## I. INTRODUCTION
Technologies that have already and will continue to have a strong impact on the transformation of healthcare are closely related to capture, data exchange, artificial intelligence, smart control, visualization with simulation, 3D printing and robotics, which are made possible by technologies in the field of automatic data processing and broadband communication technologies. All of the above, including the Internet, ambient devices and intelligent computer systems, are causing an increasing use of these technologies in medical practice. Thus, technologies from the field of Automation and ICT technology, through the increasingly widespread use of supported health services, also affect social relations.
In addition to ICT technologies, which already have and may have had a great impact on the transformation of healthcare, technologies such as: remote monitoring of vital parameters (Telehealth), artificial intelligence, 3D printing technologies (organs, parts of the skeleton), augmented and virtual reality, wearable non-invasive sensors, digitization, robotic surgical systems and the development of bioinformatics smart structures.
We predict that the increasing aging of the population, the rise of chronic diseases, natural and other disasters, and the increased demand for real-time monitoring and patient care systems will accelerate the use of artificial intelligence in almost all areas of healthcare. In order to achieve the mentioned goals, it is necessary to increase the knowledge of the medical staff in the areas of application of the mentioned technologies. In addition to these, it will be necessary to look for support in making quality diagnoses, support in image analysis, 3D printing, simulation of surgical interventions, design of custom devices and tools, improvement of the accuracy of medication action, augmented and virtual reality, simulation of treatment procedures, augmented and virtual reality, wearable body sensors, improved patient participation, as well as the next generations of technology-supported healthcare.
## II. IMPORTANT KNOWLEDGE OF MEDICAL STAFF
If we want to develop superior health care and expand it into widespread use in all branches of medicine, we must also properly educate doctors and support staff so that they can successfully use all the latest achievements in the treatment and rescue of patients. Since these skills are complex, and since the methods that support the aforementioned procedures are based on real data, it is important that only these are systematically managed throughout the healthcare system, while at the same time they are accessible to artificial intelligence methods, which increasingly support too many areas of healthcare. As the doctor becomes burdened with new challenges, let's give just a few basic technological areas important for successful treatment.
### a) Unified Database
One of the biggest challenges in healthcare today is the lack of data sharing between healthcare providers. Almost no patient information is shared between providers, causing delays and potentially harmful patient treatment that could be avoided by implementing a single shared database. The secure exchange of patient data and information between healthcare providers is one of the most important advances of our time. Withholding patient data and information leads to unnecessary healthcare costs. This greatly affects the duplication and thus the redundant bio-medical analyzes and examinations that are carried out. Such closing of patient data and information can also lead to inadequate treatment, which can also be dangerous. Shared databases can help bridge the gap by giving healthcare professionals direct and easy access to critical patient data and information. Thus, the safe exchange of data and information about patients between health service providers and the support of the analysis of this data using artificial intelligence will represent one of the most important advances in medicine in the coming decade.
### b) Artificial Intelligence
Artificial intelligence (AI) is one of the most powerful tools in today's modern knowledge-based medicine systems. The power of artificial intelligence lies in its fast and detailed analysis of large amounts of data. Artificial intelligence enables real-time monitoring of all vital functions and thus high-quality, professional and affordable health care. By analyzing the data, it also helps healthcare workers to diagnose disease states, as well as to make the best decisions in the treatment of patients. Artificial intelligence is also helpful in managing and performing tedious and time-consuming administrative tasks. Using learning methods, we can develop models from known data that help predict the outcome of a certain patient treatment procedure. These are supervised learning methods, while unsupervised learning methods mainly look for patterns or similarities between data.
### c) Predictive Data Analysis
Artificial intelligence (AI) and machine learning (ML) are already being used for predictive analytics in healthcare. AI and ML can help predict possible patient conditions by analyzing patient data on the fly, on the basis of which we can save their lives. By analyzing vital data, the system can monitor the patient's response to certain drugs or treatment protocols. Based on the remote monitoring of this data, the system will analyze which patients are likely to be readmitted to the hospital and for which reasons.
Real-time predictive analytics of patient and family data also enables preventive treatment of patients, because a timely medical history can mean how to avoid a patient's admission to the hospital.
### d) AI Assistance in Medical Image Analysis
Artificial intelligence already has a strong influence on the transformation of healthcare. We can ask ourselves, how do doctors understand what is practically happening in the dynamic space of artificial intelligence? Pattern recognition algorithms supported by artificial intelligence transform a winter landscape image into a spring blooming scene.
Today, we've reached a point where pattern recognition algorithms and artificial intelligence (AI) are more accurate than radiologists at spotting breast cancer images and other medical features that involve correlations between normal and abnormal patterns.
Artificial intelligence can therefore identify changes in imaging patterns faster than a top radiologist, which can help diagnose, track, progress and respond to disease treatment. The approach to the analysis of patients' imaging material using artificial intelligence represents a great support and potential for clinical decisions in time-critical situations or when there is a lack of available expertise. This aid represents an important support for medical staff in cases of remote or poorly funded medical institutions. AI is not only used in the evaluation of conventional radiological examinations, but also in cases of computed tomography (CT) and magnetic resonance imaging (MRI).
We use artificial intelligence where it enables better and more successful treatment, thereby increasing the quality of treatment and thus the credibility of the hospital.
