## I. BACKGROUND
Many urologists in underdeveloped nations in Africa have the choice of surgical treatment or an indwelling urinary catheter because the majority of adult males with LUTS caused by BPH present late and have related comorbidities. $^{(1)}$ Storage symptoms, formerly known as irritative symptoms (frequency, urgency, and nocturia), and voiding symptoms, formerly known as obstructive symptoms (hesitancy, weak urine stream, intermittency, straining, and terminal dribbling) are the two categories for lower urinary tract symptoms caused by BPH. and postmicturition sensations (such as dribbling and a sense of incomplete emptying). $^{(2)}$
When these patients first arrive, their main concern is to have their LUTS and BPH-related discomfort addressed. For this to be done successfully, accurate assessments of these patients and their classification using a validated scoring system are required. The most often used measurement for this is the International Prostate Symptom Score (IPSS).[3]
The symptoms are compiled and divided into three categories: mild (0-7), moderate (8-19), and severe (20-35). The following situations would benefit from the usage of a trustworthy IPSS: the classification of patients into various treatment modes, the exchange of information between patients and physicians, the recording of treatment outcomes, and the comparison of various treatment modalities. $^{(3)(4)}$
In carefully chosen patients, transurethral resection of the prostate (TURP) is the gold standard for treating symptomatic BPH. The medication helps to improve the quality of life score and resolve LUTS brought on by BPH. $^{(5)(6)}$
The purpose of this study was to evaluate the remission of LUTS caused by BPH following TURP in patients at our center using the IPSS, its voiding and storage symptoms sub score, and QoLS.
## II. METHODS
### a) Study Design
In the Institute of Urology of KCMC Moshi, Tanzania, patients who underwent TURP for symptomatic BPH participated in this 6-month hospital prospective observational study.
### b) Study Population and Data Sources
All symptomatic BPH patients who underwent TURP between June 2021 and January 2022. To rule out any possible differential diagnoses for BOO, the chosen patients underwent appropriate diagnostics, a history review, and physical examination. Trucut prostate biopsies are performed and sent for histological evaluation in patients with serum PSA levels greater than $4\mathrm{ng / ml}$ and/or suspect DRE. To maintain uniformity, the translated IPSS was administered by a specific author who was fluent in the subject's original tongue (by a physician). Prostate transurethral resection was carried out while sedated. The same author who gave the preoperative IPSS reviewed them with IPSS in the clinic one month after the TURP. This was reiterated over the phone three months after the TURP.
The KCMUCo Research and Ethical council and the Institute of Urology at KCMC, respectively, provided their approval and consent for the conduct of this study from a retrospective evaluation. Information about the patients was kept completely private: In this investigation, no specific patient identifiers were employed.
### c) Outcomes and Explanatory Variables
Irritable and obstructive symptoms (LUTS) were the primary study outcome, and IPSS, QoLS, Storage, and Voiding were used as the study's explanatory variables.
### d) Statistical Analysis
The IPSS, QoLS, storage, and voiding sub scores were compared before and after 3 months after TURP using the paired t-test.
## III. RESULTS
The final data analysis included 156 patients who had had TURP in total. Table 1 displays the demographics of the patients. The majority of the patients had mean ages of 66, 6.7, 54.7, 13.1, and 24.2, 7.5, respectively, for prostate volume and weight of tissue removed. Baseline IPSS values for QoLS, storage, and voyaging were 28(21,31), 6(5,6), 12(11,13), and 16(14,18), respectively. Following a three-month follow-up, the overall IPSS score, QoLS, and both of its subscores (storage and voiding domain), all experienced significant declines.
There was less decline in the voiding sub score when comparing the median change in storage and voiding sub scores. This research demonstrates that the storage sub score changes more frequently after TURP than it does after voiding and may return to normal.
