the short physical performance battery to investigate sarcopenia. In addition, a comprehensive approach based on the social determinants model contributes to creating nutritional care plans adjusted to personalized needs to prevent the appearance of malnutrition, detect it in time, and intervene to avoid musculoskeletal, joint, metabolic, endocrine and cardiovascular complications. The family physician must identify individual, interpersonal, and contextual problems, establish a management plan, provide health education for the patient and their family, and locate family resources to strengthen behaviors to promote and maintain nutritional and mental health. In addition, risk factors must be identified and intervened to avoid restricting the patient's social participation.
It is the job of the state to implement policies, strategies (such as community-based rehabilitation), and social inclusion plans to improve population nutritional health since there is a social debt, taking into account that aging with high allostatic load in people from countries "from the south" is an expression of the geographical pattern of human development and a social disadvantage reflected in people with disabilities.
Competing interests: None declared
Data availability statement All data relevant to the study are included in the article or uploaded as supplemental information.
Generating HTML Viewer...
References
131 Cites in Article
(2021). Heart Disease and Stroke Statistics.
Vivienne Chuter,Frank Quigley,Patrik Tosenovsky,Jens Ritter,James Charles,Jane Cheney,Robert Fitridge (2022). Australian guideline on diagnosis and management of peripheral artery disease: part of the 2021 Australian evidence‐based guidelines for diabetes‐related foot disease.
D Arnett,R Blumenthal,M Albert (2019). Correction to: 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.
García Alfonso,C,Martínez Reyes,A García,V,Ricaurte Fajardo,A Torres,I,Coral (2019). Diagnosis and Treatment of Acute Ischemic Stroke: An Update.
Angélica Toro Cubides (2018). Análisis crítico de la implementación de la resolución del ministerio de salud 3280 del 2018 y su ruta integral de atención en salud para la población materno perinatal (RIAS) en la humanización del trabajo de parto y parto.
Martínez Pérez,Florencio Héctor (2015). Comunicación, desempeño laboral y discapacidad auditiva.
K Bowen,V Sullivan,P Kris-Etherton,K Petersen (2018). Nutrition and cardiovascular disease-an update.
(2022). 1. Improving Care and Promoting Health in Populations: <i>Standards of Medical Care in Diabetes—2022</i>.
Frank Visseren,Franc¸ois Mach,Yvo Smulders,David Carballo,Konstantinos Koskinas,Maria Back,Athanase Benetos,Alessandro Biffi,Jose´-Manuel; Boavida,David Capodanno,Bernard Cosyns,Carolyn Crawford,Constantinos Davos,Ileana Desormais,Emanuele Di Angelantonio,Oscar H; Franco,Sigrun; Richard Halvorsen,F Hobbs,Monika Hollander,Ewa Jankowska,Matthias Michal,Simona Sacco,Sattar,; Naveed,Lale Tokgozoglu,Serena Tonstad,Konstantinos Tsioufis,Ineke; Van Dis,Isabelle Van Gelder,Christoph Wanner,Bryan Williams (2022). Task Force Members. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies. With the special contribution of the European Association of Preventive Cardiology (EAPC).
Antonio Pelliccia,Sanjay Sharma,Sabiha Gati,Maria Bäck,Mats Börjesson,Stefano Caselli,Jean-Philippe Collet,Domenico Corrado,Jonathan Drezner,Martin Halle,Dominique Hansen,Hein Heidbuchel,Jonathan Myers,Josef Niebauer,Michael Papadakis,Massimo Piepoli,Eva Prescott,Jolien Roos-Hesselink,A Stuart,Rod Taylor,Paul Thompson,Monica Tiberi,Luc Vanhees,Matthias Wilhelm (2020). 2020 ESC Guidelines on Sports Cardiology and Exercise in Patients with Cardiovascular Disease.
S Virani,A Alonso,E Benjamin (2020). American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2020 update: a report from the American Heart Association.
Thomas Unger,Claudio Borghi,Fadi Charchar,Nadia Khan,Neil Poulter,Dorairaj Prabhakaran,Agustin Ramirez,Markus Schlaich,George Stergiou,Maciej Tomaszewski,Richard Wainford,Bryan Williams,Aletta Schutte (2020). 2020 International Society of Hypertension Global Hypertension Practice Guidelines.