Artificial intelligence is generally divided into 10 functional areas /19/:
1. Deduction, reasoning and problem solving.
2. Knowledge representation: useful information about the real-world objects of the problem.
#### 3. Machine learning.
4. Robotics, which means movement and manipulation and the recognition of efficient paths.
5. Planning: the system's ability to set goals and achieve them.
6. The process of communication in natural language.
7. Perception and computer vision.
8. Social intelligence for recognition, interpretation and simulation of human movements.
9. Creativity, which means a combination of theoretical and practical solution design.
10. General intelligence, which means autonomous thinking, and machine learning intelligence.
### e) AI and Diagnosis
Reading and real-time analysis of a huge amount of data is a big problem for doctors, as the results of data analysis are important for making a diagnosis. Artificial intelligence, like a top specialist, "examines" the patient's electronic medical record together with all imaging elements, captured vital parameters and laboratory results faster and more efficiently by connecting all this data to the existing database, and compares it with examples of patients from around the world. Based on feature analysis and comparison, the AI algorithm makes a diagnosis proposal. The system supported by AI methods only helps the doctor in making a diagnosis, the final decision is always in the domain of the diagnostician.
In the field of AI in medicine, there are a number of interesting companies that are already and are ready to participate in the development of models that promote quality and two levels of treatment. These are:
Imagia: artificial clinical intelligence for early detection of cancerous changes.
Butterfly: for successful medical imaging accessible to everyone in the world.
Mindshare: medicine with image-driven intelligence.
Bay Labs: deep learning on critical unsolved problems in healthcare.
Zebra: Algorithms help radiologists discover often-overlooked indications.
Behold.Ai: an artificially intelligent medical imaging platform.
A Tomwise: Developer of AtomNet's deep learning technology for small molecule detection.
Pathway Genomics: combining artificial intelligence and deep learning in precision medicine.
Advenio: Provides machine learning-based artificial intelligence, deep learning, and computer aided discovery (CADx) for diagnostic clinical imaging.
Enlitic: Uses deep learning to extract actionable insights from a multitude of clinical cases.
Lunit: development of advanced software for analysis and interpretation of medical data.
Sig Tuple: building intelligent screening solutions to aid diagnosis.
Insilico Medicine: Artificial Intelligence for Drug Discovery, Biomarker Development.
Medymatch: a method to prevent chronic diseases and improve patient treatment.
Intuitive: Da Vinci robotic systems for surgical care.
The assessment of the potential of artificial intelligence in medicine begins with understanding the framework of the operation of AI using the solutions offered by the mentioned foreign as well as domestic research and development-oriented companies /20/.
### f) 3D Scanning in the Medical Field
When capturing information about internal organs, we see the use of a set of different scanning methods such as X-rays, CT, MRI and ultrasound. Unfortunately, there is a methodological gap in obtaining data on external body parts. With the advent of 3D scanners that allow accurate measurement of the size, shape, texture, color and surface of human skin, a new area of clinical application is emerging, ie high-resolution 3D scanning. It is useful to support these methods with the results of X-ray measurements, computed tomography, magnetic resonance and ultrasound.
Today, 3D scanning tools have already been developed for commercial medical applications, where together with analysis data, simulations and the final model, we arrive at the rapid production of effective customized medical implants. With a 3D scanner, a set of captured images is combined into a virtual 3D model, where we also use the technologies of stereo vision, photogrammetry and peripheral projections.
3D objects can be easily produced with a printer that follows the data from a 3D scanner. 3D scanning service as well as 3D printing are crucial for many fields of medicine. The emphasis in the development of the model is on the time, accuracy of the implant reconstruction, as well as its improvement.
### g) 3D Printing
Creating anatomical models using 3D printing enables the creation of physical models of anatomically accurate patient structures that can be used for surgical planning and education for both patients and trainees. This is extremely beneficial for complex surgical procedures where any error could be harmful, as can be the case in neurosurgery. This revolutionary technology will improve patient care by better training medical staff and increasing the effects of personalized health solutions. To generate an appropriate medical image model, appropriate supporting software such as 3D Slicer 3DIM Viewer is required. The information generated by the 3D scanner helps surgeons and radiologists to control and select the correct MRI or CT segmentation. Segmentation and visualization data are converted into a uniform STL format that can be used in other applications.
By 2025, 3D printing in the medical field is expected to be worth around 3.2 billion euros with an expected annual growth rate of $17.7\%$.
### h) Custom Design of Devices and Tools
Medical devices, prosthetics, dental implants and even surgical tools can now be customized to the patient or user. Sterile surgical instruments such as forceps or scalpel handles can be manufactured at significantly lower costs. 3D printed prosthetic limbs or implants that are specially adapted to the user have the same functionality as traditionally made prosthetic elements, but they can be made faster and cheaper.
### i) Augmented and Virtual Reality
Augmented and virtual reality (AR and VR) caused first a real confusion, and then a real revolution in medicine. The first VR applications started in the early 1990s due to the need of medical personnel to visualize complex medical data, especially during surgery or for surgery planning. VR can also be described in terms of human experience as "a real or simulated environment in which the observer experiences telepresence", where telepresence can be described as a sense of presence (Riva, 2003) in the environment through communications." Augmented reality is popular in various fields. medicine. Its use in medicine is a more and more promising technique for operations that require great precision. The use of augmented and virtual reality in the medical field shows promising results. With the help of augmented and virtual reality, doctors will be trained, and at the same time, these technologies can represent a therapeutic tool for treating patients.
### j) Simulation of Medical Procedures
Augmented and virtual reality (AR and VR) allow the realization of detailed simulations of medical procedures, allowing doctors to walk through one, two or a hundred procedures before starting to work directly with a patient. Simulation technology has become so good that doctors and medical students can practice with superior accuracy on the problem itself, while experiencing simulations and procedures with near-total immersion in the problem. This gives the ability to make decisions and review results without putting the patient at risk while experimenting and learning.
