## I. INTRODUCTION
Stillbirth is defined as a baby born with no signs of life at or after 28 weeks' gestation.[1, 2] It is one of the growing public health issues worldwide. In 2019, around 2 million babies were stillborn, with worldwide prevalence of 13.9 per 1000 total births.[2-4] Women in sub-Saharan Africa and Southern Asia bear the greatest burden of stillbirths in the world, where $42\%$ and $34\%$ of the global stillbirth occurred in sub-Saharan Africa and Southern Asia respectively. [2, 3] Where as women in Europe, Northern America, Australia and New Zealand bear lower burden of still birth in the world, with $2\%$ of global stillborn babies. [2] There is also large differences by national income group, $27\%$ of the global stillborn in low income groups compare to $2\%$ of the global stillborn in high income group. Overall, $40\%$ of stillbirth occurs during labor. [2, 3, 5] This loss could be avoided with improved monitoring and timely access to emergency obstetric care when required. [6]
This loss reaches far beyond the loss of life. Stillbirth has psychological impacts, such as maternal depression, and profound financial consequences for parents. And also it has long-term economic impacts for society. [7] But this traumatic loss of life remains a neglected issue. [2] They are invisible in policies and programs and underfinanced as an area requiring intervention. Targets specific to stillbirths were absent from the Millennium Development Goals (MDGs) and are still missing in the 2030 Agenda for Sustainable Development. [2]
The United Nations' Global Strategy for Women's, Children's and Adolescents' Health (2016-2030) includes stillbirths in its vision, "An end to preventable maternal, newborn, child and adolescent deaths and stillbirths", and urges for stillbirths to be prioritized. [2] The Every Newborn Action Plan (ENAP), which was endorsed by 194 WHO Member States, calls for each country to achieve a rate of 12 stillbirths or fewer per 1,000 total births by 2030 and to reduce equity gaps, particularly in countries that have already met the stillbirth target. [2, 8] In Eritrea, stillbirth rate was 18.3 stillbirth per 1000 total birth in 2019.[2] It was reduced by $21.3\%$ compared to stillbirth estimated in the year 2000. This rate makes Eritrea one of the 56 countries who are at risk of missing the ENAP stillbirth target by 2030. [2]
Risk factors for stillbirth can be due to Socioeconomic and demographic, obstetric and fetal factors. Socioeconomic and demographic factors which is primarily a combination of education, residency, marital status, occupation, income and age had an influence on the still birth rate as showed in different studies. [1, 2, 9-13] A study in rural China showed that paternal exposure to smoking was risk factors of stillbirth. the study also showed that Folic acid intake before and after pregnancy had a protect factors of stillbirth. [14]
Different study showed that preceding birth interval less than 24 month, increasing parity, maternal hypertension or pregnancy induced hypertension, maternal diabetes, maternal obesity, previous history of stillbirth, bleeding during pregnancy, febrile illness during pregnancy, mother with no or inadequate prenatal care, labour length greater or equal to 24 hours, refereed cases, presence meconium and not using partograph were obstetric risk factors associated with stillbirth. [1, 2, 9-20] A study in Nigeria showed that delivery at health facilities was more risky by $81\%$.[21] the same study also showed that C-section was $46\%$ more risky than vaginal delivery. Study done by Tesema et al. revealed also C-section was by $81\%$ more risky than counterparts. [11] Different studies showed that fetal factors associated with stillbirths were being male by gender, fetal congenital malformation, and low birth weight or small for gestational age and multiple pregnancies. [2, 9, 12, 17, 19, 20, 22]
Establishing association of stillbirth with different maternal, fetal, pregnancy and obstetric factors can help to prioritize interventions to improve birth outcomes in resource-poor areas, including Eritrea.[23] To the knowledge of the researchers, a similar research has not been done in Eritrea. Research is critical to develop interventions aimed at averting such risk factors of stillbirth. Hence, this study was conducted to identify socio-demographic, maternal health-related and obstetric-related factors that possibly result in stillbirth in the study area.
## II. METHODOLOGY
### a) Study Design
The study was a hospital-based unmatched case-control. Mothers who gave stillbirths were considered as cases whereas those who gave live births were considered as controls. The inclusion criteria were whose with charts available and had all the necessary information.
### b) Study area
The study was conducted at Dekemhare Hospital, which is located in Zoba Debub (Southern Region), around 40 km to south east of Asmara, the capital city of Eritrea. This hospital provides service to subzone of Dekemhare, which has a population around 60,000. [24] It also serves as a referral center for three subzones of Southern Region; Segheneyti, Mai-ayni and Tsurona. This hospital comprises several wards such as medical, pediatric, maternity and also dental and ophthalmic clinics. Maternity hospital provides comprehensive emergency, obstetric, and neonatal care service. In addition, the hospital provides maternal waiting room.
### c) Study population
All mothers who delivered from January 2017 to December 2021 in Dekemhare Hospital were the study population.
### d) Sample Size Determination
Sample size was calculated using Epi-Info 7.0 StatCalc program by taking assumptions of $95\%$ confidence level, three controls for each case, $80\%$ power and $35\%$ prevalence of exposure (birth weight was taken as exposure) among control and odds ratio 1.78. A total sample size of 543 (136 cases and 407 controls) were calculated.
