I. INTRODUCTION
Anemia is a public health problem that affects a large number of people throughout the world, especially pregnant women. It is a condition characterized by a reduction in the number of red blood cells and a fall in the concentration of hemoglobin (Hb) in the blood to the threshold of in pregnant women (Hallberg et al., 2001; WHO, 2001). Various markers are used to assess iron status: Hb can be considered as the circulating form of iron, while ferritin and transferrin receptor saturation levels reflect the state of the body's iron reserves. The interpretation of these markers is complex (Diouf et al., 2015). It is a major public health problem in the world in general and in developing countries in particular (WHO, 2011; Sanogo, 2012; Diouf et al., 2015). It affects more than 3.5 billion people in developing countries, or , compared with just in developed countries (Baily, 2017). Women of childbearing age, particularly pregnant women and children, are the groups at highest risk. The prevalence observed in developing countries is high: of children aged 1-5 years, of women of childbearing age and of pregnant women (WHO, 2021). Table I shows the criteria used to classify anemia according to age and sex.
| Hemoglobin rate (g/dl) | |
| Children < years | < 11 |
| Women | < 12 |
| Pregnant women | < 11 |
| Men | < 13 |
Table II shows the thresholds adopted by the WHO for reporting anaemia according to age, sex and gestational status.
Table II: Hemoglobin Levels for Diagnosing Anemia in the Mother (g/l)
| Population | Anemia* | |||
| No anemia | lighta | moderate | severe | |
| Children aged 6 to 59 months | 110 or over | 100-109 | 70-99 | Under 70 |
| Children aged 5 to 11 years | 115 or over | 110-114 | 80-109 | Under 80 |
| Children aged 12 to 14 ans | 120 or over | 110-119 | 80-109 | Under 80 |
| Non-pregnant women (15 years and over) | 120 or over | 110-119 | 80-109 | Under 80 |
| Pregnant women | 110 or over | 100-109 | 70-99 | Under 70 |
| Men (aged 15 and over) | 130 or over | 100-129 | 80-109 | Under 80 |
Table III shows the thresholds proposed by the US Centers for Disease Control and Prevention (CDC) for reporting anemia during the weeks of gestation and the three trimesters of pregnancy.
Table III: Thresholds for Reporting Anemia in Pregnant Women According to the CDC
| Pregnancy weeks | Hemoglobin level (g/dl) |
| 16 | 10,6 |
| 20 | 10,5 |
| 24 | 10,5 |
| 28 | 10,7 |
| 32 | 11 |
| 36 | 11,4 |
| 40 | 11,9 |
| Pregnancy trimester | |
| Second | 10,5 |
| Third | 11 |
The main cause of maternal anaemia in Africa is a lack of iron, which is essential for the formation of red blood cells, and folate. Between and of pregnant women in malarious regions are anemic (De Benoist et al., 2008; Menon, 2016). However, nutritional deficiencies in certain nutrients such as vitamin A, folic acid and vitamin B12 can lead to anaemia (WHO, 2007). Worldwide, an estimated of pregnant women suffer from anaemia. In developing countries, the prevalence of iron deficiency varies between and , or more than 500 million women of childbearing age. This prevalence is higher in areas where parasitic infections are highly endemic (WHO, 2011). Pregnant women's iron requirements increase during pregnancy, rising from per day in the first trimester to per day in the second trimester and per day in the final trimester, which is why special attention needs to be paid to these women.
Although all infections can lead to anemia, intestinal helminth infections, malaria, schistosomiasis and acquired human immunodeficiency virus (HIV) infection are the main causes of anemia in the intertropical zone (Sylvianne, 2016).
Helminthiasis are parasitic diseases caused by intestinal parasitic worms known as helminths. Hookworm, ascariasis and trichocephalosis are the intestinal helminth infections responsible for anaemia (Larocque et al., 2005). Of these three parasitic diseases, hookworm infection, with predominantly digestive and haematological manifestations, has been the most widely described as responsible for anaemia (Smith and Brooker, 2010). It is widespread in all hot and humid, tropical and subtropical areas, mainly in sub-Saharan Africa and South-West Asia, affecting 576 to 740 million people (Bethony et al., 2006). Hookworms are more anemic than roundworms and whipworms.
