


I. INTRODUCTION
Bangladesh is a developing country in the northeastern part of South Asia. It covers 147,570 square km of landmass with a large population base of approximately 162 million (CIA World Fact Book, July 2020 estimation). The country has experienced rapid development in many areas (World Bank, 2019). Still, many development challenges are remained to resolve. The main development challenges of the country resonate around excess pressure on land and agriculture, persistent poverty and income inequality, unplanned urbanization, incompetent health structure, energy insecurity, inefficient water resource management, natural disaster, climate changes, and so on (Bangladesh Secretariat, 2012). Among these, unplanned rapid urbanization becomes one of the focal concerns for ensuring sustainable urban development.
Rapid urbanization is a reason for forming informal slum settlements that impose limit on sustainable urban development. According to statistics, around 2.23 million slum people find their residence in the city of the country (BBS, 2014). The number of slum settlements is rapidly increasing at an alarming rate to manifest around 3,399 slums in Dhaka out of a total of 13,943 slums in the country (BBS, 2014). People from different regions of the country migrate to Dhaka in searching for their livelihood (Ishtiaque & Mahmud, 2011) in response to low employment opportunities in the rural economy (Black, Kniveton & Schmidt-Verkerk, 2013). Most of the migrated people are impoverished and take shelter in disadvantaged places in the city area to form slums (Farhana, Rahman & Rahman, 2012). It causes disproportionate growth of the urban poor population that augments the slum community in Dhaka city.
The concept of a slum community depends on various spatial contexts. The definition of a slum community is conditional on a set of socio-economic, political, cultural, livelihood, and environmental factors (Banks, 2012). A group of people from a slum community is called slum people who live in an uncomfortable and neglected part of an urban city where housing and living situations are poor (Begum & Moinuddin, 2010). Slum communities in Dhaka confront multifaceted social, economic, and environmental problems. The overcrowded slum settlements render the task of urban planning and development strenuous for public utility providers and local government agencies. In this backdrop, Dushtha Shasthya Kendra (DSK), a social enterprise, develops and integrates multiple development projects under urban development programs. Ensuring social, economic, and environmental justice of the slum habitat to uplift them from the vicious cycle of poverty and improve their standard of life underlies the core of the organizational objectives of DSK.
The current case study attempts to elucidate the mechanism of blending and connecting the major urban development interventions of DSK (the primary and secondary health care project, micro-credit project, water, sanitation hygiene project, and human capital development training cells). It highlights the operationalization of a community-based organization (CBO) that occupies a pivotal position in the strategic management of urban development projects of DSK. According to DSK, the coordinated activities of people from slum communities to accomplish specific development objectives are called CBOs (DSK Publication, 2017). CBO-based management of development projects sustainably improves the standard of living of slum people in the long run by channelling solutions to correlated problems from a single institutional framework. Thus, the objective of this case study is to explore the strategic integrative approach of slum community development as a unique urban development approach adopted by DSK in Dhaka city of Bangladesh.
II. PROBLEMS OF SLUM COMMUNITY IN DHAKA CITY
Slum people in Dhaka encounter several social, economic, and environmental problems. These problems exert paramount uncertainty and vulnerability for them. So, a brief but close examination of the problem confronted by slum people is worthwhile to mention as a background for inaugurating development projects by DSK.
Low Livelihood Status and Extreme Poverty Scenario: The livelihood conditions of slum communities are poverty-stricken. Poverties (income, consumption, and asset holding) are the most frequent problems in urban slum areas (Hossain, 2007). A baseline survey by Nazem and Hossain (2012) demonstrates that 27.10 per cent of slum people fall under extreme poor, 25.43 per cent are poor, 25.04 per cent belong to moderately impoverished, and 22.43 per cent are marginally poor. Slum-dwellers spend 65 per cent of their total income on food items, whereas 96 per cent of households rarely can manage more than two meals in a day. Usually, slum people are engaged in temporary, low-paid, insecure, uncertain, and inflexible employment. A report shows that only 32 per cent of slum households involve in the formal low-skilled job, 34 per cent are unskilled labourers, and 20 per cent engage in small vendor businesses (Banks, 2012). The main occupations of slum people include micro business, low skilled workers, garment workers, rickshaw pullers, day labourers, housemaids, vegetable vendors, shopkeepers, pushcart drivers, and many more (Alamgir, Jabbar & Islam, 2009; Rokanuzzaman, Hossain & Miah, 2013). The worst poverty scenarios across slum communities become evident that slum people stay lagging behind for attaining minimum livelihood status.