### e) Sampling procedure
Consecutive sampling was implemented to recruit all cases in the study area—all stillbirths with complete information were selected. However, to select controls, first, all live births in the hospital with complete information were listed to create a sampling frame, and then simple random sampling technique was applied to enroll those live births.
### f) Study Variable
The dependent variable for present study was birth outcome dichotomized in to stillbirth and live birth. And the independent variables were sociodemographic factors (age, residence, occupation, marital status), past and present obstetric history and medical history related factor(gravidity, parity, preceding birth interval, history of stillbirth, hypertensive disorder of pregnancy, premature rupture of membrane), abortion and delivery related factors (mode of admission, partograph use, fetal presentation, cord accident, obstructed labor, labor augmentation, duration of labor, mode of delivery) and fetal related factors (gestational age at birth, birth weight, number of newborns, congenital structure).
## III. DATA COLLECTION
Data were collected using structured data extraction tool developed from literature related to stillbirth and modified according to the local context by the investigators. The tool consists of several sections regarding to sociodemographic, maternal health and pregnancy, labor and delivery and birth outcome.
Data collectors identified charts of mothers from card room using medical record numbers and reviewed the history, delivery summary, partograph, decision notes, progress notes, and operation notes and filled in the checklist. Incomplete charts on major variables under study (no information about birth outcome and missing data more than $40\%$ the variable) were excluded.
### a) Data Quality Control and Assurance
Prior to data collection, the data collectors were trained with a practical session for one day on techniques of data collection. Pretest was carried out on $5\%$ of the samples in the same hospital in the years before the study period and modification of the checklist was made on rephrasing and skipping patterns. The investigator reviewed all checklists for omissions, clarity, and consistency of data to verify the completeness of the collected data.
### b) Data Analysis
Data were entered in CSPro 7.2 and were analyzed using SPSS version 26 b. Frequency, percentage and odds ratio (crude and adjusted) were used to describe the study population in relation to relevant variables. Univariable and multivariable logistic regression was used to identify characteristics associated with outcome. Variables found to have statistically significant associations with the outcome of interest at univariable analysis were considered in the multivariable analysis. Crude and adjusted odds ratio with $95\%$ CI was calculated and p-value $<0.02$ and
$< 0.05$, respectively, was used to declare statistical significance.
### c) Ethical considerations
Ethical clearance was obtained from the Research Ethics and Review Committee of Ministry of Health, and further permission was obtained from offices of the Ministry of Health Debub Zone and Dekemhare Hospital. Patient's confidentiality was kept secured and only selected researchers had an access to the data and personal identifiers were codded and removed from analysis. Consent form was not sought from enrolled individuals as this study was using a secondary data.
## IV. RESULTS
During the study period there were 6079 total deliveries and 151 stillbirths. Thus, the prevalence of stillbirth during the study period in Dekemhare Hospital was $2.5\%$ or 25 per 1000 deliveries. Out of 151 stillbirths, 13 cases were excluded from the study due to incomplete information. So finally a total of 552 sample charts of mothers who gave birth in Dekemhare Hospital were included in the analysis. Of all stillbirth, $51\%$ were fresh (fetal death during labor and delivery) and $49\%$ were macerated. (Fig 2) The maternal mean age was 28 years $(SD = 6.3)$ and $62\%$ of cases and $78\%$ of controls were aged between 20 to 34 years. Vast majority of cases $(89\%)$ and controls $(96\%)$ were married. $59\%$ of cases and $34\%$ of controls were rural resident. Besides, $91\%$ cases and $95\%$ controls were housewives. (Table 1)
Table 1: Sociodemographic Characteristics of Mothers in Dekemhare Hospital, Jan 2017 to Dec 2021(N=552)