Malaria remains the most important parasitosis. of malaria cases are recorded in sub-Saharan Africa (WHO, 2011), where Plasmodium falciparum is the most widespread and pathogenic species that can lead to severe anaemia (Menendez et al., 2000).
Malaria infection during pregnancy is associated with anaemia, an increased risk of severe malaria and serious fetomaternal complications such as spontaneous abortion or prematurity (WHO, 2019). Gestational malaria is responsible for of stillbirths in sub-Saharan Africa (Toussaint, 2012).
Schistosomiasis, the world's second most common parasitic endemic after malaria, bilharziasis or schistosomiasis is a chronic, debilitating disease. Over of reported cases occur in sub-Saharan Africa, and the predominant species is Schistosoma haematobium
(Friedman et al., 2005). Four mechanisms have been proposed to explain this relationship. These include iron wastage, splenic sequestration of red blood cells, autoimmune haemolysis and inflammatory anaemia (Friedman et al., 2005).
Anaemia is one of the complications associated with Human Immunodeficiency Virus infection (Volberding et al., 2004). This complication most often affects women and children in sub-Saharan Africa (Calis et al., 2008). The anaemia observed during HIV infection may be due either to neoplastic infiltration of the bone marrow or to immunological phenomena responsible for haemolytic anaemia. HIV infection can also have an indirect effect on blood haemoglobin concentration by increasing the patient's susceptibility to various infections, particularly those caused by Plasmodium falciparum, which in turn causes anaemia (Verhoeff et al., 1999). Finally, the anaemia observed during this infection may be a side effect of antiretroviral drugs, mainly zidovudine, a drug in the nucleotide reverse transcriptase inhibitor class. Other causes of anaemia can be genetic. Genetic abnormalities responsible for anaemia include sickle cell disease and thalassaemia (Modell and Darlison, 2008), Glucose-6-phosphate dehydrogenase (G6PD) deficiency (Luzzatto et al., 2001) and ovalocytosis in regions where malaria is endemic in Africa and Asia (Bossi and Russo, 1996).
The consequences of iron deficiency in pregnant women could increase the risk of maternal morbidity and mortality, foetal mortality or the risk of having a low birth weight baby (WHO, 2008; Harvey et al, 2016).
Reducing the prevalence of iron deficiency is one of the major objectives of public health policies in developing countries. In conjunction with international organisations and non-governmental structures, they are seeking to implement interventions, the majority' of which target young children and women of childbearing age (Diouf et al., 2015).
According to the same authors, anaemia and iron deficiency stem from a complex aetiology, and comprehensive action on all the factors involved (infections, parasitism, malnutrition) is surely the most effective approach, but undoubtedly the most difficult to implement today. Programmes focused on increasing dietary iron intake seem more accessible, although their large-scale implementation often remains a challenge. In addition to approaches aimed at encouraging the consumption of iron-rich foods by improving incomes and education, there is interest in supplementation and fortification programs (Mannar, 2006). In all cases, effective communication must be put in place as close as possible to the populations concerned to promote the success of the program, which always involves changing habits and convincing them of the merits (Mannar, 2006).
Given our current state of knowledge, very few studies have been carried out on the correlation between iron status and dietary habits in pregnant women at Guelendeng District Hospital.
This study aims to determine the prevalence of anaemia in pregnant women admitted for consultation to the maternity at Guelendeng District Hospital, and to contribute to nutritional advice on good nutrition for pregnant women.