Poor Quality Housing and Threats of Eviction: Economically deprived slum people find their accommodation in undignified conditions in environmentally hazardous areas such as solid waste landfills, open drains, culverts, and near to contaminating industries (Alamgir, Jabbar & Islam, 2009). Most of the housing conditions are indigent (weak and temporary structure). It is also subject to high population density (around 891 persons per acre) (Islam, Mahbub & Nazem, 2009). Slum houses are composed of local cheap and non-durable raw materials (BBS, 2014). The weakly structured house may cause substantial human suffering in response to disasters like floods, cyclones, storms, earthquakes, and many more. In the meantime, threats of eviction become a common problem for slum people that create uncertainty for them. Several examples of eviction incidence are there. For instance, at least 400,000 people have shifted their residence in Dhaka from 1971 to 2010 (Islam & waMungai, 2016). The appearance of eviction has continued to date. After evictions, it seems to be arduous for slum dwellers to emigrate and settle because most of them already have migrated to an area and have no other alternative places to be settled. Thus, evictions pose risks for slum people to lose their livelihood and render them in impoverished situations (Islam & waMungai, 2016).
Lack of Fresh Water, Sanitation and Health Services: Slum dwellers are restricted to entitle fresh water and sanitation facilities in Dhaka (Arias-Granada et al., 2018). Slum people do not possess a legal identity, residential address, or land ownership. So, they usually do not have the access to get water supply connections from public utility providers (Arias-Granada et al., 2018). Households in the slum community share their latrines and water sources with more than ten other families. Public utility authorities can only cover 37 per cent of slum people by delivering safe water (Arias-Granada et al., 2018). At the same time, 90 per cent of slum people share toilets, and 26 per cent use open spaces. Health problems are the by-product of these unhygienic environments. It leads to various seasonal, waterborne, infective, and chronic diseases such as fever, asthma, food poisoning, skin diseases, diarrhoea, hepatitis, poor mental health, and many more (Howden-Chapman, 2004). Slum people do not get proper treatment and medication when they become sick because they cannot afford to bear the higher cost of modern city hospitals and public health services provision is also constrained by limited resources.
Lack of Proper Education: Even though access to education is crucial for slum people to withhold from extreme poverty (Cameron, 2009), they have minimum access to educational services. Government schools deliver education services to only 26 per cent of slum children (Baker, 2007). Schools of various nongovernment organizations serve 27 per cent of slum people, and the remaining 47 per cent do not have any schooling experience (Baker, 2007). Demographic statistics also reveal that in the adult group (age above 15), approximately 36.2 per cent of males and 42.3 per cent of females have no schooling experience. In the children segment (age above 06 but below 15), around 14.1 per cent of boys and 8.9 per cent of girls stay far from primary school education (Razzaque, Chowdhury & Mustafa, 2019). The ambient of many primary schools for slum children is also not satisfactory in terms of delivering pure drinking water and proper school sanitation facilities.
III. CASE: THE INCEPTION OF DUSHTHA SHASTHYA KENDRA (DSK)
In 1985, a team of passionate social entrepreneurs (professionals, doctors, social activists, and volunteers) collaborated to inaugurate the journey using the name of Niramoy Free Friday Clinic. It was a clinic free of cost that dedicatedly operated on weak holidays to relieve distressed slum people from common diseases (DSK, 2018). In the beginning, the clinic was only voluntarily engaged in facilitating primary health in Dhaka. Meanwhile, in 1988, a devastating flood happened that adversely impacted on health conditions of the squatter slum in the city area. In response, DSK formulated a dedicated medical team to work formally in aiding the relief and delivering primary health care services to flood-prone slum people. In the meantime, the clinic obtained its legal status by registering with the Department of Social Service (Dha-02273) in 1989 and finally, emerged as an NGO in 1991, namely Dushtha Shasthya Kendra meaning a health centre for the impoverished with NGO Affair's Bureau (No 577) of Bangladesh (DSK Website).