### k) Wearable Body Sensors
As the diversity of wearable technology systems and applications increases, they are expected to become an indispensable part of our lives, much like smartphones were in the past. With today's long-lasting small batteries, with data exchange via a WiFi communication channel and with the support of real-time data acquisition of vital functions, wearable non-invasive sensors will quickly become an integral part of monitoring and caring for the user's health.
### i) Timely Diagnosis and Clinical Support
Wearable body smart vital signs sensors have rapidly expanded to allow real-time collection of clinically relevant medical data. Combined with well-designed mobile apps, users can view the analysis of their collected data and also share it with their healthcare professionals. Users can also receive alerts in case of detected irregular courses of vital parameters such as heart rate, breathing rate, etc., which may indicate a serious patient condition. The mentioned technology of real-time capture of vital parameters can, by using other patient data and AI methods, enable the timely diagnosis of a dangerous health condition of patients, even before it worsens and/or becomes life-threatening.
### j) The Next Generation of Technologically Supported Healthcare System
The next technology-supported generations of the healthcare system (NGS) will have a strong impact on changes in healthcare. The next generations are expected to play a central role in the development of personalized medicine, to enable, with their potential, great added value in clinical and research projects, both at the level of the individual and the nation. The main advantages of new technologies are the enormous increase in the quality of diagnosis, the reduction of healthcare costs, the improvement of the quality of life of patients and the advancement of medical science and innovation.
### k) Smart Healthcare Communication Networks in the Hospital of the Future and Data Structures
The concept of the Hospital of the Future (HoF) will mainly enable the wireless connection of patients, healthcare workers, sensors, computers and medical devices.
To meet the stringent requirements of future healthcare scenarios, such as improved performance, security, privacy and spectrum utilization, we propose a flexible hybrid optical-radio wireless network that provides efficient, high-performance wireless connectivity for the hospital of the future. The concept of the connected hospital of the future takes advantage of flexible hybrid optical-radio networks. Such networks can be dynamically reconfigured to meet the needs of communication over optical or radio communication channels, depending on the requirements of the current service. We envisage that the communication network of the hospital of the future will consist of many communication devices and hybrid optical-radio access points for data transmission. Communication systems based on the use of visible light exploit the idea of visible light communication (VLC), where white light-emitting diodes (LEDs) provide both room illumination and optical wireless communications (OWC). A hybrid radio-optical communication system can in principle be used in any future hospital scenario.
In addition to hybrid access, we also envisage the use of a reconfigurable optical - radio communication wireless network (WBAN), which enables the expansion of a conventional WBAN network to a more general, application-adaptive network. As the radio spectrum becomes more and more congested, the hybrid wireless network approach is an attractive solution for more efficient use of the spectrum. The HoF concept aims to improve healthcare while using hospital resources efficiently.
This type of solution, which combines optical and radio transmission networks, would increase spectral efficiency, privacy and at the same time reduce the exposure of patients to radio signals (RF).
The huge increase in new communication technologies such as 4G and 5G, the increase in the use of wearable Internet of Things (IoT) sensors and the increase in wireless medical communication devices could lead to spectrum congestion, security and privacy issues for users of radio networks.
Therefore, in the case of smart hospitals and smart healthcare, we need to use the aforementioned technologies in transforming conventional care into patient-centered care. The aforementioned adaptive networks, together with the 5G and 6G technologies announced today, represent an impetus for a rapid revolution in the healthcare vertical. Currently, 4G and other communication standards are used in healthcare for smart health services and applications. The aforementioned technologies are crucial for the development of future smart healthcare services.
With the growth of the healthcare industry, more and more applications are expected to generate huge amounts of data in various shapes and sizes. Such large and diverse data require special consideration in terms of time-consuming point-to-point connections, bandwidth, time-consuming processing, etc. Current communication technologies have a hard time meeting the demands of the highly dynamic and time-sensitive healthcare applications of the future.
Therefore, today's 5G networks are being developed to address the diverse communication needs of Internet of Things (IoT) healthcare services. Today's smart healthcare networks, with the help of the 5G standard, represent the convergence of IoT devices that require improved network performance and cellular coverage. Current IoT connectivity solutions face challenges such as supporting a huge number of devices, standardization, energy efficiency, device density and security.
6G. This next generation of wireless technology is expected to deliver even higher speeds, lower latency and higher bandwidth for the instantaneous delivery of massive amounts of data in decentralized, intelligent networks.
6G is now in the research phase and while it is still a little early to name the killer applications, some predict that it will become an integral part of our society. One focus for 6G is a further step towards "always-on" and "lag-free" communications, including very high data rates. This will significantly increase productivity and drive new opportunities in automation, artificial intelligence (AI) and the Internet of Things (IoT).
ICT technologies have changed the way medicine is practiced and taught. Therefore, we must also delve deeper into the study of the challenges facing medical education in the age of ICT. They are:
- Preparing for the changing behavior of Internet-savvy patients.
- Raising awareness of the benefits of using ICT
- Motivating medical students and doctors to use ICT for information seeking, learning and development
## III. ARTIFICIAL INTELLIGENCE AND ROBOTICS IN SURGERY
### a) Surgery and Robotics
Artificial intelligence is now seen as an aid to surgery rather than a replacement for an actual surgeon. The use of artificial intelligence in surgery, together with surgical robotics, patient scanning and 3D visualizations, is already causing significant changes in surgical procedures on both sides, both the surgeon and the patient.