II. MATERIALS AND METHODS
1. Materials
1.1 Study Area and Setting
The study was carried out in the town of Guelendeng. Located between North and East, Guelendeng District Hospital is situated in the north of the town, about 3 km along the Guelendeng-N'Djamena road. It is a public facility built in 2007 with co-funding from Chad and the European Union, and covers an area of . It has been operational since 2010. It includes the following Departments: Medicine, Surgery, Maternity, Pediatrics, Nutrition Therapeutic Unit (UNT), Laboratory, Reference Consultation Room, Administration and Pharmacy block, accommodation for the District Medical Officer (MCD) and the midwife in charge of the maternity ward. The Guelendeng health district has an estimated population of 120,860, according to Chad's second General Population and Housing Census (RGPH2). It has twelve (12) health centers, two of which are non-functional. The maternity in this district was used as the setting for the study.
1.2 Study Type and Period
This was a cross-sectional, forward-looking study covering a 3-month period from November 2022 to February 2023.
1.3 Biological Material
The biological material consisted of all blood samples from pregnant women attending antenatal consultation at the maternity of the Guelendeng District Hospital, for whom a blood count examination test (NFS) had been prescribed and found to be positive (Hb level strictly less than ).
1.4 Laboratory Technical Equipment
The equipment to be used was packaged in such a way as to ensure that the blood samples taken were not contaminated. These included non-coagulating tubes, hypodermic needles, medical syringes, tourniquets, alcohol, cotton wool, gloves and a gown. The equipment consisted of a Hemocue and a Mindray-BC 3000 plus photometer. Blood samples were taken by laboratory technicians.

2. Methods
2.1 Study Population
The study population consisted of pregnant women attending antenatal consultation at the maternity of the Guelendeng District Hospital.
Inclusion Criteria
The Study Included:
- All women who came to the maternity and had a positive pregnancy test (urine, blood or ultrasound);
- All pregnant women of any age who consented to the study, regardless of the age of their pregnancy;
- All pregnant women presenting clinical signs suggestive of anaemia or not, for whom a blood count examination test (NFS) was prescribed and whose result showed an Hb level strictly below .
Non-Inclusion Criteria
All women who did not meet the inclusion criteria were excluded from the study.
2.2 Sampling
Sampling consisted of exhaustive and consecutive recruitment of all pregnant women who met the inclusion criteria and were admitted to the maternity hospital during the 3-month study period. We were therefore able to recruit 67 pregnant women, 50 of whom were presumed anemic during the study period.
2.3 Ethical and Administrative Considerations
Initially, we obtained a research authorization from the Bongor Teachers' Training Higher School. We then went to the administration of the Guelendeng District Hospital to obtain authorization for a research placement. The verbal consent of the pregnant women surveyed was obtained before any data was collected, and we were bound by strict confidentiality.
2.4 Studied Variables
The main study variables were: sociodemographic and socio-economic characteristics, and anaemia and malaria test results.
2.5 Hematological Parameters
A blood count examination test (NFS) and hemoglobin levels were carried out at the Guelendeng
District Hospital laboratory. The blood count examination was carried out using an appropriate device called a Mindray-BC 3000 plus photometer, which automatically counts all the elements in the blood from a blood sample taken.
2.6 Conduct of the Study
During the study, we enlisted the services of a midwife who had been trained in the diet of pregnant women. After explaining the purpose of the research to the pregnant women and obtaining their consent, the women who met the inclusion criteria were interviewed using a survey form.
2.7 Pre-Testing
The survey form was pre-tested with 10 pregnant women of all ages who had undergone biological tests. This gave us an idea of how well the various questions were understood, and enabled us to reformulate the survey form.
2.8 Survey Form
A questionnaire structured in 2 main parts was used to collect the data:
- The first part dealt with the socio-demographic characteristics of the pregnant woman;
- The second part provided information on the socioeconomic characteristics of the pregnant woman;
2.9 Data Processing and Analysis
Word 2010 was used to draw up the questionnaire and collect the data. Excel 2010 was used to draw the graphs. The data collected was analyzed using Excel 2010 and processed using SPSS, Statistics 25.