a) Major Urban Development Interventions of DSK for Slum People
DSK started its journey by providing only primary health care services to extremely poor slum squatters in Dhaka. Once it achieved the initial success of the first project, it got the motivation to offer other related services for ameliorating the standard of living of slum people (DSK, 2000). Since then, DSK has been implementing several projects under the urban development program to solve various problems associated with urban public health, education and poverty. These projects range from health care projects (primary health care projects and hospital projects) to microcredit projects, environmental health projects (water supply, sanitation, and hygiene promotion), human resources training cells, and so on (DSK, 2004). DSK tailored these projects so that it could advance the social, economic, and environmental development of slum people by enabling them to be empowered and self-reliant through sustainable CBO development. In the subsequent sub-sections, a brief description is given of the major urban development interventions of DSK.
Meeting Emerging Needs of Primary Health Care Services: Slum people usually fall under the low-income group. They cannot afford high-cost health care services offered by private hospitals and clinics. The resource constraints of government health care providers are also high to fully satisfy the demand of disadvantaged people. As a result, slum people deprive of having necessary health care services. In filling this gap, DSK undertakes a primary health care project in Dhaka from its inception to build sustainable and participative health networks with the slum community (DSK, 2004). The primary health care project of DSK ensures the availability of health care services free of cost to the vulnerable slum group. However, only the member borrowers of the micro-credit project of DSK are eligible to access the primary health care services. The member borrowers, their children, husband or wife, father and mother become eligible to access the primary health care services. This project centers on three main components of clinical based activity, home visits by community health workers and training of traditional birth attendants (DSK, 2004). Community health workers frequently visit members' houses for regular medical checkups. Patients can also go to satellite clinics for medical treatments whenever required. And the traditional birth attendants are given training about hygienic practices to avoid unprecedented situations during parturition. DSK facilitates community-wide public health education campaigns for exchanging knowledge during the regular community meetings on micro-credit issues.
Replicating Micro-Credit Model in Scaling up the Effects: DSK has been operating the micro-credit model of Grameen Bank since 1992 as a poverty reduction strategy in the urban slum (DSK, 2014). This micro-credit model enables women in slum communities to empower economically by delivering inclusive financial services (Singha & Alam, 2020). DSK offers several innovative financial instruments, for example, a risk fund (akin to insurance) for livelihood security and property (livestock, crop), mobile services for receiving and issuing cash, money transfer, mobile top-up, account opening, micro-insurance, savings, remittances and so on (DSK, 2014). Women from a family with a monthly income of USD 25 to USD 30 in the range form a group to become eligible for getting micro-credit due to their backward socioeconomic position in society. Women from a group of five members of similar demographic
status and mutual trust are eligible for accessing the micro-credit. Matching and combining a few groups is a CBO where the entrepreneurial traits of member borrowers are nurtured, harnessed and utilized to develop micro-businesses (DSK Publication, 2016). DSK delivers training to member borrowers on personal financial management, credit operation and management of group savings through the CBO operation. The micro-credit project of DSK positively impacts social rank, political consciousness and relative bargaining position of women in family and society.
Ease the Access to Pure Drinking Water: Slum people do not get pure water supply from Dhaka Water Supply and Sewerage Authority (DWASA) because they do not have the endowment of land ownership in city (Matin, 1999). The DWASA and other utility providers also have a negative perception regarding the financial ability of slum communities to pay bills on time. Informal water markets also have been operated by locally influential persons to sell water at an unreasonably higher price to squatter slum people. In this situation, DSK starts playing an intermediary role between the slum community (buyer) and the DWASA (supplier) for mitigating such market void (Matin, 1999). DSK bears the liability of paying security deposits and unpaid charges to DWASA on behalf of slum people and negotiates with DWASA and Dhaka City Corporation (DCC) to build water points for slum communities. DSK ensures the supply of pure water to slum people and creates a demand for pure water to slum people through a community-wide awareness campaign. DWASA and DSK jointly constructed the first water point in October 1992 which serves more than 200 households (Matin, 1999). DSK has established more than 3200 water connections with the coordination, guidance and strategic supervision of international donors, DCC and DWASA to benefit around 800,000 slum people in Dhaka (DSK, 2018). Moreover, DSK transferred the ownership of water points to the community in 2001. Now, slum communities can directly communicate with DWASA for new water points. They also can engage in financial transactions with DWASA. Thus, DSK puts forward a transformation in the water delivery system for the slum community by building a direct networking protocol for them with DWASA and by changing their social practices.