Frank Chaloupka,Lisa Powell,Kenneth Warner (2019). The Use of Excise Taxes to Reduce Tobacco, Alcohol, and Sugary Beverage Consumption.
J Huang,K Walton,R Gerzoff,B King,F Chaloupka (2015). State Tobacco Control Program Spending -United States, 2011.
Kazim Husain,Rais Ansari,Leon Ferder (2014). Alcohol-induced hypertension: Mechanism and prevention.
M Canicoba,S Mauricio (2017). Valoración del estado nutricional en diversas situaciones clínicas.
Who (2022). Gráfico 1.3. La informalidad en los países de ALC es alta, 2017 o el último año disponible.
Shinta Nishioka,Hidetaka Wakabayashi (2022). Interaction between malnutrition and physical disability in older adults: is there a malnutrition-disability cycle?.
J Robertson,E Emerson,S Baines,C Hatton (2014). Obesity and health behaviours of British adults with self-reported intelectual impairments: cross sectional survey.
Carlos Ocres (2019). Vitamin d concentrations among older adults according to physical disability status: nhanes 2007-2014.
(2000). Global health estimates 2016: deaths by cause, age, sex, by country and by region.
(2017). Oficina de Promoción Social y la Sala situacional de las Personas con Discapacidad.
(2022). Behavioral Counseling Interventions to Promote a Healthy Diet and Physical Activity for Cardiovascular Disease Prevention in Adults Without Cardiovascular Disease Risk Factors: Updated Systematic Review for the U.S. Preventive Services Task Force.
L Alessandro (2019). Rehabilitación multidisciplinaria para pacientes adultos con accidente cerebrovascular.
Paula Quevedo (2019). La malnutrición: más allá de las deficiencias nutricionales.
Fernando Gómez,David Osorio-García,Luisa Panesso,Carmen-Lucia Curcio (2021). Healthy aging determinants and disability among older adults: SABE Colombia.
Fátima Núñez,Julieta Méndez,Miriam Espinola De Canata,Angel Rolón (2022). Fomento de la salud en pacientes con diabetes mellitus tipo 2 de las unidades de salud familiar del distrito de Limpio, Paraguay, 2022.
Cheryl Anderson,Anne Thorndike,Alice Lichtenstein,Linda Van Horn,Penny Kris-Etherton,Randi Foraker,Colleen Spees (2019). Innovation to Create a Healthy and Sustainable Food System: A Science Advisory From the American Heart Association.
(2018). Exercise Is Medicine: a global health initiative.
L J Frank,Visseren (2021). Corrigendum to: 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies With the special contribution of the European Association of Preventive Cardiology (EAPC).
Who (2021). CHAPTER 9. Joint FAO/WHO Nutrition Committee.
(2020). Foreword.
Yara Cárdenas-Cepero,Luisa (2022). La enseñanza de la biología desde la teoría general de sistemas: mirada bioética.
Mu Xia,Xueliu Li,Jonathan Tudge (2020). Operationalizing Urie Bronfenbrenner’s Process-Person-Context-Time Model.
H Bravo-Andrade,N Ruvalcaba,M Orozco,Y González-Gaxiola,M Hernández-Paz (2018). Introducción al modelo ecológico del desarrollo humano.
Tracey Gendron,Alexa Van Aartrjik,Kyrié Carpenter,Ryan Backer,Ashton Applewhite (2022). Ageism Interventions: The Need for An Ecological Perspective.
A Schenck,A Meyer,T Kuo,D Cilenti (2015). Building the evidence for decision-making: the relationship between local public health capacity and community mortality.
(2021). General mental health.
José Moreno-Montoya,Silvia Ballesteros,Heidy García-Orozco,Nubia Bautista-Bautista,Pedro Barrera-López,José De La Hoz-Valle (2016). Healthcare Seeking and Mortality of Patients with Diabetes during the COVID-19 Pandemic in Colombia: a Nationwide Study.