Table 1: Background characteristics of study participants (N= 156)
<table><tr><td>Characteristic</td><td>Frequency</td><td>Percentage</td></tr><tr><td>Age</td><td></td><td></td></tr><tr><td>60 and below</td><td>29</td><td>18.6</td></tr><tr><td>Above 60</td><td>127</td><td>81.4</td></tr><tr><td>Mean±SD</td><td></td><td></td></tr><tr><td>66±6.7</td><td></td><td></td></tr><tr><td>Education level</td><td></td><td></td></tr><tr><td>No/Primary education</td><td>47</td><td>30.1</td></tr><tr><td>Secondary education & above</td><td>109</td><td>69.9</td></tr><tr><td>Prostate volume (mls)</td><td></td><td></td></tr><tr><td>40 and below</td><td>29</td><td>18.6</td></tr><tr><td>Bove 40</td><td>127</td><td>81.4</td></tr><tr><td>Mean±SD</td><td></td><td></td></tr><tr><td>Weight of resected tissue (gm)</td><td></td><td></td></tr><tr><td>25 and below</td><td>93</td><td>59.6</td></tr><tr><td>Above 25</td><td>63</td><td>40.4</td></tr><tr><td>Mean±SD</td><td></td><td></td></tr><tr><td>24.2±7.5</td><td></td><td></td></tr></table>
Table 2: Comparison of outcomes before and after (Median used)
$\left( {\mathrm{N} = {156}}\right)$
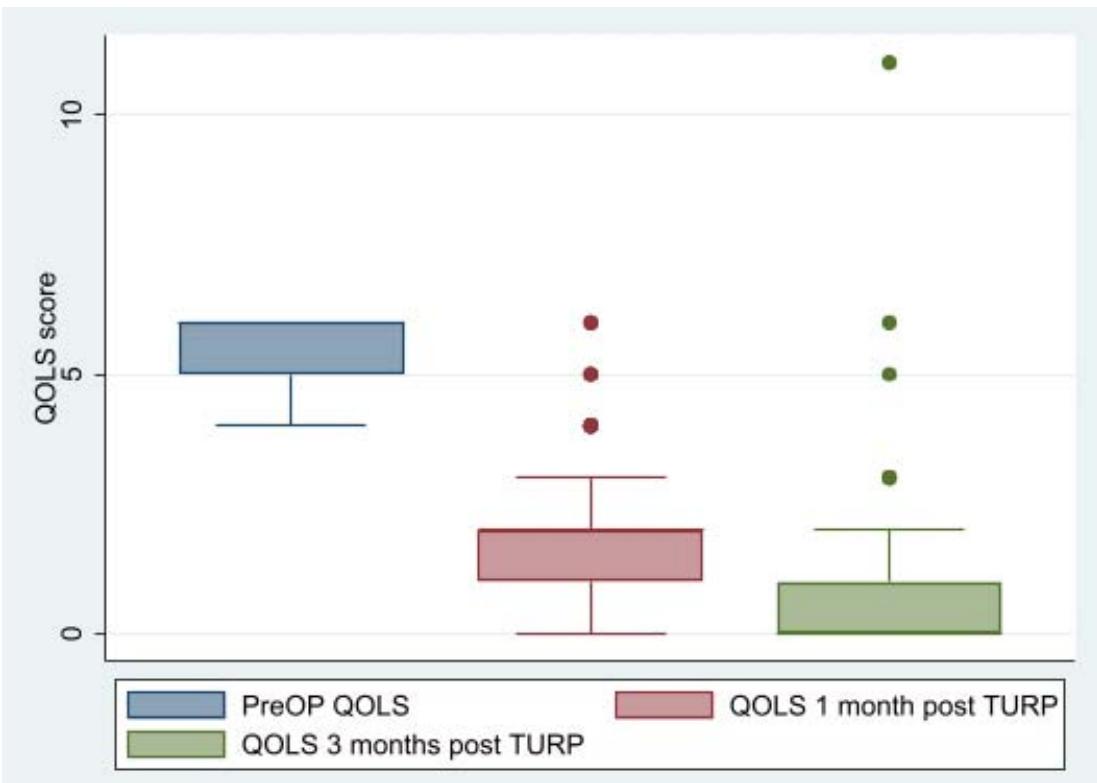
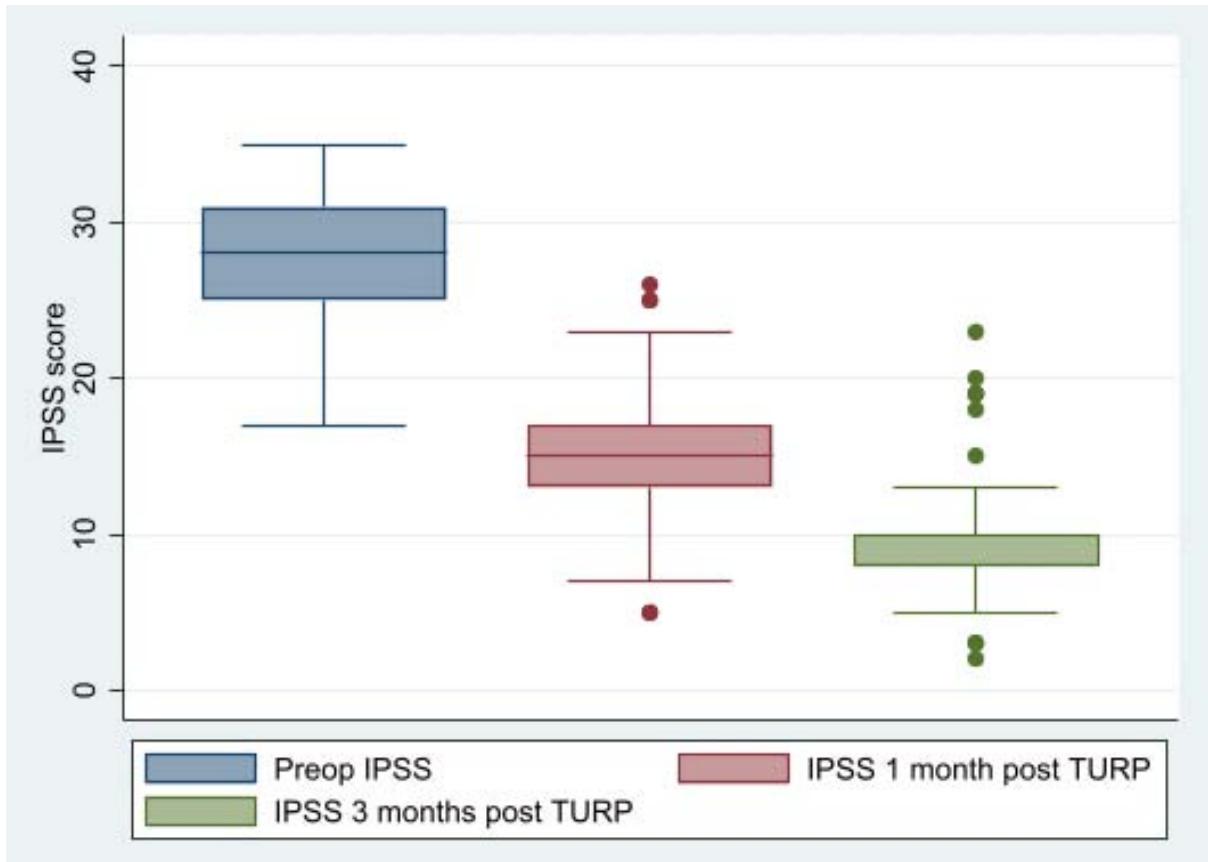
<table><tr><td>Characteristic</td><td>PreOP</td><td>1 month post TURP</td><td>3 months post TURP</td></tr><tr><td>IPSS</td><td>28 (25,31)</td><td>15 (13, 17)</td><td>8 (8,10)</td></tr><tr><td>QOLS</td><td>6 (5, 6)</td><td>2 (1, 2)</td><td>0 (0, 1)</td></tr><tr><td>Storage</td><td>12 (11, 13)</td><td>6 (5, 7)</td><td>4 (3, 4)</td></tr><tr><td>Voiding</td><td>16 (14, 18)</td><td>8 (7, 10)</td><td>5 (4, 6)</td></tr></table>
Comparison of outcomes (graphical presentation)
IPSS
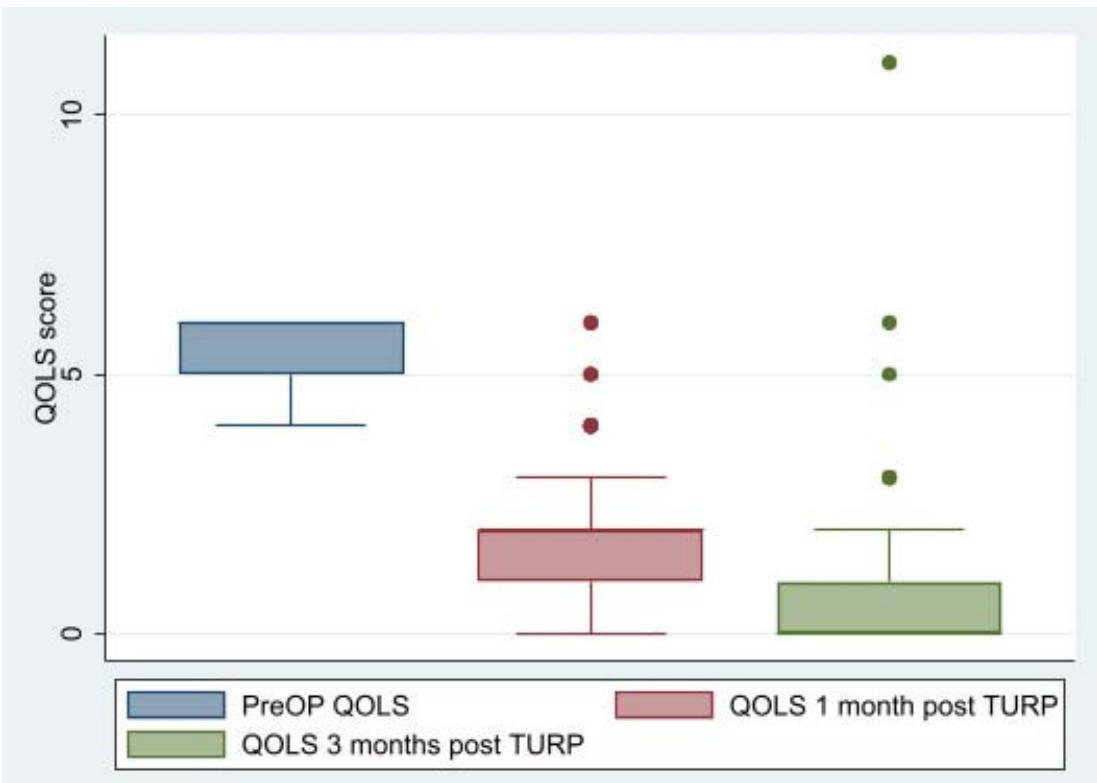 Panel label: QOLS.
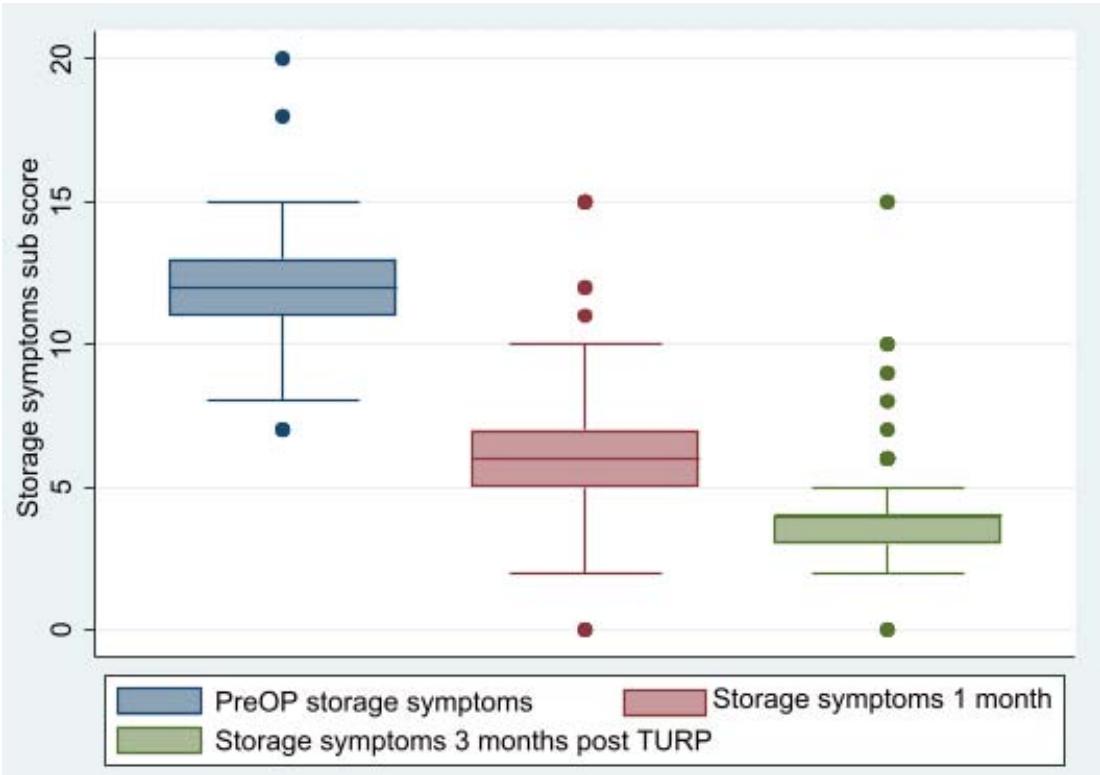 Panel label: Storage.
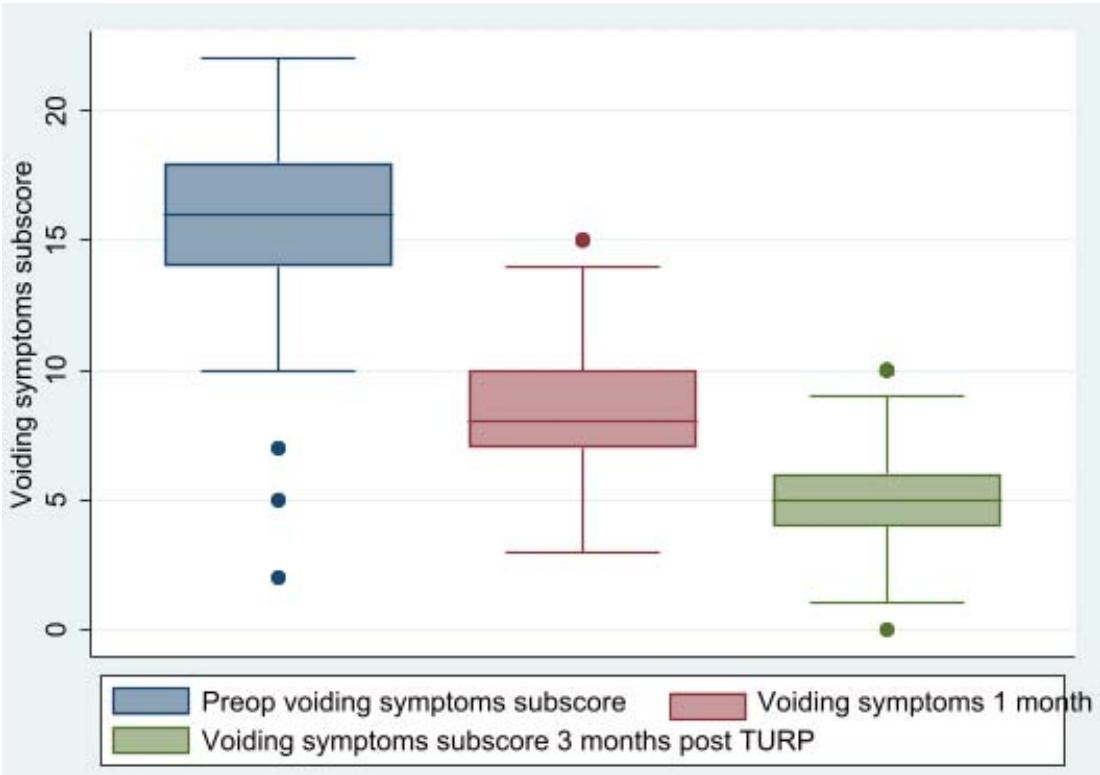 Voiding
## IV. DISCUSSION
This study is the first on LUTS resolution following TURP to be conducted at our center. Despite the obstruction being removed, some alterations that arise inside the bladder as a result of BPO might not return to normal. According to this study, the majority of TURP patients were in their sixth decade of life, had severe LUTS, and had a low quality of life as a result of unpleasant symptoms. Patients who had undergone TURP had an average prostate size of 54.7gm. In recent investigations, men who had undergone TURP had prostate volumes ranging from 46.1gm to 60gm.[7] The average age of the TURP patients was around 66 years old, which is similarly comparable to the data from Gacci et al., who found that the average age was 68 years old.[8] This findings confirm the validity of enlargement of prostate disease of the elderly male.