Supporting Sanitation Facilities and Promoting Hygiene Awareness: Slum settlers usually dispose of excreta at a nearby open drain and water body. They do not afford the initial investment of constructing, maintaining and adopting safe sanitation technology options. They lack awareness
of using and maintaining hygienic practices and latrines. It causes a direct threat to the urban environment and the health of slum people. In response, DSK engages in promoting, supporting, guiding and sustaining hygienic practices among slum people (DSK, 2018). DSK segments and targets the slum community into multiple groups to conduct promotional campaigns. It disseminates information on the importance of using safe water, hand washing at six critical times, food hygiene, solid wastage management, menstrual health management, sanitation and hygienic practices to men, women, adolescent girls and children of slum communities. DSK arranges several interactive sessions such as focus group discussions, workshops and training to facilitate the awareness campaign.
DSK also has been implementing an innovative awareness project in 27 urban primary schools since 2007. Teachers of schools teach and guide students to change their attitudes toward sanitation and hygiene practices so that students can transfer good practices from schools to their communities. It relieves slum children from various diseases (diarrhoea, dysentery, worm infestation) and increases their enrollments, attendance, welfare and learning performance. Along with awareness campaigns, DSK also provides two types of financial support: grant-based and lending based to create demand for hygienic technology options among slum communities (Singha, 2019). DSK mobilizes funds under the grant scheme from different donors and foundations to purchase, install and maintain sanitation hardware for slum people. It also sanctions loans for sanitation purposes at flexible maturity, terms, conditions and interest rates.
- Delivering Secondary Health Care Services at Affordable Prices: DSK established a hospital in 1999 at Mohammadpur of Dhaka with the financial support of the Swiss Red Cross (DSK, 2013). The hospital delivers secondary and tertiary healthcare services to low-income slum people and middle-income people (DSK, 2010). Three categories of hospital services include: indoor patient services (patient admissions, labour and general surgical operation theatre), outdoor patient services, emergency services, mother and child care services, operation, and medical investigative services (diagnostic, laboratory, ultrasound, radiography), and ambulance services. Emergency services are open for 24 hours and outdoor services for 12 hours a day. The prices of these services are substantially low in contrast to the traditional private hospitals. The hospital only maintains a break-even cost to operate in the long run (DSK, 2019). The
hospital has all modern upgraded pieces of equipment and a team of highly skilled and professional technicians. The hospital team consists of a director, gynaecologists, surgeons, oncologists, nurses, specialist doctors and supporting staff.
- Development of Human Capital that can Create Difference: DSK emphasizes developing human capital as an enduring task to accomplish urban development objectives. It started a well-structured training cell in 1999 for capacity building of its staff and community members (DSK, 2004). The training module of the training cell aims to keep up the motivation and productivity of development workers and CBO members. DSK provides training to employees on microcredit project management; managerial skill development; orientation on service rules; accounting and management system; team and leadership building; office management; gender sensitivity; software; training on psychosocial counselling; and advanced training on saving and revolving loan. The grass root participants training of DSK includes management of CBO, gender, team building and leadership, disaster management, project planning, safe health behaviour development, monitoring approaches, communication skill development, financial management, reproductive health service, community-based disaster risk reduction, assessing health risk and safety and strategy for self-help group development. A pool of professional experts from DSK, government agencies, and other NGOs develop, deliver, evaluate and update the training materials. Through this training cell, DSK shares the organizational values, missions, visions, norms and culture among employees and slum community members to productively engage them to short term and long term development objectives.