III. RESULTS AND DISCUSSION
1. Results
We were able to survey a total of 67 pregnant women, 50 of whom showed signs of anaemia. The results of the hemoglobin tests (Hb level ) confirmed that 27 women were anemic out of the 50 presumed to be anemic. These results are presented below in the form of figures and tables.
1.1 Socio-Demographic And Socio-Economic Characteristics of Respondents
1.1.1 Distribution of Pregnant Women with Anaemia by Age Group
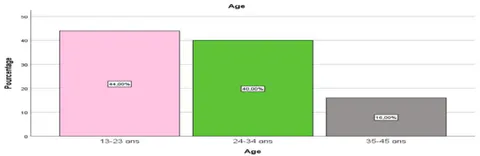
The figure shows that the most represented age group is between 13 and 23, with , followed by 25 to 34 ; the least represented age group is 35 to 45, with . The anemic pregnant women at the extremes of age in the study were aged 13 and 45.
1.1.2 Financial Income Variable
Figure 2 shows the distribution of pregnant women surveyed according to their families' monthly financial income.
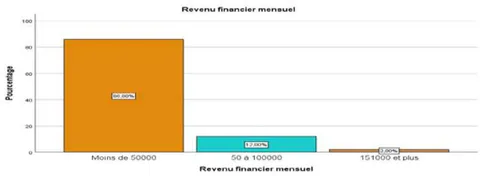
According to the results of the survey, of the women come from families with a monthly financial income of less than 50,000 FCFA. This implies that the majority of women in the study come from poor and vulnerable families. This result also shows that of the women in the study come from families with financial incomes of between 50 and 100,000 FCFA.
1.1.3 Level of Education of the Women Surveyed
Figure 3 shows the distribution of anemic pregnant women in the study according to their level of education.
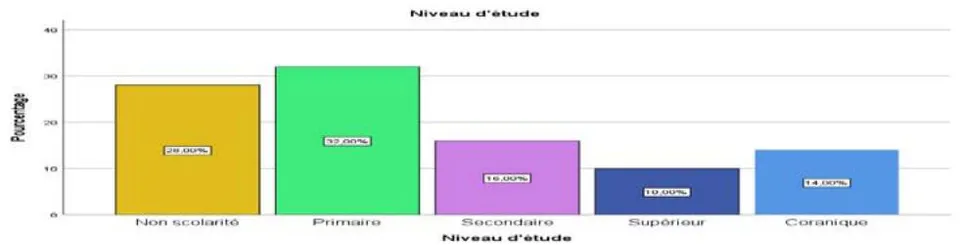
The results of the study show that almost a third of the women surveyed had attended primary school , followed by those who had not . These two groups account for of pregnant women with anaemia. This may have an impact on the lack of knowledge about balanced diets to ensure good nutritional status for the woman and her unborn baby.
Next come women who have attended secondary school (16%) and Koranic school (14%). Pregnant women with anaemia who had attended higher education represented only 1/10 of the women in the study.
1.1.4 Variable Linked to Ethnic Origin
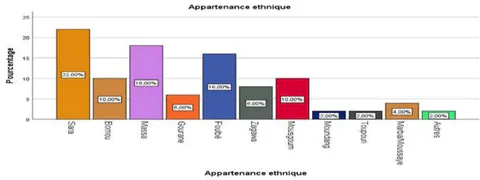
The results of the study show that more than ten ethnic groups live together in the town of Guelendeng, with the majority of pregnant women with anaemia belonging to the Sara ethnic group (22%), followed by the Massa (18%). Next come the Peuhls (16%), followed by the Mousgoum and Bornou at 10% each. and others at 2% each. Zagawa women are represented in the survey at 8%, Gouranes at 6% and Marbas/Mousseys at
4%. The least represented ethnic groups in the study are the Moundang and Toupouri, with 2% each.
1.1.5 Antenatal Consultation
Figure 5 shows the distribution of anemic pregnant women according to their attendance at antenatal consultation.