<table><tr><td>Variables</td><td>Category</td><td>Cases N (%)</td><td>Controls N (%)</td><td>Total N (%)</td></tr><tr><td rowspan="3">Maternal age</td><td>less than 20</td><td>11 (8)</td><td>21 (5)</td><td>32 (5.8)</td></tr><tr><td>20 to 34</td><td>85 (62)</td><td>321(78)</td><td>406 (74)</td></tr><tr><td>above 34</td><td>42 (30)</td><td>72 (17)</td><td>114 (21)</td></tr><tr><td rowspan="2">Residency</td><td>urban</td><td>56 (41)</td><td>272(66)</td><td>328 (59)</td></tr><tr><td>rural</td><td>82 (59)</td><td>142 (34)</td><td>224 (40)</td></tr><tr><td rowspan="2">Marital status</td><td>married</td><td>123 (89)</td><td>398(96)</td><td>521(94)</td></tr><tr><td>single</td><td>15 (11)</td><td>16 (4)</td><td>31 (7)</td></tr><tr><td rowspan="2">Occupation</td><td>house wife</td><td>125 (91)</td><td>393 (95)</td><td>518 (94)</td></tr><tr><td>employed</td><td>13 (9)</td><td>21 (5%)</td><td>34 (6)</td></tr></table>
### a) Maternal Health and Pregnancy Related Characteristics of Participants
More than three-fourths, $78\%$ of cases and $76\%$ of controls were multigravida and $11\%$ of cases and $8\%$ of controls had previous history of stillbirth. Merely, $4\%$ of cases and $1\%$ of controls had experienced different medical illness. Regarding birth interval, $17\%$ of cases and $12\%$ of controls had presiding birth interval of less than 2 years. (Table 2)
<table><tr><td colspan="5">Table 2: Maternal Health Related Characteristics of Mothers in Dekemhare Hospital, Jan 2017 to Dec 2021(N=552)</td></tr><tr><td>Variables</td><td>Category</td><td>Cases N (%)</td><td>Controls N (%)</td><td>Total N (%)</td></tr><tr><td rowspan="2">Gravidity</td><td>Primigravida</td><td>31 (23)</td><td>99 (24)</td><td>130 (24)</td></tr><tr><td>Multigravida</td><td>107 (78)</td><td>315 (76)</td><td>422 (76)</td></tr><tr><td rowspan="2">Parity</td><td>Primiparos</td><td>36 (26)</td><td>106 (26)</td><td>142 (26)</td></tr><tr><td>Multipara</td><td>102 (74)</td><td>308 (74)</td><td>410 (74)</td></tr><tr><td rowspan="2">History of abortion</td><td>Yes</td><td>30 (22)</td><td>83 (20)</td><td>113 (21)</td></tr><tr><td>No</td><td>78 (57)</td><td>236 (57)</td><td>314 (57)</td></tr><tr><td rowspan="2">Preceding birth interval</td><td>< 2 years</td><td>18 (17)</td><td>47 (12)</td><td>65 (12)</td></tr><tr><td>≥ 2 years</td><td>89 (83)</td><td>268 (65)</td><td>357 (65)</td></tr><tr><td rowspan="2">History of still birth</td><td>Yes</td><td>15 (11)</td><td>32 (8)</td><td>47 (9)</td></tr><tr><td>No</td><td>92 (67)</td><td>288 (70)</td><td>380(69)</td></tr><tr><td rowspan="2">Maternal medical illness</td><td>Yes</td><td>5 (4)</td><td>6 (1)</td><td>11 (2)</td></tr><tr><td>No</td><td>133 (96)</td><td>408 (99)</td><td>541 (98)</td></tr></table>
### b) Labor and Delivery Related Characteristics of Participants
Almost two third, $65\%$ of cases and $76\%$ of controls, were admitted in the first stage of labour. About $38\%$ of cases and $11\%$ of controls were referred from other health facilities. And around $19\%$ of cases and $37\%$ of controls filled in the three components of partograph (fetal condition, progress of labour and maternal condition). Augmentation or induction of labour was conducted in $9\%$ of cases and in $3\%$ of controls. In the cases group $5\%$ had cord accident and $3\%$ had uterine rupture, but none of those were happened among control. Prolonged obstructed labour was experienced in $15\%$ of cases and $5\%$ of controls. (Table 3)
<table><tr><td colspan="5">Table 3: Labor and Delivery Related Characteristics of Mothers in Dekemhare Hospital, Jan 2017 to Dec 2021(N=552)</td></tr><tr><td>Variable</td><td>Category</td><td>Cases N (%)</td><td>Controls N (%)</td><td>Total N (%)</td></tr><tr><td rowspan="2">Use of partograph</td><td>Yes</td><td>26 (19)</td><td>154 (37)</td><td>180 (33)</td></tr><tr><td>No</td><td>112 (81)</td><td>260 (63)</td><td>372 (67)</td></tr><tr><td rowspan="2">Prolonged obstructed</td><td>Yes</td><td>20 (15)</td><td>21 (5)</td><td>41 (7)</td></tr><tr><td>No</td><td>118 (86)</td><td>393 (95)</td><td>511 (93)</td></tr><tr><td rowspan="2">Augment or induced</td><td>Yes</td><td>12 (9)</td><td>11 (3)</td><td>23 (4)</td></tr><tr><td>No</td><td>126 (91)</td><td>403 (97)</td><td>529 (96)</td></tr><tr><td rowspan="2">Prom</td><td>Yes</td><td>3 (2)</td><td>25 (6)</td><td>28 (5)</td></tr><tr><td>No</td><td>135 (98)</td><td>389 (94)</td><td>524 (95)</td></tr><tr><td rowspan="2">Duration of labour</td><td>Less than 24h</td><td>127 (92)</td><td>385 (93)</td><td>512 (92)</td></tr><tr><td>> or equal 24h</td><td>11 (8)</td><td>31 (7)</td><td>42 (8)</td></tr><tr><td rowspan="2">Mode of admission</td><td>Referred</td><td>52 (38)</td><td>46 (11)</td><td>98 (18)</td></tr><tr><td>Not referred</td><td>86 (62)</td><td>368 (89)</td><td>454 (82)</td></tr><tr><td rowspan="2">Presence