The use of artificial intelligence in the learning and training of surgeons is very important. This training is undergoing significant changes, as simulation methods with the support of artificial intelligence create the possibility of learning from virtual surgical procedures. Both surgeons and trainees can practice skills in a controlled environment, developing new surgical methods and increasing their understanding of more complex procedures. The use of artificial intelligence and simulation processes in the training of surgeons improves the quality and efficiency of work. With this approach, young specialists in the field of surgery can increase the quality of their knowledge, as they acquire a certain level of competence for further work.
Robot-assisted surgery is one of the most important technological achievements in the field of surgery in the last two decades [1]. With the introduction of laparoscopic - minimally invasive surgery (MIK), this procedure allows surgeons direct access to internal organs, which creates the need to improve ergonomics and creates the need for intelligent support of the robotic manipulator. MIK is accessed through small openings, using specialized instruments and cameras (laparoscope) to observe the operation site. Robotic-assisted MIS (RMIS) uses the same principles, where the instruments are the same, except that they are driven by motors and control systems that provide greater instrument dexterity and precision, as well as effective visualization at the surgical terminal. Such a surgical system is da Vinci (Intuitive Surgical Inc., USA), which is widespread throughout the world and also here in Slovenia.
The development of management methods and artificial intelligence methods have greatly influenced the efficiency of robot-assisted surgery. In this, artificial intelligence methods have proven to be widely applicable, such as in the training of surgeons, in the simulation of surgical interventions, in intraoperative decision-making, in predicting events, as in preoperative planning of major operations, management of complications and re-certification of surgeons /2/.
A surgical robot is therefore an autonomous, computer-controlled device that can be programmed in such a way as to represent an important aid to the surgeon in positioning and working with instruments, as well as in solving increasingly complex problems. [1] The systems currently in use are not intended to operate independently of the surgeon. These systems act as extensions of the arms, fully controlled by the surgeon, and are best described as manipulators. The surgeon's main console represents the user interface of the robot, which provides the surgeon with functions such as a three-dimensional view with the help of an endoscopic camera, control of the manipulators used by the surgeon during the surgical procedure, as well as scaling, which means converting the surgeon's natural movements into filtered micro-movements, which increases the accuracy of the manipulator's hand movements.
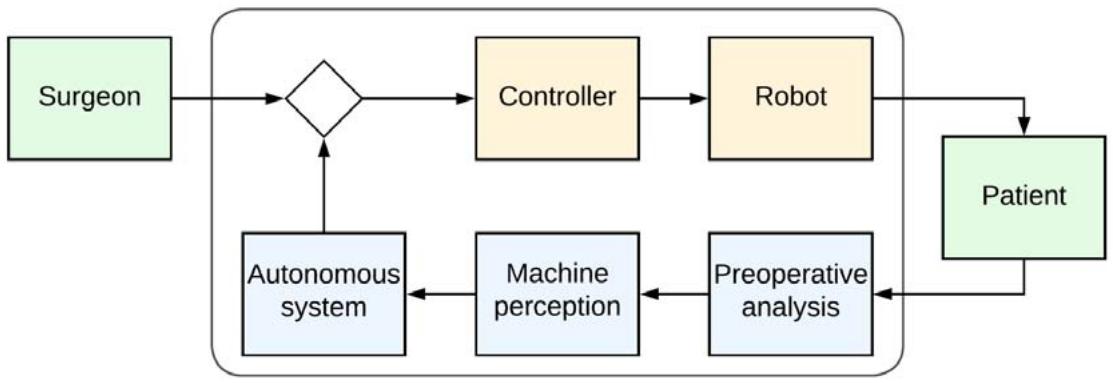
Development and research in the field of surgical robots require intensive cooperation of several research areas. The structuring of these research efforts was published in the article/ Autonomy+in+Surgical +Robotics/ from 2017. Autonomy of surgical robots is defined by the International Organization for Standardization (ISO 8373:2012) as "the ability to perform a planned task based on current state and perception without human intervention." However, "autonomy" is not a single state, but a set in which the degree of human intervention is inversely dependent on the degree of robotic autonomy - independence. Examples of robotic surgical devices with variable autonomy are robots from Intuitive Surgical, Sunnyvale, CA, USA.
The degree of autonomy of surgical robots is divided into six levels in the mentioned article, namely:
- Without autonomy,
- Help the robot
- Task autonomy,
- Conditional autonomy,
- High autonomy and
- Complete autonomy.
This classification is inspired by the definition of the level of "automated driving" in the automotive field. Incorporating autonomy into the work of a surgical robot raises many questions regarding the ethical, medical, legal and social aspects of autonomy. These problems are being discussed around the world, especially from the point of view of ethics and safety, as we can expect that researchers will offer solutions that will allow autonomous robots to offer greater patient safety, higher quality of treatment and at the same time reduce the burden on medical staff. Here, a positive social perception of surgical robots is important from the point of view that hospitals do not become factories and patients become facilities on a conveyor belt.
It is also important to distinguish between automatic and autonomous operation /Autonomy and Surgical Robotic/. Automatic operation is completely predictable, following either deterministic or probabilistic processes. At a basic level, the robot actually performs movements on the patient's side, which are controlled by the surgeon via a control interface. Here we do not encounter machine decision-making, but all decision-making is left to the surgeon. If the variations of the external parameters are too large, the system may also fail in such a case. In such a case, the autonomous system is able to adapt to changed external conditions, since its adaptation requires deep knowledge and the use of cognitive tools, which do not exist in the classic automatic control of a robot system.