IV. DISCUSSIONS
DSK, a well-known social enterprise, extends its operational horizon to provide development assistance in slum communities at three layers. At the first layer of its operation, DSK begets its journey by supplying relief and primary health care to squatter slum communities in response to a devastating flood. Then, it acquires the legal identity as a non-profit organization. Even though DSK initiates its operation by delivering primary health care services, it does not confine its development services to the health sector only. It accumulates experiences and gathers knowledge about the problems confronted by the slum community. DSK learns from the slum context that earning a subsistence level of income and access to other basic amenities are essential to get out of slum people from the vicious cycle of poverty. So, DSK brings momentum to its operational excellence by diversifying its development project portfolio at second layer. The significant development projects of DSK include but are not limited to microcredit, hospital, water, sanitation and hygiene, and human capital development project. At the final layer of DSK's operation in the urban development, it plans to sustain and scale up the positive impacts by strategically integrating these projects through CBOs.
Figure one depicts the connections among major urban development projects of DSK, whereas CBOs underlie the heart of the interlinkages. It represents a unique urban development approach undertaken by DSK to illustrate a strategic integrative perspective of slum community development. Slum people confront a set of problems that are not independent. These problems are closely connected and have multiplicative adverse effects. So, the solution landscape of DSK base on delivering blended and aligned multiple development services to slum people. The integrated development service provisions of DSK aims to ensure social, economic and environmental value for the disastrous slum people at the same time from a single organization which has been achieved by formulating and operationalizing CBOs.
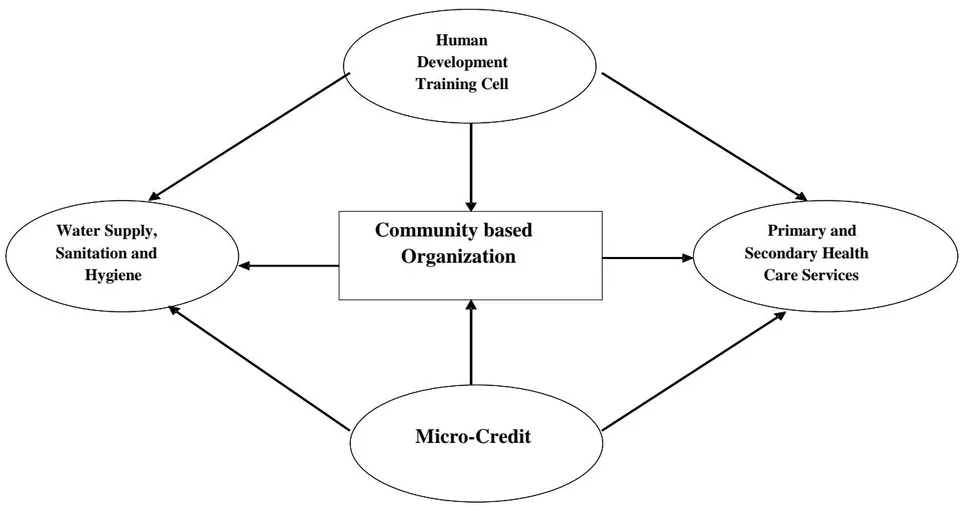
CBOs thrive on specific development purposes for slum people and ensure human participation in the development process, where the development goals are formulated and implemented by slum community members. CBOs coordinate various development activities of DSK. The microcredit borrower's groups develop CBOs with the direct help and guidance of DSK. Most of the members of CBOs are women who actively participate in the people-centric development process as co-creators in DSK's development projects. The executive committee of CBOs does have authority to accept, select and sanction loan applications. CBOs develop and maintain close networking with telecommunication services providers, financial institutions and donors for the operational sustainability of the micro-credit intervention. DSK effectively blends its primary health care project with the microcredit project (DSK, 2014). Community participation based health care services are delivered to borrowers of microcredit projects through CBOs to simultaneously impact public health and economic indicators (DSK, 1997). This community-driven mechanism reveals the growing participation rate of the borrower members of micro-credit to health care projects. In addition, DSK transfers 2.5 per cent of income earned by the microcredit project to finance primary health care projects. DSK hospital also allocates 5 per cent of gross income as a 'health equity fund' for the poor CBO members who can get secondary health services free of cost. Members of microcredit projects can also apply for loans for building the water points, and buying, installing and maintaining hygienic-sanitary technology (Singha, 2019). DSK adopts the model of self-governed CBOs to manage the water points in terms of cost of capital, operation and maintenance (Martin, 1999). A representative water committee is also formed for each CBO, headed by women, to support the community in solving local problems through proper planning, designing, selecting the location, and formulating water use rules. DSK transferred the ownership of water points to the community in 2001 for the first time. Since then, CBOs can construct and manage water connections and pay the bill to DWASA on behalf of slum people. CBOs also hold responsibility for the operation, maintenance and cleanliness of the sanitary hardware. In interconnecting these development projects, the human capital development cell of DSK plays a vital role. It enhances the capability of its employees and team leaders of CBOs. The training cell of DSK provides dedicated training to the staff on microcredit, water supply, sanitation and hygiene, and primary and secondary health projects. It also gives necessary training to CBO members, who directly influence the members of the slum community.