of PIH</td><td>Yes</td><td>4 (3)</td><td>1 (0)</td><td>5 (1)</td></tr><tr><td>No</td><td>134 (97)</td><td>413 (100)</td><td>547(99)</td></tr><tr><td rowspan="2">Presence of cord accident</td><td>Yes</td><td>7 (5)</td><td>1 (0)</td><td>8 (1)</td></tr><tr><td>No</td><td>131 (95)</td><td>413 (100)</td><td>544 (99)</td></tr><tr><td rowspan="2">Presence of uterine rupture</td><td>Yes</td><td>4 (3)</td><td>0 (0)</td><td>4 (1)</td></tr><tr><td>No</td><td>134 (97)</td><td>414 (100)</td><td>548 (99)</td></tr><tr><td>Presence of APH</td><td>Yes</td><td>4 (3)</td><td>2 (1)</td><td>6 (1)</td></tr><tr><td></td><td>No</td><td>134 (97)</td><td>412 (99)</td><td>546(99)</td></tr><tr><td rowspan="2">Stage of labour on admission</td><td>First stage</td><td>89 (65)</td><td>315 (76)</td><td>404 (73)</td></tr><tr><td>Second stage</td><td>49 (35)</td><td>99 (24)</td><td>148 (27)</td></tr><tr><td rowspan="3">Mode of delivery</td><td>cephalic</td><td>94 (68)</td><td>374 (90)</td><td>468 (85)</td></tr><tr><td>Breech delivery</td><td>25 (18)</td><td>9 (2)</td><td>34 (6)</td></tr><tr><td>Cs delivery</td><td>19 (14)</td><td>31 (8)</td><td>50 (9)</td></tr></table>
### c) Fetal Related Characteristics of participants
From a total of 138 cases reviewed, $32\%$ had positive fetal heart beat on admission. And also $72\%$ of cases and $89\%$ of controls delivered in their gestational age between 37 and 42 weeks. Around $49\%$ of cases' babies and $91\%$ of controls' babies had birth weight in the range of 2500- 3999 g. Of all deliveries, $59\%$ of case and $51\%$ of controls delivered male newborns and also only $6\%$ of cases and $7\%$ controls had multiple deliveries. Among deliveries $15\%$ of cases and $1\%$ of controls had fetal congenital malformation. Among all the fetal congenital malformation, $64\%$ were neural tube defects. (Fig 1) The mean birth weight was 2603 $(\mathrm{SD} = 941)$ gram for case and 3236 $(\mathrm{SD} = 459)$ gram for controls. And also mean gestational age was $37(\mathrm{SD} = 3)$ weeks of the cases and $39(\mathrm{SD} = 1)$ weeks for controls.(Table 4)
<table><tr><td colspan="5">Table 4: Fetal Related Characteristics in Dekemhare Hospital, Jan 2017 to Dec 2021(N=552)</td></tr><tr><td>Variables</td><td>Category N (%)</td><td>Cases N (%)</td><td>Controls N (%)</td><td>Total N (%)</td></tr><tr><td rowspan="2">Number of fetus</td><td>Single</td><td>130 (94)</td><td>407 (98)</td><td>537 (97)</td></tr><tr><td>Twin</td><td>8 (6)</td><td>7 (2)</td><td>15 (3)</td></tr><tr><td rowspan="2">Baby gender</td><td>Female</td><td>56 (41)</td><td>204 (50)</td><td>260 (47)</td></tr><tr><td>Male</td><td>82 (59)</td><td>210 (51)</td><td>292 (53)</td></tr><tr><td rowspan="3">Birth weight</td><td>Less 2500</td><td>59 (43)</td><td>16 (4)</td><td>75 (14)</td></tr><tr><td>2500-3999</td><td>67 (49)</td><td>375 (91)</td><td>442 (80)</td></tr><tr><td>Above 4000</td><td>12 (9)</td><td>23 (6)</td><td>35 (6)</td></tr><tr><td rowspan="2">Type of stillbirth</td><td>Fresh stillbirth</td><td>70 5(1)</td><td>0 (0)</td><td>70 (13)</td></tr><tr><td>Macerated stillbirth</td><td>68 (49)</td><td>0 (0)</td><td>68 (12)</td></tr><tr><td rowspan="2">Congenital abnormality</td><td>Yes</td><td>21 (15)</td><td>4 (1)</td><td>25 (5)</td></tr><tr><td>No</td><td>117 (85)</td><td>410 (99)</td><td>527 (96)</td></tr><tr><td rowspan="3">Gestational age</td><td>< 37</td><td>35 (25)</td><td>31 (8)</td><td>66 (12)</td></tr><tr><td>37-42</td><td>99 (72)</td><td>367 (89)</td><td>466 (85)</td></tr><tr><td>>=42</td><td>4 (3)</td><td>16 (4)</td><td>20 (4)</td></tr><tr><td rowspan="2">Mean with SD</td><td>Birth weight (gram)</td><td>2603+941</td><td>3236+459</td><td>3078+673</td></tr><tr><td>Gestational age (weeks)</td><td>37+3</td><td>39+1</td><td>38+2</td></tr></table>
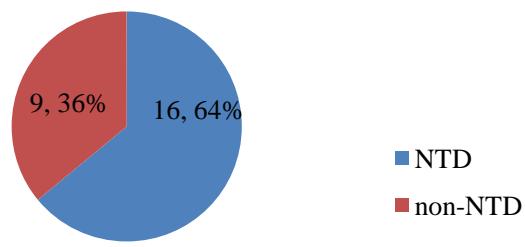 Fig 1: Types of congenital malformation in Dekemhare Hospital, Jan 2017 to Dec 2021 (N=25)
NTD= Neural Tube Defect
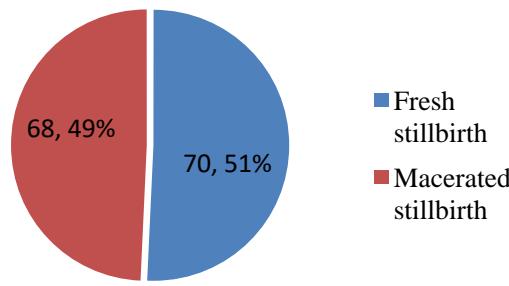 Fig 2: Type of stillbirth in Dekemhare Hospital, Jan 2017 to Dec 2021(N=138)
### d) Determinants of Stillbirth
A univariable analysis was done to assess the association of stillbirth with different independent variables using logistic regression. The result showed that variables like residency, mode of delivery, number of fetus, birth weight, marital status, use of partograph, gestational age, presence of congenital abnormality, presence of prolonged obstructed labour, labour augmentation or induction, mode of admission, presence of PIH and presence of APH have shown statistical association with stillbirth in the univariable analysis (Table 5).