### b) Adaptive Control of Robots
Robot control is the process by which we influence the behavior of a robot system in order to achieve the desired performance. We therefore need a control system because the real operation of the robot system can deviate from the desired operation. The robotic system is always located in an environment that also determines the robot's operating space. When controlling a system, ie a robot, we are talking about input and output parameters, and the control system itself acquires information about the system and the environment via sensors, and on the basis of these parameters and algorithms, determines the control signals used to control the robot. Here we are talking about influencing or input parameters and output parameters. An essential part of control, or process management or robot management, is therefore the real-time acquisition of various information such as coNo
- Information about the desired
- Information about the criterion that defines the modes of operation,
- Information about the management system,
- Information about nodding signals,
- Information about restrictions.
By observing the activity, we create an appropriate knowledge base that enables the robot to be guided to the desired goal. This is how we get to the step when the system thinks and decides. Here, the quality of management depends on the management method and the timeliness of the robot system's response. In order for the response to be adequate, the robotic system must act in such a way that it takes into account all the limitations of time, space and process parameters.
Thus, when controlling a robot, we are dealing with the environment, with goals, with criteria, with limitations, such as with observation, reasoning or learning, and with action. All these activities are carried out by the process computer in real-time, according to the appropriate steps, which is why we are talking about real-time closed-loop computer control of the robot. (Figure 1).
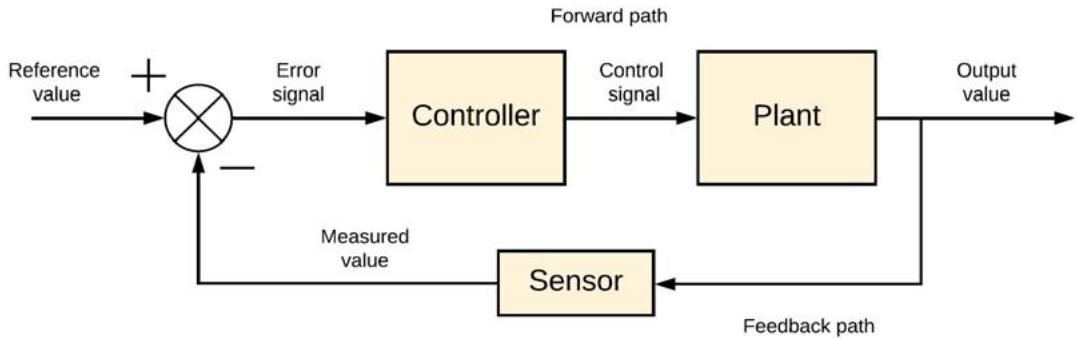 Figure 1: The basic principle of controlling the robot system
In this closed-loop control system, which is the basis for controlling individual robot assemblies, the error signal is the input to the control unit. The error signal is the calculated difference between the input desired signal and the feedback measured signal. By reducing the error, we stabilize the system output so that the desired value is reached at the system output. By using closed-loop control, the system minimizes system error. A block diagram from figure 1 representing a closed loop system and explaining the use of at least one sensor and controller e.g. robotic units. Output signal e.g. of the robot arm (of the system), is compared with the desired value in the summing unit. The difference between the two values, which represents an error, is transferred to the control unit, which, based on the built-in algorithm, manages the output control signal, e.g. robotic arm until the desired and output values are equal.
An important step in robot control is the development of a dynamic model of the robot and the working environment. Usually, in the modeling phase, we develop a non-linear mathematical model, which we transfer into the appropriate computer language. After the analysis and validation of the model, we move on to the synthesis phase of the robot control, the goal of which is the desired speed and accuracy of reaction when the desired values are changed. After planning the guidance, we move to the phase of evaluating the operation of the robotic system in a real environment, where we must take into account all the requirements that we determined at the beginning of planning the development of the process of guiding the surgical robot. During the entire planning, we must also take into account the dynamics of the robot and the flexibility of the joints of the robot manipulators. The dynamics of the robot is very non-linear, which is why even classical planning is difficult. Based on the variation of the limits, the control parameters are determined, with which we achieve the stability of the closed-loop system from Figure 1. The flexibility of the joints is an important component of the robot dynamics, but due to this flexibility, the control efficiency is very complex, if it is compared to the control of rigid robots.
For the sake of the complexity and flexibility of the robot joints, we start adaptive ticases, when the response of the robot system's environment is also time-varying, it is impractical to change the parameters for every change in the environment, which requires the use of an adaptive type of control model. The basic solution lies in the use of an adaptive robot control procedure.. control. Therefore, in doing so, we typically use two adaptation algorithms and they are:
- Least-Mean-Square LMS and
- Recursive-Least-Squares RLS,
Where the basic process of adjusting model weights is represented by the equation:
$$
w (k + 1) = w (k) + e (k) f \{d (k), x (k) \}
$$
Changes according to the Least-Mean-Square LMS algorithm are defined by the expression:
$$
w (k + 1) = w (k) + 2 \mu . x (k) e (k),
$$
where means expression
$$
0 < \mu < \frac {1}{\lambda m a x}
$$
learning speed.
With the Recursive-Least-Squares RLS algorithm, with the expression:
$$
w (k + 1) = w (k) + R ^ {- 1} (k) x (k) e (k)
$$
And expression
$$
R ^ {- 1} (k) = R ^ {- 1} (k - 1) - \frac {R ^ {- 1} (k - 1) x (k) x (k) ^ {T} R ^ {- 1} (k - 1)}{\lambda + x (k) ^ {T} R ^ {- 1} (k - 1) x (k)}
$$
where $\mathsf{R}^{-1}(\mathsf{k})$ stands for the inverse of the autocorrelation matrix of the string $x(k)$, symbol $\lambda$ represents maximum value of the autocorrelation matrix eigenvector. The RLS algorithm is computationally more complex, but despite its computational complexity, it is more accurate and much faster, therefore, it is more suitable for use in a real-world environment such as a robotic arm environment.