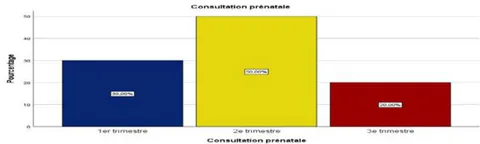
Figure 5 shows that most pregnant women (50%) do not attend antenatal clinics until the second trimester of their pregnancy, while 30% do so from the first trimester onwards, compared with 20% who attend in the third trimester.
1.1.6 Profession of Anemic Pregnant Women Surveyed These results are shown in Figure 6 below.
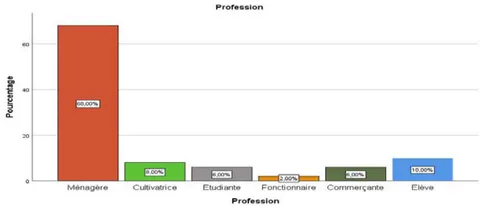
The results summarized in Figure 6 above show that of anemic pregnant women were housewives, followed by students and then farmers . Pregnant women with anaemia who were students and shopkeepers each accounted for only of the women in the study. Only of pregnant women with anaemia were civil servants.
1.1.7 Variable Related to Water Supply Sources
Figure 7 shows the distribution of the women in the study by source of water supply.
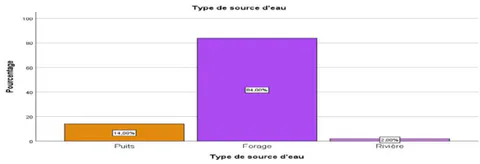
The figure shows that of women get their water from boreholes, followed by of women who get their water from wells. Of the women surveyed, obtained their water from rivers.
1.1.8 Variable Linked to the Type of House Lived in
Figure 8 shows the results of the survey according to the type of house lived in by the women surveyed.
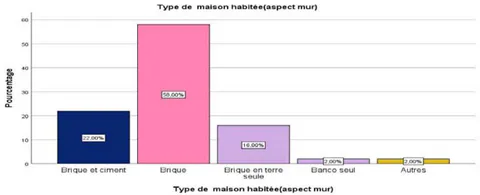
The above results show that of the women surveyed sleep in houses built of brick, sleep in houses built of brick and cement. We also note that of these women sleep in houses built of mud bricks, while sleep in houses built of bingo. In our opinion, houses built of mud bricks and bingo, when not plastered smooth, are breeding grounds for mosquitoes.
1.1.9 Variable Linked to the Number of People in the Respondent's Family
Figure 9 shows the distribution of women surveyed according to the number of people living in the respondent's family.
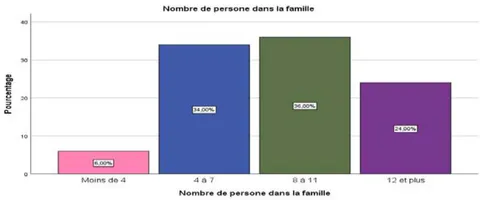
The results show that of the women surveyed come from families with between 8 and 11 members, followed by of pregnant women from families with between 4 and 7 members, and finally women living in families with 12 or more members . The survey results show that only of the women surveyed were from families with fewer than 4 members.