Those variables with a $p < 0.2$ in the univariable analysis were considered for model building. A forward selection was used to eliminate insignificant covariates from the final model. Besides, multicollinearity was checked to assess whether covariates had correlation. The results from the final model revealed that, breech (AOR: 10.27; $95\% \mathrm{CI}$: 3.87-27.27), congenital abnormalities (AOR: 9.36; $95\% \mathrm{CI}$: 2.47-35.45), referred from other health facilities (AOR: 4.71; $95\% \mathrm{CI}$: 2.41-9.17), augmented or induced (AOR: 4.79; $95\% \mathrm{CI}$: 1.33-17.31), cord accident (AOR: 75.40; $95\% \mathrm{CI}$: 6.57-865.75) were found be risk factors of stillbirth. Conversely, birth weight 2500-3999 g (AOR: 0.03; $95\% \mathrm{CI}$: 0.01-0.07), above 4000g (AOR: 0.12; $95\% \mathrm{CI}$: 0.04-0.32), utilized partograph (AOR: 0.38; $95\% \mathrm{CI}$: 0.20-0.74), PIH (AOR: 0.03; $95\% \mathrm{CI}$: 0.03-0.36), PROM (AOR: 0.14; $95\% \mathrm{CI}$: 0.03-0.68) were found to be a protective factor of stillbirth. (Table 5)
<table><tr><td colspan="4">Table 5: Determinants of Stillbirth among Women Attended Deliveries in Dekemhare Hospital, a univariable and multivariable analysis</td></tr><tr><td>Variables</td><td>Categories</td><td>COR (95%CI)</td><td>AOR (95%CI)</td></tr><tr><td rowspan="2">Residence</td><td>Rural</td><td>1</td><td></td></tr><tr><td>Urban</td><td>0.35 (0.24-0.53)*</td><td></td></tr><tr><td rowspan="3">Mode of delivery</td><td>Cephalic</td><td>1</td><td>1</td></tr><tr><td>Breech</td><td>11.11 (5.02-24.60)*</td><td>10.27 (3.87-27.27)**</td></tr><tr><td>CS</td><td>2.45 (1.33-4.53)*</td><td>1.74 (0.75-4.05)</td></tr><tr><td rowspan="2">Number of fetus</td><td>Multiple</td><td>1</td><td></td></tr><tr><td>Single</td><td>0.28 (0.10-0.78)*</td><td></td></tr><tr><td rowspan="3">Birth weight</td><td><2500</td><td>1</td><td>1</td></tr><tr><td>2500-3999</td><td>0.05 (0.03-0.09)*</td><td>0.03 (0.01-0.07)**</td></tr><tr><td>4000+</td><td>0.14 (0.06-0.35)*</td><td>0.12 (0.04-0.32)**</td></tr><tr><td rowspan="2">Marital status</td><td>Married</td><td>1</td><td></td></tr><tr><td>Single</td><td>0.33 (0.15-068)*</td><td></td></tr><tr><td rowspan="2">Use of partograph</td><td>No</td><td>1</td><td>1</td></tr><tr><td>Yes</td><td>0.39 (0.25-0.63)*</td><td>0.38 (0.20-0.74)**</td></tr><tr><td rowspan="3">Gestational age</td><td><37</td><td>1</td><td></td></tr><tr><td>37-42</td><td>0.24 (0.14-0.40)*</td><td></td></tr><tr><td>>=42</td><td>0.22 (0.07-0.73)*</td><td></td></tr><tr><td rowspan="2">Congenital abnormality</td><td>No</td><td>1</td><td>1</td></tr><tr><td>Yes</td><td>18.49 (6.22-54.92)*</td><td>9.36(2.47-35.45)**</td></tr><tr><td rowspan="2">Prolonged obstructed</td><td>No</td><td>1</td><td></td></tr><tr><td>Yes</td><td>3.19 (1.67-6.08)*</td><td></td></tr><tr><td rowspan="2">Augmentation or induced labour</td><td>No</td><td>1</td><td>1</td></tr><tr><td>Yes</td><td>3.51 (1.51-8.14)*</td><td>4.79 (1.33-17.31)**</td></tr><tr><td rowspan="2">Mode of admission</td><td>not referred</td><td>1</td><td>1</td></tr><tr><td>referred</td><td>4.86 (3.07-7.71)*</td><td>4.71 (2.41-9.17)**</td></tr><tr><td rowspan="2">Presence of PIH</td><td>No</td><td>1</td><td>1</td></tr><tr><td>Yes</td><td>12.39 (1.37-111.80)*</td><td>0.03 (0.03-0.36)**</td></tr><tr><td rowspan="2">Presence of cord accident</td><td>No</td><td>1</td><td>1</td></tr><tr><td>Yes</td><td>22.18 (2.70-181.90)*</td><td>75.40 (6.57-865.75)**</td></tr><tr><td rowspan="2">PROM</td><td>No</td><td>1</td><td>1</td></tr><tr><td>Yes</td><td>0.35 (0.10-1.17) *</td><td>0.14 (0.03-0.68)**</td></tr></table>
## V. DISCUSSION
According to the findings of this study prevalence of stillbirth was $2.5\%$. The prevalence of stillbirth was almost consistent with a study conducted in South India and Bangladesh, which shows $2.97\%$ and $2.6\%$ respectively.[20, 25] Nonetheless, it was higher than studies done in India, Saudi Arabia, and Nepal.[10, 12, 26-28] Beside, it was lower than studies in Nigeria $(12.4\%)$, Aksum $(3.68\%)$, Nigerian referral hospital $(3.96\%)$ and tertiary hospital Nigerdelta $(4.8\%)$.[1, 21, 29, 30] In this study breech delivery was significantly associated with stillbirth compared to cephalic delivery. This result was in agreement with findings in various studies. [26, 30-32] so, breech presentation needs Closer surveillance and appropriate management to prevent stillbirth.