By formulating CBOs to connect different development services for delivering integrated social, economic and environmental value, DSK contributes to transforming the social practices of slum communities.
DSK sorts a path for members of CBOs to be empowered to communicate and interact with various stakeholders such as slum people in a slum community, government organizations, local and international civil society, local governments, legal and political institutions, and donor agencies. CBOs thus act as a vehicle of strategic management of empowerment and leadership skill development for the slum community to uptake the responsibility of advancing their status quo of their own. They identify and execute community development planning which is specific, measurable, achievable and realistic with the guidance, supervision, resource supply and training of DSK. CBO development strengthens the capacity of the slum community for local development goals. Slum people can analyze the problems they confront, plan and monitor the development activities for solving the problems, find and mobilize a pool of resources, allocate the budget, proceed with the necessary paperwork, and execute periodically (weekly, monthly, yearly) meetings. CBOs also generate project funds by collecting funds from members and engaging in some revenue-generating activities. That's how DSK chooses the sustainability of its operational capacity as a means of the creation of self-sustained CBOs. These self-governed CBOs learn to manage community resources and development aid from the government, donors, foundations and civil societies to enhance the operational capacity of delivering development services.
V. CONCLUSION
The strategic integrative approach to urban slum development of DSK under social entrepreneurship for slum people already has proved successful. DSK provides the means, motivations, legislative and resource support to form CBOs. It also helps transform self-reliant and self-governed CBOs for sustainable urban development in the long run. CBOs work as a social platform or a representative agent to negotiate and bargain for the social welfare of the squatter slum people. The urban development interventions of DSK, which are channelled and connected through the operation of CBOs, bring about system-level change to get out slum people from a vicious cycle of poverty. For example, the unique and realistic sustainable water supply model of DSK leads to social changes in the power relationship among multiple stakeholders (slum dwellers, the landlords, the water utility and the city authority) (Matin, 1999). It reshapes the dynamics of the power structure in the society to guide toward sustainable cities. This intervention is widely diffused and replicated by various domestic and international development institutions and the Government of Bangladesh in both rural and urban settings (Akash & Singha, 2011). Meanwhile, the awareness campaign regarding hygiene and sanitation practices among students is another innovative way of bringing change from the grassroots. This project of DSK focuses on developing a learning chain from teacher to child, child to child, child to parents and parents to community for effectively disseminating the message of sanitation and hygienic practices. When government health care services are constrained, and the private provision remains unreachable considering higher prices, DSK hospital becomes a hope for accessing secondary and tertiary health care services for urban slum people. DSK also has scaled up its operational excellence of micro-credit to empower economically marginalized people in geographically dispersed areas of Bangladesh. DSK also emphasizes developing human capital for sustainability. It provides well-designed training on different development issues to its employees, members of CBOs and other development partners. In this way, DSK scaled up its operational excellence to eradicate extreme poverty and improve the health status of any disadvantaged group in Bangladesh. DSK has successfully diffused and operated this unique development perspective in three other mega-urban cities in Bangladesh. It also has expanded its operational horizon to the rural, coastal and wetland regions domestically and in the foreign countries like Rwanda, Afghanistan and Zambia. Experiences accumulated from one project and context assist the social enterprise (DSK) in understanding the problems and solutions of new projects and integration of those projects. DSK designs and integrates some necessary services delivered by multiple projects that promote social, economic and environmental value to poor people in getting them out of a vicious cycle of poverty.



