A retrospective study based on the review of medical records in the Tasy system of patients admitted with diabetic ketoacidosis in the emergency service at Children’s Hospital Dr. Jeser Amarante Faria, Joinville-SC. 88 medical records were analyzed, corresponding to 71 patients, nine patients with more than one hospitalization, a majority of females (78%), age range from 1.3 to 17.1 years. A mean of five days of hospitalization, with 21 cases requiring hospitalization in the intensive care unit was noted, along with severe diabetic ketoacidosis in 59 consultations. Patients who never had a diabetic decompensation were 44% of the consultations. Hypoglycemia was the most common complication (24%), and no deaths were recorded during the evaluated period. Girls with a mean age of 10 years were the main group admitted with diabetic ketoacidosis, and this medical emergency is still often the first manifestation of type 1 diabetes mellitus in our midst.
## I. INTRODUCTION
Diabetes Mellitus (DM) is a metabolic syndrome characterized by the presence of hyperglycemia, and has many possible etiologies. In pediatrics, type 1 diabetes (T1D) is the most prevalent strain of DM, and it is one of the most common childhood chronic diseases. $^{1}$
T1D has an autoimmune etiology, with increasing destruction of pancreatic beta cells, the insulin producers, which leads to their total eradication, and complete exogenous insulin dependency.2 $90\%$ of cases diagnosed in pediatrics are T1D3, and approximately 96.100 children under 15 years old develop T1D every year, with an estimate of 586.000 children and teenagers being disease carriers all around the world. Brazil holds the third position of most cases of T1D in persons under 20 years.4
Typical T1D symptoms are polyuria, polydipsia, polyphagia and weight loss. When all symptoms are present, a clinical diagnosis is not hard to accomplish.
However, with a late diagnosis, the patient can develop Diabetic Ketoacidosis (DK), which has high morbidity and mortality. National data shows a prevalence of $42.3\%$ of T1D patients who were first diagnosed during an episode of DK, but the data have great regional variation.[5]
The DK is a group of many clinical and laboratorial changes caused by insufficient insulin activity and increased counter-regulatory hormone production that begins as an answer to stress situations which alter carbohydrate, fat, and protein metabolism. Glycogenolysis and gluconeogenesis occur to increase glucose production, proteolysis and lipolysis occur to provide substrates to the gluconeogenesis, which results in a ketone bodies production secondary to lipolysis. A cellular catabolism state surges after these metabolic alterations. Osmotic diuresis is a result of sugar in the urine and ketonuria, and leads to metabolic depletion of sodium, potassium and phosphorus, among other minerals. $^{1,2,4}$ Vomiting, a result of ketonemia, added to osmotic diuresis causes severe dehydration, and the hypoperfusion state in tissues all over the body aggravates the acidosis by producing lactic acid and reducing the glomerular filtration rate. Increased glucose, ketones and urea levels lead to a hyperosmolar state that induces idiogenic osmoles production by the central nervous system cells. $^{2}$
The main clinical findings in a patient during a DK state are: dehydration, ketonic breath, abdominal pain, vomiting, tachycardia, Kussmaul breathing, low blood perfusion signs, and central nervous system changes may be present. Laboratory findings include hyperglycemia $(>200\mathrm{mg / dL})$, metabolic acidosis $(\mathsf{pH} < 7,3$ or $\mathrm{HCO_3} < 15\mathrm{mEq / L})$, ketonemia and ketonuria, and anion gap elevation.
DK can be divided according to the level of acidosis. Mild DK when pH is 7,3-7,2 or $\mathrm{HCO_3}$ is between 10-15 mEq/L; moderate DK if 7,2-7,1 or $\mathrm{HCO_3}$ is between 5-10mEq/L and severe DK when pH\<7,1 or $\mathrm{HCO_3} < 5$ mEq/L. Complications such as cerebral edema, acidosis and other major hydroelectrolytic disorders secondary to DK are the main cause of death in children and teenagers with DM.
Treatment consists in progressive correction of the hydroelectrolytic disorders: a slow and steady reduction of sugar levels in blood along with ketogenesis can be managed with insulin doses administered after the initial expansion phase.
This study aims to demonstrate the characteristics of the patients who were admitted at the emergency room while in DK, how they were managed and the cases outcomes.