The odds of having stillbirth were higher in those delivered with fetal congenital abnormalities than without congenital abnormality in this study. This finding was consistent with studies done in other settings. [20, 27, 28, 33]. This could be explained by a lack of maturity of the vital organs for fetal survival making the fetus disposed to fatal complications and death. There is belief that continuing stillbirths are inevitable, and mostly due to non-preventable congenital abnormalities, but not all congenital abnormalities are inevitable, like neural tube defect could be prevented through folic acid supplementation.
This study found that women who referred from other facilities had more risk to have stillbirth than counterparts. This finding was in agreement with similar study findings at Nigeria, Southeast Ethiopia, and India. [17, 26, 29] This can be explained by most of the referred mothers coming from peripheral health facilities with serious complications. And also the distance to reach the hospitals to which they were referred pays to delay in receiving care, which can obviously cost the life of their fetus.
The odds of experiencing stillbirth were higher among mothers who had labour augmented or induced than their counterparts. This finding is consistent with the findings of studies in Ethiopia and India, [22, 34] But a study in Nepal revealed that Women with augmentation of labor had no increased risk of stillbirth. [35] In the present study stillbirth was higher among mothers with umbilical cord accident than those without umbilical cord accident. This is in line with a study by Collins. [36] This could be due to compromised blood
circulation to the fetus, which leads to hypoxia and death. This indicates that, now it is time to focus on screening and managing umbilical cord accident prenatally.
According to the finding of this study, giving birth to a baby weighing above 2500gm was found to be a protective a factor associated with stillbirth. This finding is in line with studies done in Ghana, Ethiopia, Nepal, Nigeria, Southwestern Ethiopia and Southeast Ethiopia. [12, 17-19, 30, 34, 37] This could be due to the fact that low birth weight is a complicated public health problem that includes long-term maternal malnutrition, ill health, and poor health care during pregnancy; which all can result in immature newborn and stillbirth.
This study yielded that those mothers whose labour was followed by partograph had reduced stillbirth than those not followed by partograph. This result was consistent with studies in Ethiopia, Aksum General Hospital and Nepal, that showed increased risk of stillbirth if the partograph was not used.[1, 10, 34] Poor partograph utilization may resulted in prolonging second stage of labor which could also result in miserable interventions like cesarean section, augmentation and instrumental delivery.[1] In this study pregnancy induced hypertension showed protective effect. The current study's finding was consistent with study done in Japan, which showed PIH has a protective to stillbirth.[38] However, this finding was inconsistent to studies in several settings. [9, 13, 14, 37, 39-43] This is probably because infants are delivered early due to maternal reasons, which reduces the stillbirth risk before the disease becomes symptomatic. [38] The presence of PROM was found to be a protective factor for stillbirth. This finding was in contrast to study done in Ethiopia, which showed PROM was a risk factor for stillbirth. [34] Nonetheless, another study showed a non-significant effect of early rupture of membrane on stillbirth. [44]
## VI. LIMITATION OF THE STUDY
The study was institution based study that can't be generalized to other settings. The study did not assess the effect of ANC attending and number of visits due to its absence in the documentation that could have an effect on results. Since this study was solely retrospective, it was opened to bias and results may be affected. Finally, this study did not explore the quality of care given in the health facility that requires advanced investigation which may have contribution to additional risk factors for stillbirth. So, further prospective study is needed to address these issues.
## VII. CONCLUSION
The factors that negatively affected stillbirth were not use of partograph, low birth weight, being referred from other health facility, labour augmentation or induction, presence of fetal congenital malformation, and presence of cord accident. Conversely, presence of PIH and PROM had a protective effect of stillbirth.