José Moreno-Montoya,Silvia Ballesteros,Heidy García-Orozco,Nubia Bautista-Bautista,Pedro Barrera-López,José De La Hoz-Valle (2025). Healthcare Seeking and Mortality of Patients with Diabetes during the COVID-19 Pandemic in Colombia: a Nationwide Study.
José Moreno-Montoya,Silvia Ballesteros,Heidy García-Orozco,Nubia Bautista-Bautista,Pedro Barrera-López,José De La Hoz-Valle (1581). Healthcare Seeking and Mortality of Patients with Diabetes during the COVID-19 Pandemic in Colombia: a Nationwide Study.
(1377). Ministerio de salud y Protección Social de Colombia.
Cruz-Jentoft A Bahat,G Bauer,J Boirie,Y Buryère,O Cederholm,T (2019). Sarcopenia: revised European consensus on definition and diagnosis.
Ordóñez Molina,J,Duque Ossman,J,Rosero Revelo,R,Palacio Uribe,J (2019). Recomendaciones de la Asociación Colombiana de Endocrinología, Diabetes y Metabolismo para el manejo de la obesidad.
K Casadei,J Kiel (2022). Anthropometric Measurement.
Petermann-R F Balntzi,V Gray,S Lara,J Ho,F Pell,J (2022). Global prevalence of sarcopenia and severe sarcopenia: a systematic review and metaanalysis.
Birgit Vahlberg,Lena Zetterberg,Birgitta Lindmark,Karin Hellström,Tommy Cederholm (2022). Functional performance, nutritional status, and body composition in ambulant community-dwelling individuals 1–3 years after suffering from a cerebral infarction or intracerebral bleeding.
Fiona Ecarnot,Domenico Rogoli,Stefania Maggi (2021). Epidemiology of Sarcopenia.
Tatsuro Inoue,Keisuke Maeda,Ayano Nagano,Akio Shimizu,Junko Ueshima,Kenta Murotani,Keisuke Sato,Kazuki Hotta,Shinichiro Morishita,Atsuhiro Tsubaki (2021). Related Factors and Clinical Outcomes of Osteosarcopenia: A Narrative Review.
E Dent,F Martin,H Bergman,J Woo,R Romero-Ortuno,J Walston (2019). Management of frailty: opportunities, challenges, and future directions.
V Strini,R Schiavolin,A Prendin (2021). Fall Risk Assessment Scales: A Systematic Literature Review.
W Willett,J Rockstrom (2019). Food in the Anthropocene: the EAT-Lancet Commission on healthy diets from sustainable food systems.
Yoshihide Sunada (2022). A Potential Nutritional Indicator Predictable for Stroke-Related Sarcopenia.
Nadja Scherbakov,Wolfram Doehner (2011). Sarcopenia in stroke—facts and numbers on muscle loss accounting for disability after stroke.
Robert Wood,Johnson Foundation (2018). The Robert Wood Johnson Foundation.
V Rodríguez,E Simon (2008). Bases de la Alimentación Humana.
Monica Serra (2018). The Importance of Assessing Nutritional Status to Ensure Optimal Recovery during the Chronic Phase of Stroke.
Ya Su,Michiko Yuki,Mika Otsuki (2020). Prevalence of stroke-related sarcopenia: A systematic review and meta-analysis.
Matthias Kaiser,Jürgen Bauer,Christiane Rämsch,Wolfgang Uter,Yves Guigoz,Tommy Cederholm,David Thomas,Patricia Anthony,Karen Charlton,Marcello Maggio,Alan Tsai,Bruno Vellas,Cornel Sieber (2010). Frequency of Malnutrition in Older Adults: A Multinational Perspective Using the Mini Nutritional Assessment.
Christopher Wallis,Bheeshma Ravi,Natalie Coburn,Robert Nam,Allan Detsky,Raj Satkunasivam (2017). Comparison of postoperative outcomes among patients treated by male and female surgeons: a population based matched cohort study.
Jorge Álvarez-Díaz (2020). La necesaria perspectiva de género para el análisis de problemas de salud.
Gao Qian Qian,K Hu,C Yan,B Zhao,F Mei,F Chen,L Zhao,Y Shang,Y Ma,B Ma (2021). Associated Factors of Sarcopenia in Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis.