## II. METHODS
Retrospective study with data obtained by reviewing the emergency room archives at the Children's Hospital Dr. Jeser Amarante Faria, Joinville-SC. There were included patients admitted at the Emergency room in the period between january 2013 and December 2017 who were clinically diagnosed with DK and had the following laboratory findings: hyperglycemia $(>200\mathrm{mg / dL})$, metabolic acidosis $(pH < 7,3$ or $\mathrm{HCO}_3 < 15\mathrm{mEq / L})$, ketonemia or ketonuria. The International Classification of Diseases used to filter out the charts found in the medical records on the PHILIPS
Tasy system (Philips Healthcare, Cambridge, MA, USA) were E10.1, E13.1, E14.1 and E10.0. Incomplete or lost charts were excluded from the study. Starting from the data bank built as a Microsoft Excel 2013 sheet, the data was analyzed and presented as statistics. This research was approved by the Hospital Hans Dieter Schmidt/SES/SC ethics and research committee, under the authorization number 3.098.043.
## III. RESULTS
There were 97 hospitalizations of 88 patients with DK. Nine patients were hospitalized more than once (one patient arrived seven times at the hospital, another one five times, another one was four times, and six patients were hospitalized two times each, in a time span of five years), totalling 28 admissions. Of these 88 patients, $68\%$ were girls (60). Age range varied from 1.3 to 17.1 years, and 10.7 years were the average age (Table 1).
DK as a T1D first manifestation corresponded to 48 medical attendances, $49\%$ of the total $(p$ -value $= 0.920)$ (Figure 1).
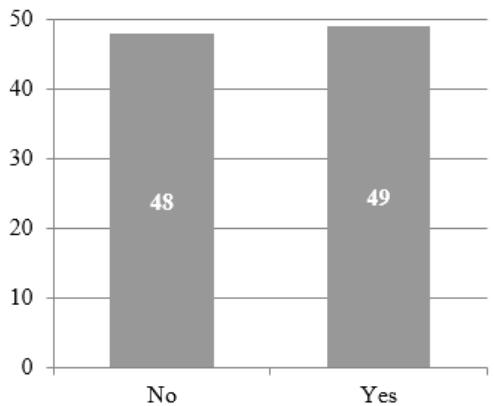 Figure 1: DK as a T1D first manifestation
Severe cases corresponded to $65.9\%$ of the medical attendances, $20.6\%$ were moderate, and $13.4\%$ were the mild cases, considering $\mathsf{pH}$ and $\mathrm{HCO}_3$ levels of the arterial gasometry that was first collected.
Among the 97 hospitalizations, 27 were admitted in the Intensive Care Unit (ICU). The patients were, on average, five days in the ICU, but two of them stayed for more than 20 days (one patient during his leukemia treatment and another presented cerebral edema as a complication).
In 28 cases there were complications, hypoglycemia being the most common in $19.5\%$, hypocalcemia in $9.2\%$, hypercalcemia in two and hypernatremia in one occasion. Cerebral edema was the most serious complication, happening in one patient but with no deaths.
## IV. DISCUSSION
T1D incidence all over the world increased in the last decades, especially among children under 5 years old. An estimate of 30 thousand Brazilians are T1D carriers, and Brazil occupies the third position of countries where T1D has the most prevalence.[4]
It is imperative to recognise the profile of the patients who present DK at the emergency room, as this is the main cause of death among diabetic children and teenagers $^2$.
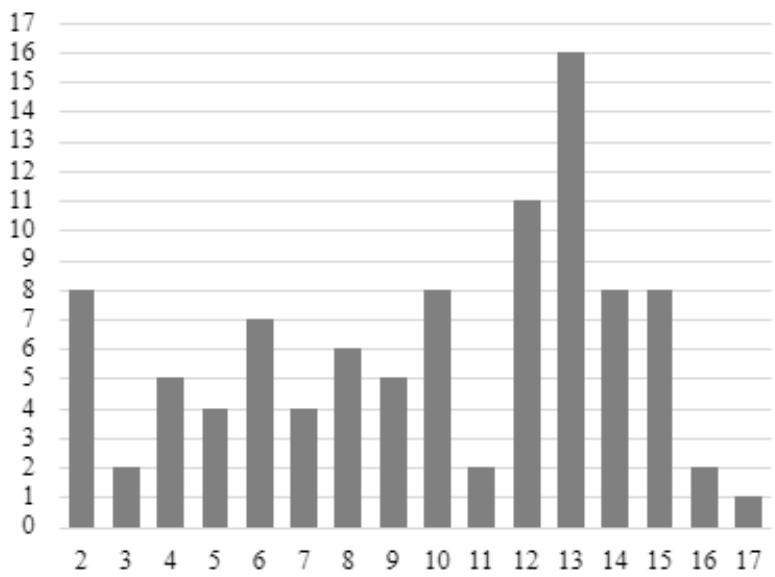 Figure 2: Distribution graphic of number of hospitalization x age in years
By observing the age distribution graphic (Figure 2), it is clear that the teen years are the period in which it is most difficult to accomplish a good metabolic control, therefore the highest incidence of DK complications happen during this period.6 In this study, $49.4\%$ $(p$ -value $= 0.920)$ of the hospitalizations corresponded to first decompensation situations. In a large national study, the Brazilian T1D Study Group (BrazDiab1SG)[^4], 3591 patients with T1D (56% feminine sex) were evaluated at public institutions, and it was found that $42.3\%$ of patients with T1D were diagnosed with the condition during a DK episode, a similar result was obtained in our study, like in other literatures. The glycemic decompensation is usually longer and more severe in newly diagnosed patients with T1D.[^6]
Insulin was first used in the 1950s, when the mortality rate was up to $10\%$. Today, there are specialized centers with focus on the treatment of DK, where the mortality rate in general is below $1\%$. Fortunately, no deaths were recorded at the analyzed period. Cerebral edema, considered the most feared complication, occurred only once, with a positive outcome.