1.2 Hemoglobin Test Results
1.2.1 Hemoglobin Test Results Per 10 Pregnant Women Surveyed
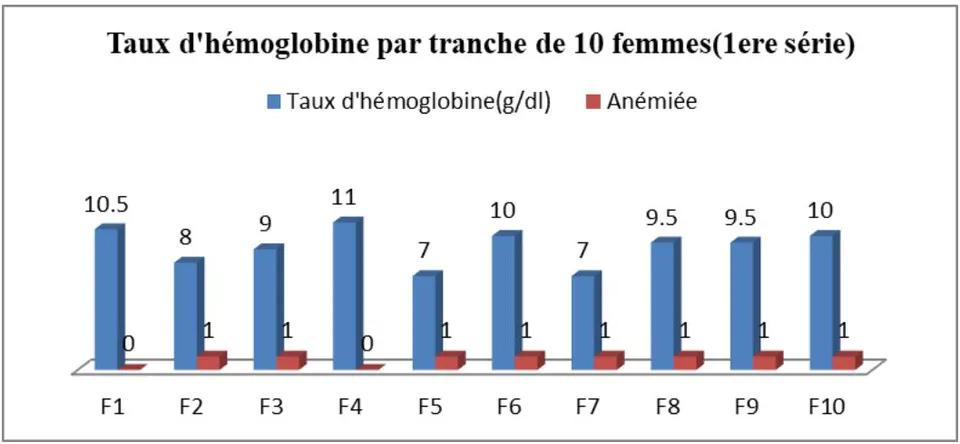
Figure 10 shows that hemoglobin levels varied from one woman tested to another, with a maximum of and a minimum of in the first series. Of the 10 women tested, 8 were anemic with hemoglobin levels .
1.2.2 Hemoglobin Test Results for the Second Series of 10 Women Surveyed
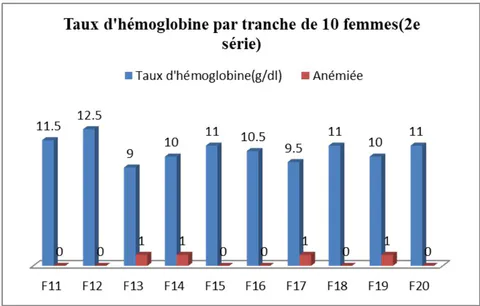
Figure 11 shows that hemoglobin levels varied from to in the second series, with 4 out of 10 women being anemic. Thus, out of 50 women in the study with signs of anemia divided into five series of ten women, 27 were confirmed as anemic.
1.3 Prevalence (P) of Anemia in Pregnant Women Attending The Maternity Ward of Guelendeng District Hospital Prevalence is determined by the following formula:
Applying the above formula, the calculated prevalence of anemic pregnant women at Guelendeng District Hospital is .
1.4 Malaria Test Results
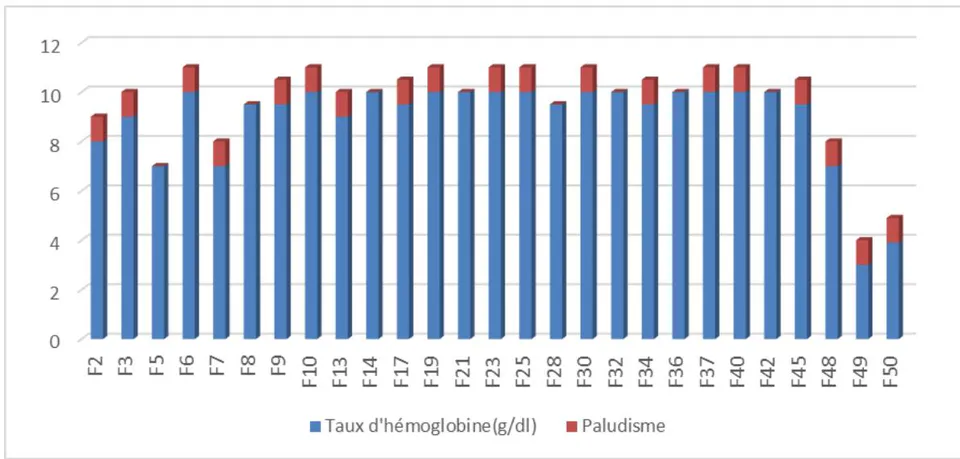
According to the results of the study, of the 27 women with anemia, 19 tested positive for malaria, a percentage of .