C De Winter,L Bastiaanse,T Hilgenkamp,H Evenhuis,M Echteld (2012). Cardiovascular risk factors (diabetes, hypertension, hypercholesterolemia and metabolic syndrome) in older people with intellectual disability: Results of the HA-ID study.
Mar Bourel (2004). Contenu en sel de l'alimentation et hypertension arte´ rielle.
María Quiroga De Michelena,Isabel (2010). Hipertensión arterial - Aspectos genéticos.
Ramírez Bello,Julián,Oscar Pérez-Méndez,Ramírez-Fuentes,Silvestre,Carrillo-Sánchez,Silvia,Gilberto Vargas-Alarcón,José Fragoso,Manuel (2011). Genética y genómica de la hipertensión arterial: una actualización.
M Mudau,A Genis,A Lochner,H Strijdom (2012). Endothelial dysfunction: The early predictor of atherosclerosis.
Esc/Eas (2020). Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk.
Allan Hackshaw,Joan Morris,Sadie Boniface,Jin-Ling Tang,Dušan Milenković (2018). Low cigarette consumption and risk of coronary heart disease and stroke: meta-analysis of 141 cohort studies in 55 study reports.
Who (2018). WHO report on the global tobacco epidemic, 2025.
(2010). Reducing Tobacco Use: A Report of the Surgeon General: Executive Summary.
J Fernandez-Sola (2015). Cardiovascular risks and benefits of moderate and heavy alcohol consumption.
(2020). Correction to: Heart Disease and Stroke Statistics—2019 Update: A Report From the American Heart Association.
(2019). Unknown Title.
Juliana Carvalho,Marilia Correia,Hélcio Kanegusuku,Paulo Longano,Nelson Wolosker,Raphael Ritti-Dias,Gabriel Cucato (2022). Association between the risk of malnutrition and functional capacity in patients with peripheral arterial disease: A cross-sectional study.
(2020). Program Budget of the Pan American Health Organization 2020-2021.
Peter Lloyd-Sherlock,Shah Ebrahim,Ramon Martinez,Martin Mckee,Pedro Ordunez (2000). Reducing the cardiovascular disease burden for people of all ages in the Americas region: analysis of mortality data, 2000–15.
R Martínez-Leal,Salvador Carulla,L,Ruiz Gutiérrez-Colosía,M Nadal,M Novell-Alsina,R Martorell,A (2011). La salud en personas con discapacidad intelectual en España: estudio europeo POMONA-II.
M Hayes,Kelly Beiser,A Kase,C (2003). The influence of gender and age on disability following ischemic stroke: the Framingham study.
S Doyle,S Bennett,S Fasoli,K Mckenna (2010). Interventions for sensory impairment in the upper limb after stroke.
Juan Suárez Escudero,María Oviedo Cáceres,Yuliana Llano Naranjo,Johana Arias Uribe,José Villegas Mesa,María Zapata Vásquez,Jorge Ferreira Morales,Jessica Reyes Cisneros,Karen Cano Calle,Sydney Goldfeder De Gracia,Juan González Franco,Esau Astudillo Valverde (2011). Etiología de baja visión y ceguera en siete centros de referencia en Colombia entre los años 2012 a 2017.
Xiangfeng Cong,S Liu,W Wang,J Ma,J Li (2022). Combined consideration of body mass index and waist circumference identifies obesity patterns associated with risk of stroke in a Chinese prospective cohort study.
Michael Jensen,Donna Ryan,Caroline Apovian,Jamy Ard,Anthony Comuzzie,Karen Donato,Frank Hu,Van Hubbard,John Jakicic,Robert Kushner,Catherine Loria,Barbara Millen,Cathy Nonas,F Pi-Sunyer,June Stevens,Victor Stevens,Thomas Wadden,Bruce Wolfe,Susan Yanovski (2013). 2013 AHA/ACC/TOS Guideline for the Management of Overweight and Obesity in Adults.
E Mill-Ferreyra,V Cameno-Carrillo,H Saúl-Gordo,M Camí-Lavado (2018). Estimación del índice de masa corporal con base en la circunferencia braquial, para pacientes con discapacidad permanente o transitoria.