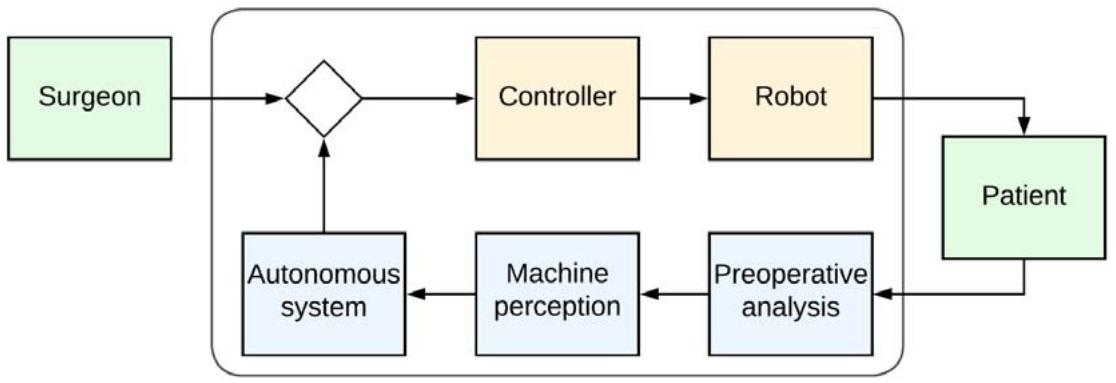 Figure 2: The System 3 level is capable of autonomously defining specifications for planning and performing a surgical task, while at level 2 all these specifications are determined by the surgeon /18/
The latest trend in management is the remote control of robots. These are operated by a human operator remotely. In remote work, despite new communication technologies such as 5G, there is a problem with the delay that occurs between the sensory feedback and the command that the remote operator gives to the manipulator. In order to overcome the delay dependence, the master-slave principle is introduced, which acts as a connector of two networks. With the advent of 6G communication technology, delays will be reduced to below 0.01ms, which will prevent unwanted interference when controlling the robot remotely.
### c) AI and Data in Surgical Robotics
Artificial intelligence actually simulates human intelligence using algorithms that run on computers. Thus, computer-aided systems using artificial intelligence perform tasks that require an intelligent approach similar to that of a human. The use of artificial intelligence (AI) and machine learning (ML) in medicine is increasingly intensive, as the amount and availability of clinical data increases. With the approach of using AI and ML in medicine, we can perform complex data interpretation and identify non-linearities that are not immediately noticed by classical statistical techniques.
People often wonder why data is important at all. Data quality is extremely important when performing data analysis, whether it will be used for artificial intelligence or not. The quality of the data has two components:
#### 1. Missing data
#### 2. Incorrect information
Both components are highly problematic, and the impact of the difficulty of each component can only be determined on a case-by-case basis. If data quality is not taken into account in the process of machine learning a model, then the analysis of the model leads to wrong conclusions.
Traditionally, structured data is the basis for effective quantitative analysis. As we know from the theory of systems management, response in addition to the properties of the system, the system depends on the signal at the input. Just as in machine learning, we also need data and AI; quality which means distinguishing between good and bad data. Bad data is a kind of noise, which causes the system output to respond incorrectly. These incorrect responses run the system, eg robot, in the wrong direction.
It also raises the question of what is the quality of the data? Here, the answer is subjective, as it depends on the field of application and methods of artificial intelligence. When parsing data sets we must pay attention to empty elements, or the indefinite e-element e of the data set. The data sets must consistently track the variables assigned to e.g. one v blood oxygen, another pressure, third temperature, etc. They must also be as perfect as possible, since we need to know the origin of data capture (sensor). We must trust these data sources, they must be accurate, but at the same time they must be valid. This means that data must be captured at the same time from other data sources.
Data accuracy is therefore key in model development, as in the application of AI methods. Because we collect data from different sources for system modeling, we must trust the data sources completely. If there are any virithat are not accurate, it will be our response distorted and you will not be able to get the correct answer. The data set must be valid, which is crucial for temporal data sets. The use of non-simultaneously captured givens may hinder the learning process, so we need a set of simultaneously captured givens.
At the same time, each piece of data must be unique and belong only to a certain set of variables i. For example, the oxygen data in the blood belongs only to one and not to several variables.
Quality and accurate givens we use them in operating theaters for simple support activities, as they can be used to recognize speech, visually detect objects, recognize patterns, and make appropriate decisions based on algorithms and recognized parameters ti. Artificial intelligence algorithms enable on-the-fly machine learning of natural language with real-time data capture, such as processing a, computer vision and and other data of vital functions. Based on this data and using AI and ML algorithms, robotic systems enable the automation of certain routine tasks and thus increase the efficiency of the entire surgical process.
As you can see, due to the nature of the work, surgery generates very large data sets that can be processed in detail and in depth using artificial intelligence methods. These data, in addition to those already mentioned, also include preoperative setup surgical data sets (patient clinical, laboratory, and imaging tests), intraoperative data only (based on video and kinematic data), and data sets including time, individual activities during the operation, the time of the entire operation, success rate of patient treatment and quality criteria of the performed procedure.