Based on this study, we highly recommended on the improvement of health care provider's skill to manage babies presenting in breech position, utilization of partograph during labour, strengthening referral system and monitoring and evaluating of referral practice, improving documentation of antenatal care visits in delivery register. And also timely and early identification of mothers who are at risk for neural tube defect and supplementation of folic acid at preconception.
Author Contributions: HG, FK and BT contributed to the study conception and design. Material preparation, data collection and analysis were performed by all authors. All the authors reviewed the manuscript and approved the final version of the manuscript.
Funding: This research had no any source of fund.
Disclosure
Abbreviations: PROM: Premature Rupture of Membrane; PIH: Pregnancy Induced Hypertension; CS: Cesarean Section; APH: Antepartum Haemorrhage
### ACKNOWLEDGMENTS
Authors acknowledges to the data collectors and Dekemhare hospital.
Conflict of interest: The authors report no conflicts of interest in this work.
Generating HTML Viewer...
References
44 Cites in Article
Tesfay Berhe,Hailay Gebreyesus,Haftom Teklay (2019). Prevalence and determinants of stillbirth among women attended deliveries in Aksum General Hospital: a facility based cross-sectional study.
(2020). United Nations Inter-agency Group for Child Mortality Estimation (UN IGME): A Neglected Tragedy: The global burden of stillbirths.
Lucia Hug,Danzhen You,Hannah Blencowe,Anu Mishra,Zhengfan Wang,Miranda Fix,Jon Wakefield,Allisyn Moran,Victor Gaigbe-Togbe,Emi Suzuki,Dianna Blau,Simon Cousens,Andreea Creanga,Trevor Croft,Kenneth Hill,K Joseph,Salome Maswime,Elizabeth Mcclure,Robert Pattinson,Jon Pedersen,Lucy Smith,Jennifer Zeitlin,Leontine Alkema (2021). Global, regional, and national estimates and trends in stillbirths from 2000 to 2019: a systematic assessment.
Sethi (2019). Assessment of knowledge of evidencebased maternal and newborn care practices among midwives and nurses in six provinces in Indonesia.
Unicef Who (2020). ENDING PREVENTABLE NEWBORN DEATHS AND STILLBIRTHS BY 2030: MOVING FASTER TOWARDS HIGH-QUALITY UNIVERSAL.
Gary Darmstadt,Mohammad Yakoob,Rachel Haws,Esme Menezes,Tanya Soomro,Zulfiqar Bhutta (2009). Reducing stillbirths: interventions during labour.
(2021). Joint Technical Brief on Stillbirth Situation and Way Forward for the East Mediterranean, Arab States, and Middle East & North Africa Region. Amman/Cairo: World Health Organization Regional Office for the Eastern Mediterranean (WHO EMRO), United Nations Population Fund Arab States Regional Office (UNFPA ASRO), United Nations Children's Fund Regional Office for the Middle East & North Africa.
Lynn Callister (2016). Global Strategy for the Health of Women, Children, and Adolescents.
Marcia Almeida,Gizelton Alencar,Hillegonda Novaes,Ivan França Jr,Arnaldo Siqueira,Oona Campbell,Daniela Schoeps,Laura Rodrigues (2007). Risk-factors for antepartum fetal deaths in the city of São Paulo, Brazil.
Ashish Kc,Johan Wrammert,Robert Clark,Uwe Ewald,Mats Målqvist (2016). Inadequate fetal heart rate monitoring and poor use of partogram associated with intrapartum stillbirth: a case-referent study in Nepal.
Tesema (2021). Prevalence of stillbirth and its associated factors in East Africa: generalized linear mixed modeling.
J Hirst,J Villar,C Victora,A Papageorghiou,D Finkton,F Barros,M Gravett,F Giuliani,M Purwar,I Frederick,R Pang,L Cheikh Ismail,A Lambert,W Stones,Y Jaffer,D Altman,J Noble,E Ohuma,S Kennedy,Z Bhutta (2018). The antepartum stillbirth syndrome: risk factors and pregnancy conditions identified from the <scp>INTERGROWTH</scp>‐21<sup>st</sup> Project.
Sujatha Lakshmi,Uma Thankam,Preetha Jagadhamma,Anuja Ushakumari,Nirmala Chellamma,Sankar Hariharan (2017). Risk factors for still birth: a hospital based case control study.
Yimin Qu,Shi Chen,Hui Pan,Huijuan Zhu,Chengsheng Yan,Shikun Zhang,Yu Jiang (2019). Risk factors of stillbirth in rural China: A national cohort study.
M Robert,Silver (2011). Causes of Death Among Stillbirths.
(2016). WHO: Making every baby count: audit and review of stillbirths and neonatal deaths.
Mekonnen Dagne (2021). Determinants of Stillbirth among Deliveries Attended in Bale Zone Hospitals, Oromia Regional State, Southeast Ethiopia: A Case-Control Study.
Engelbert Nonterah,Isaiah Agorinya,Edmund Kanmiki,Juliana Kagura,Mariatu Tamimu,Emmanuel Ayamba,Esmond Nonterah,Michael Kaburise,Majeedallahi Al-Hassan,Winfred Ofosu,Abraham Oduro,John Awonoor-Williams (2020). Trends and risk factors associated with stillbirths: A case study of the Navrongo War Memorial Hospital in Northern Ghana.