Xiangfeng Cong,S Liu,W Wang,J Ma,J Li (2022). Combined consideration of body mass index and waist circumference identifies obesity patterns associated with risk of stroke in a Chinese prospective cohort study.
Ahmed Negm,Jeremy Lee,Radmehr Hamidian,C Jones,Rachel Khadaroo (2022). Management of Sarcopenia: A Network Meta-Analysis of Randomized Controlled Trials.
R Izquierdo-Gómez,D Martínez-Gómez,A Acha,O Veiga,A Villagra,M Díaz-Cueto (2014). Objective assessment of sedentary time and physical activity throughout the week in adolescents with Down syndrome. The Up&Down study.
E Wilmot,C Edwardson,F Achana,M Davies,T Gorely,L Gray,K Khunti,T Yates,S Biddle (2012). Sedentary time in adults and the association with diabetes, cardiovascular disease and death: systematic review and meta-analysis.
J Manson,N Cook,I Lee (2019). Vitamin D supplements and prevention of cancer and cardiovascular disease.
F Lobelo,Rohm Young,D Sallis,R (2018). Council on Cardiovascular Surgery and Anesthesia; and Stroke Council. Routine assessment and promotion of physical activity in healthcare settings: a scientific statement from the American Heart Association.
Hernández Martínez,Blanca,Caballero Lambert,Ana Olivia,Estrada Salas,Ana Karen,Martha Guevara Sanginés,Leticia,Judith Orozco Méndez (2013). Nutrición y rendimiento en atletas con discapacidad intelectual y conocimientos de sus cuidadores.
Katie Brooker,Kate Van Dooren,Lyn Mcpherson,Nick Lennox,Robert Ware (2014). Systematic Review of Interventions Aiming to Improve Involvement in Physical Activity Among Adults With Intellectual Disability.
Pelliccia (2021). Comentarios a la guía ESC 2020 sobre cardiología del deporte y el ejercicio en pacientes con enfermedad cardiovascular.
E Preston,Ada Stanton,R (2016). Prediction of Independent Walking in People Who Are Nonambulatory Early After Stroke: A Systematic Review.
Carrie Patnode,Nadia Redmond,Megan Iacocca,Michelle Henninger (2022). Behavioral Counseling Interventions to Promote a Healthy Diet and Physical Activity for Cardiovascular Disease Prevention in Adults Without Known Cardiovascular Disease Risk Factors.
G Figueroa,L Muñoz,K Villamil,G Rosero,E Garicano Vilar,Hernández Villa,I,Onrubia González-De La Aleja,J Rodríguez -Alonso,P,San Mauro-Martín,I (2016). Estrategia educativa para modificar estilos de vida no saludables en adultos jóvenes con malnutrición.
Aritza Huarcaya Cordova (2018). Estilo de vida y estado nutricional del adulto mayor que acude al centro de salud Subtanjalla, Ica julio 2018.
Keita Tsutsumiuchi,Hidetaka Wakabayashi,Keisuke Maeda,Hiroshi Shamoto (2020). Impact of malnutrition on post-stroke cognitive impairment in convalescent rehabilitation ward inpatients.
J Wang,B Luo,Y Xie,H Hu,L Feng,Z Li (2014). Evaluation methods on the nutritional status of stroke patients.
H Wong,S Harith,P Lua,K Ibrahim (2020). Prevalence and predictors of malnutrition risk among poststroke patients in outpatient setting: a crosssectional study.
Amy Bodde,Dong-Chul Seo,Georgia Frey,Marieke Van Puymbroeck,David Lohrmann (2012). The Effect of a Designed Health Education Intervention on Physical Activity Knowledge and Participation of Adults with Intellectual Disabilities.
A Sayinzoga,C Lefèvre-Dognin,A Bourget Massari,J Paquereau,P Crenn (2018). État nutritionnel et profil métabolique du patient handicapé neuro-moteur adulte à l’admission et à la sortie de rééducation post-réanimation.
Randi Libbon,Jenna Triana,Alison Heru,Ellen Berman (2019). Family Skills for the Resident Toolbox: the 10-min Genogram, Ecomap, and Prescribing Homework.