The analysis of the patients characteristics in this study showed that DK was most frequent in girls at 10 years of age. It still is very common that the first manifestation of T1D is the sudden and serious DK. Although a medical emergency, the appropriate management increases the chances of a positive outcome.
Generating HTML Viewer...
References
11 Cites in Article
Maria Dos Santos,Claudia Gallafrio (2008). CARDIO-ONCOLOGIA NA POPULAÇÃO PEDIÁTRICA.
J Piva,M Soledade,M Czepieiewiski,Cetoacidose Diabetica (2015). Medicina Intensiva em Pediatria.
D Care,S Suppl (2019). 13. Children and Adolescents: <i>Standards of Medical Care in Diabetes—2019</i>.
J Oliveira,De,R Montenegro Júnior,S Vencio (2017). Diretrizes brasileiras de manejo de toxicidades imunomediadas associadas ao uso de bloqueadores de correceptores imunes.
M Czepieiewiski,P Garcia,J Piva,D Machado (2009). Cetoacidose Diabetica.
Lelma Castro,André Morcillo,Gil Guerra-Júnior (2008). Cetoacidose diabética em crianças: perfil de tratamento em hospital universitário.
(2017). Obstructive sleep apnea and primary snoring: treatment.
N Cho,J Kirigia,J Mbanya,K Ogurstova,L Guariguata,W Rathmann,A Reja (2017). International Diabetes Federation. Diabetes Atlas.
J Piva,M Czepielewski,P Garcia,D Machado (2007). Current perspectives for treating children with diabetic ketoacidosis.
C Alves,A De,K Cargnin,L Paula,De,L Garcia,P Collett-Solberg,R Liberatore,T Della-Manna (2018). Diabetes Mellitus Tipo 1 e Autocuidado.
C Alves,A De,K Cargnin,R Arrais,P Collett-Solberg,L Garcia,R Liberatore,C Andrade,N Do (2018). Diabetes Mellitus Tipo 1 e qualidade de vida relacionada à saúde.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Lucas Horochoski. 2026. \u201cStudy of Patients with Diabetic Ketoacidosis Admitted at the Pediatric Emergency Service at Childrens Hospital Dr. Jeser Amarante Faria\u201d. Global Journal of Medical Research - F: Diseases GJMR-F Volume 23 (GJMR Volume 23 Issue F3): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
A retrospective study based on the review of medical records in the Tasy system of patients admitted with diabetic ketoacidosis in the emergency service at Children’s Hospital Dr. Jeser Amarante Faria, Joinville-SC. 88 medical records were analyzed, corresponding to 71 patients, nine patients with more than one hospitalization, a majority of females (78%), age range from 1.3 to 17.1 years. A mean of five days of hospitalization, with 21 cases requiring hospitalization in the intensive care unit was noted, along with severe diabetic ketoacidosis in 59 consultations. Patients who never had a diabetic decompensation were 44% of the consultations. Hypoglycemia was the most common complication (24%), and no deaths were recorded during the evaluated period. Girls with a mean age of 10 years were the main group admitted with diabetic ketoacidosis, and this medical emergency is still often the first manifestation of type 1 diabetes mellitus in our midst.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