Tensay Welegebriel,Tegene Dadi,Kebadnew Mihrete (2017). Determinants of stillbirth in Bonga General and Mizan Tepi University Teaching Hospitals southwestern Ethiopia, 2016: a case–control study.
V Rajshekher,Mali (2021). Association of Stillbirths with Maternal and Fetal Risk Factors in a Tertiary Care Hospital in South India.
C Njoku,C Emechebe,E Eyong,J Ukaga,K Anachuna (2016). Prevalence and risk factors for stillbirths in a tertiary hospital in Niger Delta area of Nigeria: a ten year review.
Newtonraj (2017). Level, causes, and risk factors of stillbirth: a population-based case control study from Chandigarh, India.
Vicki Flenady,J Frøen,Halit Pinar,Rozbeh Torabi,Eli Saastad,Grace Guyon,Laurie Russell,Adrian Charles,Catherine Harrison,Lawrence Chauke,Robert Pattinson,Rachel Koshy,Safiah Bahrin,Glenn Gardener,Katie Day,Karin Petersson,Adrienne Gordon,Kristen Gilshenan (2009). An evaluation of classification systems for stillbirth.
Shamsun Nahar,Atiya Rahman,Hashima Nasreen (2013). Factors Influencing Stillbirth in <scp>B</scp>angladesh: A Case–Control Study.
Rakhi Dandona,G Kumar,M Akbar,Debarshi Bhattacharya,Priya Nanda,Lalit Dandona (2019). Deferred and referred deliveries contribute to stillbirths in the Indian state of Bihar: results from a population-based survey of all births.
E Archibong,A Sobande,A Asindi (2003). Antenatal intrauterine fetal death: a prospective study in a tertiary hospital in south-western Saudi Arabia.
M Jahani (2015). Factors Affecting Stillbirth Rate in the Hospitals Affiliated to Babol University of Medical Sciences.
Banke-Thomas A Ac,U Gwacham-Anisiobi (2021). Influence of travel time and distance to the hospital of care on stillbirths: a retrospective facility-based cross-sectional study in Lagos, Nigeria.
Okonofua (2019). Prevalence and determinants of stillbirth in Nigerian referral hospitals: a multicentre study.
Georg Macharey,Mika Gissler,Leena Rahkonen,Veli-Matti Ulander,Mervi Väisänen-Tommiska,Mika Nuutila,Seppo Heinonen (2017). Breech presentation at term and associated obstetric risks factors—a nationwide population based cohort study.
László Zsirai,György Csákány,Péter Vargha,Vilmos Fülöp,Ádám Tabák (2016). Breech presentation: its predictors and consequences. An analysis of the Hungarian Tauffer Obstetric Database (1996–2011).
Neamin Tesfay,Frehiwot Legesse,Mandefro Kebede,Fitsum Woldeyohannes (2022). Determinants of stillbirth among reviewed perinatal deaths in Ethiopia.
Atrsaw Liyew,Mihretu Molla,Zelalem Azene (2021). Risk Factors of Stillbirth Among Women Who Gave Birth in Amhara Region Referral Hospitals, Ethiopia, in 2019: A Case-Control Study.
H Litorp,A Sunny,A Kc (2021). Augmentation of labor with oxytocin and its association with delivery outcomes: A large-scale cohort study in 12 public hospitals in Nepal.
Jason Collins (2012). Umbilical cord accidents.
Kc (2015). Risk factors for antepartum stillbirth: a case-control study in Nepal.
Reiharuyam (4117). Causes and risk factors for singleton stillbirth in Japan: Analysis of a nationwide perinatal database, 2013-2014.
Sutapa Neogi,Jyoti Sharma,Preeti Negandhi,Monika Chauhan,Siddharth Reddy,Ghanashyam Sethy (2018). Risk factors for stillbirths: how much can a responsive health system prevent?.
Haimanot Abebe,Solomon Shitu,Haile Workye,Ayenew Mose (2021). Predictors of stillbirth among women who had given birth in Southern Ethiopia, 2020: A case-control study.
Basso Ananth (2010). Impact of Pregnancy-Induced Hypertension on Stillbirth and Neonatal Mortality in First and Higher Order Births: A Population-Based Study.
Tao Xiong,Yi Mu,Juan Liang,Jun Zhu,Xiaohong Li,Jinke Li,Zheng Liu,Yi Qu,Yanping Wang,Dezhi Mu (2018). Hypertensive disorders in pregnancy and stillbirth rates: a facility-based study in China.
Abadi Berhe,Abiodun Ilesanmi,Christopher Aimakhu,Afework Mulugeta (2020). Effect of pregnancy induced hypertension on adverse perinatal outcomes in Tigray regional state, Ethiopia: a prospective cohort study.
Telksew Yezengaw,Tariku Dingeta,Tesfaye Assebe,Biruk Tusa (2022). Stillbirth and Its Association with Early rupture of Membranes in Sub-Saharan Africa: Systematic Review and Meta-Analysis.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Hailemichael. 2026. \u201cPrevalence and Determinants of Stillbirth among Women Attended Deliveries in Dekemhare Hospital: Case-Control Study\u201d. Global Journal of Medical Research - E: Gynecology & Obstetrics GJMR-E Volume 23 (GJMR Volume 23 Issue E1): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