Before TURP, the study's overall IPPS was 28(21,31), and QOLS was 6(5,6). This result differs from the study conducted in Italy, where preoperative IPPS and QoLS were respectively 19.6 and 3.41, and the study conducted by Luite et al. in Nepal, where preoperative IPPS was 24.66 and QoLS was 5.10.9. This result demonstrates that our population's preoperative IPPS and QoLS are greater than those of patients in the European and Western globe. This may be due to our patients' delayed presentation, and some of our clients even believe that LUTS is a symptom of aging and refuse medical attention.[7] In our study, the baseline score for storage symptoms was 12 (11, 13), which decreased to 4 (3, 4) 3 months after TURP, with a net change of -8 (8, 9). But this decrease in storage symptoms happens far more frequently than voiding symptoms. The results of the study indicate that post-TURP changes in storage symptoms sub-score occur more frequently than changes in voiding symptoms, and those changes in voiding may return to normal, while other alterations that take place inside the bladder as a result of BPO may not, even after the obstruction is removed. In contrast to the study by Chalise et al., obstructive symptoms improve much more (82.4%) than irritable symptoms (46.3%) following TURP.(7) Kang YJ et al.'s study demonstrates that patients with diabetes who had improved storage symptoms.(5)
## V. CONCLUSION
Reduction in IPSS, QoLS, and its subscore after TURP. Greater than voiding symptoms is the newer storage score. As a result, TURP continues to be the gold standard of care for patients with LUTS caused by BPE. However, greater health promotion efforts are needed to encourage patients to arrive at the urology clinic on time.
### ACKNOWLEDGMENTS
Generating HTML Viewer...
References
8 Cites in Article
L Stothers,S Mutabazi,R Mukisa,A Macnab (2016). The burden of bladder outlet obstruction in men in rural Uganda.
O Amu,E Udeh,A Ugochukwu,N Dakum,V Ramyil (2013). The value of international prostate symptom scoring system in the management of bph in jos, nigeria.
J Michael,Barry (1992). Bukht, Mirza Michael John, (Michael Barry), (10 Sept. 1941–4 Aug. 2011), food journalist; Programme Controller, Classic FM Radio, 1992–97.
J Bae,H Kang,H Lee,K Lee,M Cho (2016). Predictors of de novo urge urinary incontinence after photoselective vaporization of the prostate.
S Anutrakulchai (2005). Residual LUTS after Transurethral Resection of Prostate (TURP): The Urodynamic Studies in Chiangmai University.
B Luitel,D Gupta,P Chalise,P Subedi,S Chapagain,U Sharma,P Gyawali,G Shrestha,B Joshi (2016). Change in storage symptoms after transurethral resection of prostate: a prospective observational study.
M Gacci,R Bartoletti,S Figlioli,E Sarti,B Eisner,V Boddi,M Rizzo (2003). Urinary symptoms, quality of life and sexual function in patients with benign prostatic hypertrophy before and after prostatectomy: a prospective study.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Mbarouk Mohammed. 2026. \u201cResolution of Lower Urinary Tract Symptoms due to Benign Prostatic Hyperplasia after Transurethral Resection of Prostate in Northern Zone of Tanzania\u201d. Unknown Journal GJMR-I Volume 23 (GJMR Volume 23 Issue I1): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.