2. Discussion
The results of this study showed that the age group most represented among anemic pregnant women is the 13-23 age group (44%), followed by the 25-34 age group (40%). Early marriages from the age of 13 should be discouraged, as these women enter the intergenerational cycle of malnutrition. The 18 to 23 age group corresponds to the age group during which women are more active in terms of reproduction. Nadia et al. (2018) in Morocco observed a significant difference between the mother's age and the onset of anemia. They explain this significance by the fact that mothers have different eating habits depending on their age. Mothers who are very young (19 years) lack the maturity, skills and, above all, nutritional experience that would enable them to eat well and look after themselves.
According to the results of our survey, of the women were from families with a monthly income of less than 50,000 FCFA. This implies that the majority of women in the study come from poor and vulnerable families, and therefore lack the necessary means to obtain a sufficient, balanced diet that can prevent anemia. Income level is also associated with anemia prevalence: children from low-income families are more often anemic than those from better-off households (79.8% compared with 62.3%; p = 0.0015 [Student's t test]) (Diouf et al. 2015).
In terms of level of education, almost a third of the women surveyed had attended primary school , followed by those with no schooling . These two groups account for of pregnant women with anemia. This may have an impact on the lack of knowledge about balanced diets to ensure good nutritional status for pregnant women and their unborn babies. The mother's low level of education is a factor that favours the onset of anemia in pregnant women. This is due to the fact that they have little capacity to learn and practice the skills involved in good nutrition.
Half of the pregnant women in the study did not go for antenatal check-ups until the second trimester of their pregnancies, while did so from the first trimester onwards, compared with who went for check-ups in the third trimester. Regular antenatal check-ups for pregnant women, combined with the presence in maternity wards of midwives trained in the nutrition of pregnant women, and the financial resources of families, is a winning bet in the fight against anemia.
The results of the study show that of anemic pregnant women are housewives, followed by schoolgirls . These women are financially vulnerable and dependent on their husbands' financial situation. Charlotte et al (2016) in Douala, Cameroon, obtained results contrary to ours. The majority of anemic pregnant women in their study had a higher level of education (279 cases or ). Salaried women were the most represented (240 cases or ) in their study.
In our study, of women obtained their water from boreholes, followed by from wells. Of the women surveyed, obtained their water from a river. Helminthiasis and schistosomiasis, which are often linked to water, can cause anemia.
The results of the study show that of the women surveyed come from families with between 8 and 11 members, followed by of pregnant women from families with between 4 and 7 members, and finally women living in families with 12 or more members . In most cases, a large family in Chad means not enough food for everyone.
Our calculated prevalence of of pregnant women with anemia is higher than the average for Central Africa, according to the results of Diouf et al. (2015): health survey reports (DHS) indicate that, on average over 9 countries in the zone; of women (pregnant or not) aged 15 to 49 are anemic. Our results are also superior to those obtained by Charlotte et al. (2016) in Douala, Cameroon: 415 pregnant women were recruited. The prevalence of anemia was . On the other hand, the prevalence obtained in Morocco by Kazouini (2021) is higher than our result (272 cases of iron deficiency anemia, i.e. of anemias recorded).
IV. CONCLUSION
At the end of our study, we can conclude that the prevalence of anaemia is high among pregnant women in the maternity ward of the Guelendeng District Hospital in Chad. It is within the range of WHO data for 2021 for developing countries. Almost three quarters of the anaemic women in the study tested positive for malaria.
The study also revealed that antenatal consultations by pregnant women were low, and of those who did attend, they claimed to be unaware of nutritional advice. Almost all the women in the study live in large families.
The low level of education, low monthly income, large families in which the women surveyed live and poor antenatal care are just some of the risk factors for anemia in pregnancy.
As women's attendance at antenatal clinics and maternity wards at Guelendeng District Hospital is low and the study sample small, these results cannot be generalized to Chad.
ACKNOWLEDGEMENTS
We would like to thank the people who helped us with this study: the Guelendeng District Medical Officer, Dr. Serge NANGOYOUM; the midwife, Mrs NADJIGA DJENOM, in charge of the maternity unit; the head laboratory technician, Mr ADOUM NODJINGAR; and all those who are not mentioned by name.