### d) Artificial Intelligence to Support Surgeons in Decision-Making
Performing a classic operative intervention, the surgeon's decision-making is dominated primarily by hypothetical-deductive reasoning, his individual judgment and heuristics. Such decision-making can lead to bias, error, and preventable harm. Artificial intelligence with predictive analytics, as well as clinical decision support systems, are aimed at increasing the quality of surgeon decision-making. In cases of manual data capture and manual analysis by participating staff, the clinical utility of these data is compromised and thus the success of the intervention. The problem can be overcome by the real-time application of models and artificial intelligence on a set of data captured in real-time from electronic health devices and patient records. This approach requires standardization of data, advances in model interpretability, careful implementation and monitoring, attention to ethical challenges involving algorithm bias and liability for error, and retention of treatment performance status assessment and human intuition in the decision-making process.
Linking artificial intelligence to surgeon decision-making can improve the surgical process, subsequent care, identification and mitigation of risk factors, decisions about postoperative control, and shared decisions about the use of all resources.
Artificial intelligence is helpful for surgeons in the understanding and critical evaluation of the new surgical procedures, or research and development thereof. Obtaining good data to develop algorithms in medicine is expensive and time-consuming. The use of artificial intelligence in surgery itself, supported by methods of real-time recognition of the scene, service process, speech, etc., is developing more slowly than in other areas of medicine. The biggest reason is the complexity of operations and thus mainly the lack of appropriate data structures, real-time capture during the implementation of the operative procedure.
As we have already mentioned, the use of artificial intelligence algorithms in surgical learning enables quality learning and training, such as preparing the surgical team for samo surgery. With the introduction of simulation procedures based on deep learning and artificial intelligence, surgical training has undergone significant changes in all areas in recent years. Artificial intelligence is particularly useful for creating surgical simulations, allowing trainees to practice skills in a controlled environment and develop a better understanding of the complex task of surgery.
Looking at the advantages of operating simulators, we see them as an excellent way to teach trainee surgeons to established surgeons in a low-risk environment or when developing new techniques. Training surgeons with simulators reduces the number of risks, reducing errors during the procedure, thereby reducing the risks and mortality rate due to medical errors.
Studies have shown that students who use simulators perform better and retain more of what they learn than their counterparts who use more traditional methods of medical training. In fact, in one medical aptitude test, 20 students who used high-tech simulators far outperformed students who used traditional training /21/.
Compared to older methods, training with a simulator enables faster interventions, the presence of auxiliary staff is less and takes less time, the costs of the intervention are lower, and the probability of a successful intervention is disproportionately higher.
From that what has been said, we can see that artificial intelligence has a huge potential in the field of surgery, so the use of the mentioned methods together with simulators of surgical interventions it is necessary to include it in the daily work of surgeons. Considering the state of new technologies in surgery, it is necessary to expand medical study programs by teaching the mentioned methods, i.e. to familiarize students with the use of artificial intelligence and simulation procedures in healthcare and medical robotics. Medical education institutions must better prepare medical students for changing technologies, as well as for increasingly knowledgeable patients who are increasingly knowledgeable about their illnesses, than they once were. Doctors of the future must be prepared for this new reality. At the same time, it is necessary to encourage patients to be more responsible for their health.
### e) Surgical Robots in the Real World
The fact that even in surgery the bodies are moving introduces additional complexity for the surgeon, let alone for the surgical robot. Some robots that already show a certain level of autonomy can be used in operations for performing simple routine tasks. What is e.g. Tibia - tibia fixed, it's relatively easy to work with and doesn't move much once it's locked into place. Unfortunately, certain parts of the body are not so easy to fix in place. For example, muscles contract, stomachs rumble, brains wiggle, and lungs expand and contract even before the surgeon begins the operation. Although the surgeon obviously sees and feels that when these organs are moving, how does the robot know if his scalpel is in the right place or if the tissues have moved? The solution to such dynamic inclusions combine the use of cameras and sophisticated tracking of tissue movement software in real time. A person as a surgeon marks certain points on the tissue with drops of fluorescent glue and create markers that the robot can follow. At the same time, the camera system creates a 3-D model of the tissue using a grid of light points projected onto the area. With the support of the software, the robot sees changes in the projected network and thus perceives, i.e. "sees" the actual state that is before him.
Today, robots that observe human actions and learn from these actions, according to one of the ML algorithms. Based on this type of learning, robots already predict the actions of their human counterparts. This method of predictive control allows robots to proactively plan and execute actions based on anticipating the action of a human partner. /[15] Huang,
C. M., & Mutlu, B. Anticipatory Robot Control for Efficient Human-Robot Collaboration/. Research has proven that monitoring user actions helped to improve cooperation and the efficiency of task performance /16/. Robot manipulators thus more accurately perform tasks that are otherwise performed by humans, because humans are not limited by their intelligence, but rather by their physical strength. We overcome these kinds of problems with robots.
Over the years, much has been thought about the structure of the psychological characteristics of human-robot joint action. Among the various factors, perfectly coordinated action was also related to the formation of expectations
The actions of the first partner towards the second and also the consequent fulfillment of these expectations [14, 17].
Thus, robotic manipulators have become a standard application in surgical medicine, where management and also the harmony between surgeon and robot is well performed by AI-based programs.
# f) The
In Slovenia, we are still developing robots at the first level of autonomy, where the robot is able to provide physical assistance to the surgeon. The characteristic of surgical robots at the lowest level is that all management decisions are left to the surgeon.

Slika 3: Collaborative robot MOTOMAN, Yaskava Kočevje In this direction, new collaborative robot development programs are also underway at Yaskava and Kočevje (picture 3), while the University of Ljubljana and the Jožef Stefan Institute are primarily engaged in research into rehabilitation robots. The development trends that we are pursuing in Slovenia are aimed at robotic systems that actively cooperate with the surgeon. This objective represents level 1 which actually provides active assistance to the surgeon. At this level, robots perform activities that affect the surgeon's intervention, which means limiting the movement of surgical instruments based on knowledge of the environment. Image sensors are important here, such as force sensors, which alert the surgeon to prohibited areas in advance. At this level, the robot se responds to
the actions of the surgeon and has no control over the execution of individual steps of the surgical procedure.