Jhonatan De La Cruz Pérez (2018). Asociación entre el dolor, rigidez, capacidad funcional y la kinesiofobia en pacientes con gonartrosis del departamento de medicina de rehabilitación del Hospital Nacional Hipólito Unanue 2020.
C Caro,J Costa,Da Cruz,Dmc (2018). Burden and Quality of Life of Family Caregivers of Stroke Patients.
B Curryer,R Stancliffe,A Dew,M Wiese (2018). Choice and Control Within Family Relationships: The Lived Experience of Adults With Intellectual Disability.
Forguione-Pérez Vp (2015). Comunicación entre médico y paciente: más allá de una consulta, un proceso educativo.
Miguel Moscoso-Porras,German Alvarado (2018). Association between perceived discrimination and healthcare–seeking behavior in people with a disability.
Asena Caner (2016). Happiness and Life Satisfaction in Turkey in Recent Years.
Debra Brucker (2019). Supplemental nutrition assistance program participation among workingage adults with disabilities who experience employment exits and entries.
Sidney Kennedy (2016). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 3. Pharmacological treatments.
Yoonji Kim,Myung-Chul Kim,Hang-Sik Park,Il-Hoon Cho,Jean Paik (2018). Association of the Anxiety/Depression with Nutrition Intake in Stroke Patients.
Sonia Lupien,Robert-Paul Juster,Catherine Raymond,Marie-France Marin (2018). The effects of chronic stress on the human brain: From neurotoxicity, to vulnerability, to opportunity.
J Newson,D Hunter,T Thiagarajan (2020). The Heterogeneity of Mental Health Assessment.
Michael Gottschalk,Katharina Domschke (2022). Genetics of generalized anxiety disorder and related traits.
(2012). Actualización del marco conceptual y operacional para las redes integradas de servicios de salud en las Américas: Consenso técnico del Banco Interamericano de Desarrollo, el Banco Mundial y la Organización Panamericana de la Salud para fortalecer las redes integradas de servicios de salud en la Región de las Américas.
J Mikulovic,J Vanhelst,J Salleron,A Marcellini,R Compte,P Fardy (2014). Overweight in intellectually-disabled population: physical, behavioral and psychological characteristics.
Erik Blas,John Ataguba,Tanvir Huda,Giang Bao,Davide Rasella,Megan Gerecke (2016). The feasibility of measuring and monitoring social determinants of health and the relevance for policy and programme – a qualitative assessment of four countries.
Cutillas Orgilés (2017). Ernesto Distribución mundial de la población con discapacidades en relación con los patrones geográficos del desarrollo humano.
Gil Obando,Lida López López,Alexandra Aguas De La Ossa,María Margarita,Hernández Blanco (2017). Adultos en situación de discapacidad, Calidad de vida y características sociodemográficas en Sincelejo (Sucre, Colombia).
Shaun Grech,Kickbusch (2014). The spaces of poverty: Renegotiating place and disability in the global south.
I Kickbusch,L Allen,C Franz (2016). The commercial determinants of health.
Michael Palmer (2011). Disability and Poverty: A Conceptual Review.
S Mitra,M Palmer,H Kim,D Mont,N Groce (2017). Extra costs of living with a disability: A review and agenda for research.
Sophie Mitra,Aleksandra Posarac,Brandon Vick (2013). Disability and Poverty in Developing Countries: A Multidimensional Study.
Mónica Pinilla-Roncancio (2018). The reality of disability: Multidimensional poverty of people with disability and their families in Latin America.
Seung-Hye Choi,Smi Choi-Kwon,Min-Sun Kim,Jong-Sung Kim (2015). Poor nutrition and alcohol consumption are related to high serum homocysteine level at post-stroke.
Julie Paquereau,Etienne Allart,Monique Romon,Marc Rousseaux (2014). The Long-term Nutritional Status in Stroke Patients and its Predictive Factors.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Diana María Igua Ropero. 2026. \u201cNutritional Status in Adults with Disabilities Secondary to Cardiovascular Diseases in a Colombian Municipality A Cross- Sectional Study\u201d. Global Journal of Medical Research - F: Diseases GJMR-F Volume 23 (GJMR Volume 23 Issue F5): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.