It also continues to develop advanced robotic components such as mechatronic assemblies for robots, advanced sensor-based robotic control systems, smart robotic effectors, laser and vision systems in robotics.
The field of development of advanced robotic systems in Slovenia also includes cognitive robotic systems, advanced human-robot interfaces, two- and multi-handed robotic systems, robotic diagnostics, mobile robotic platforms, mini-, micro- and nano-robot systems, environmental, medical and agro robotics. We also devote a large part of our research to the field of advanced control of robotic systems,
2D and 3D robotic vision for adaptive robot control, advanced robotic learning, and collaborative and reconfigurable robotics. In view of the development of 5G and 6G communication technologies, we are also devoting ourselves to research into connecting robotic systems with the Internet of Things, as well as control systems in robotics.
## IV. CONCLUSION
With the use of a smart robot, the surgeon's job will be much easier. Pthan the smart robot b Warns similar to a smart system in a car that looks for us drivers of road hazards, restrictions and the effects of the weather on the roads. Just as the driver focuses on the driving itself, the doctor will also focus on the problem itself, eg removal of cancer. Individual authors in the literature even claim that the use of a soft robot even reduced the need for anesthesia. Since there is still no possibility for the robot to be completely autonomous, today's partial autonomy technology is already a great help to surgeons around the world.
Today's robots are only used for simpler tasks, such as holding a camera, for monitoring vital functions, for understanding spoken language, and performing eg delivery of the instrument to the operator, etc. The plan also goes in this direction, developing a robot assistant in Slovenia that should help the surgeon change instruments when necessary.
Thus, robotic manipulators have become a standard application in surgical medicine, where management and also the harmony between surgeon and robot is well performed by AI-based programs.
If we conclude with thoughts about the future, we can conclude that robotic surgery has great advantages over classical surgery. The big advantage of robotic surgery over classical surgery is tudi tathat it enables surgery through smaller incisions, that it enables greater work precision, as the movements of the robotic arm are more precise than human ones, better visualization is enabled, as it enables insight into 3D high resolution and recognition of objects that are sometimes not visible to the naked eye. Because the surgeon performs surgery with a robotic arm, the surgeon can use very small jinstruments to perform surgery inside the body. Recovery after robotic surgery is much shorter. Depending on the type of procedure, the patient can get up soon, the hospital stay is shorter, the effect of anesthesia wears off faster, sometimes patients can easily return home the very next day after the procedure.
A big advantage of using a robot supported by artificial intelligence is the possible st šudija virtual representation of the entire operation process, the study aof better solutions and the advance epreparation of the entire team for the robot-assisted operation itself. Therefore, it makes sense to introduce super specializations and to introduce study programs in the fields of radiology, artificial intelligence and medicine, simulation procedures, visualization and 3D printing, for example, of.bone implants or trenutnim potrebam modified instruments. All t ovrstniprograms must be included tudi in the study program of a medical engineer, teh and tekom rednega študija medical students must also be informed about technology reviews. Le z izvrstnim poznavanjem problema in študija rešitev we will increase the quality and at the same time reduce the costs of treatment.
### Thought:
"Medical staff and AI have to monitor a person even before the appearance of illness."
Generating HTML Viewer...
References
23 Cites in Article
G Gomez (2004). Emerging Technology in surgery: informatics, electronics.
Andrea Moglia,Konstantinos Georgiou,Evangelos Georgiou,Richard Satava,Alfred Cuschieri (2021). A systematic review on artificial intelligence in robot-assisted surgery.
Jennifer Polinski,Tobias Barker,Nancy Gagliano,Andrew Sussman,Troyen Brennan,William Shrank (2016). Patients’ Satisfaction with and Preference for Telehealth Visits.
T Nesbitt (2005). Unknown Title.
A Uscher-Pinesandmehrotra (2014). Unknown Title.
Andrija Grustam,Johan Severens,Daniele De Massari,Nasuh Buyukkaramikli,Ron Koymans,Hubertus Vrijhoef (2018). Cost-Effectiveness Analysis in Telehealth: A Comparison between Home Telemonitoring, Nurse Telephone Support, and Usual Care in Chronic Heart Failure Management.
M Thygeson (2008). Unknown Title.
A Sussman (2013). Corrigendum for Stamateris et al., volume 305, 2013, p. E149–E159.
Laurence Baker,Scott Johnson,Dendy Macaulay,Howard Birnbaum (2011). Integrated Telehealth And Care Management Program For Medicare Beneficiaries With Chronic Disease Linked To Savings.
L Maier-Hein,S Vedula,Speidel (2017). Surgical data science for next generation interventions.
G Riva,J Water Worth (2003). Presence and the Self: A cognitiveneuro science approach.
Chien-Ming Huang,Bilge Mutlu (2007). Anticipatory robot control for efficient human-robot collaboration.
Günther Knoblich,Jerome Jordan (2003). Action coordination in groups and individuals: Learning anticipatory control..
Aleks Attanasio,Bruno Scaglioni,Elena De Momi,Paolo Fiorini,Pietro Valdastri (2021). Autonomy in Surgical Robotics.
Carla Pugh,Stephen Plachta,Edward Auyang,Aurora Pryor,Eric Hungness (2010). Outcome measures for surgical simulators: Is the focus on technical skills the best approach?.
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.