I. INTRODUCTION
Lipofibromatous hamartoma (LFH) is a rare condition characterized by the infiltration of peripheral nerves by fibrous and adipose tissues. Patients typically present with gradually enlarging, nontender lesions in the distribution of the affected nerve, most commonly the median nerve, which is involved in to of cases. Symptoms often include pain, sensory deficits, and motor dysfunction, with affected individuals reporting numbness and tingling along the volar aspect of the wrist and hand. Motor deficits tend to appear later in the course of the condition [1].
Congenital factors have been suggested in the etiology of LFH, sometimes associated with macrodactyly, where enlarged digits follow the median nerve's course [2]. Syndactyly has also been documented in association with LFH [3]. A family history of neurofibromatosis type 1 is pertinent, as this condition can lead to associations with malignant peripheral nerve sheath tumours and schwannomas.
Patients may exhibit neurological deficits, including hypoesthesia and decreased grip strength, as well as positive Tinel's and Phalen's tests [4]. Many individuals report a history of asymptomatic swelling that progresses to functional impairment over months or years. Differential diagnoses for LFH include benign tumours such as ganglion cysts [5], and tumours with malignant potential such as neurofibromas [6] and schwannomas [7, 8]. It is also essential to exclude malignant conditions, including liposarcoma [9] and malignant peripheral nerve sheath tumours [10].
Imaging studies play a critical role in the diagnosis of LFH. Common modalities include radiography, ultrasound, and MRI. MRI typically reveals fusiform or hourglass-shaped enlargement of the median nerve, with characteristic low-intensity serpentine nerve bundles embedded in hyperintense adipose tissue, often described as having a "coaxial cable-like" appearance [11-15]. Electromyogram (EMG) and nerve conduction studies (NCS) often show decreased sensory and motor conduction, fibrillation potentials, and signs of compressive neuropathy [16, 17].
Histopathological examination remains the definitive diagnostic method for LFH, revealing interlacing collagen, fibroblasts, and mature adipocytes, often infiltrating the nerve fascicles [18]. The nerve fibres typically appear normal, with no signs of inflammation or degeneration [19]. Management of LFH is individualized; while complete excision was historically the standard approach, it can lead to significant sensory and functional impairments [20]. Expectant management is an option for asymptomatic patients, although spontaneous regression is rare, and lesions may continue to enlarge, leading to compressive neuropathy.
II. CASE REPORT
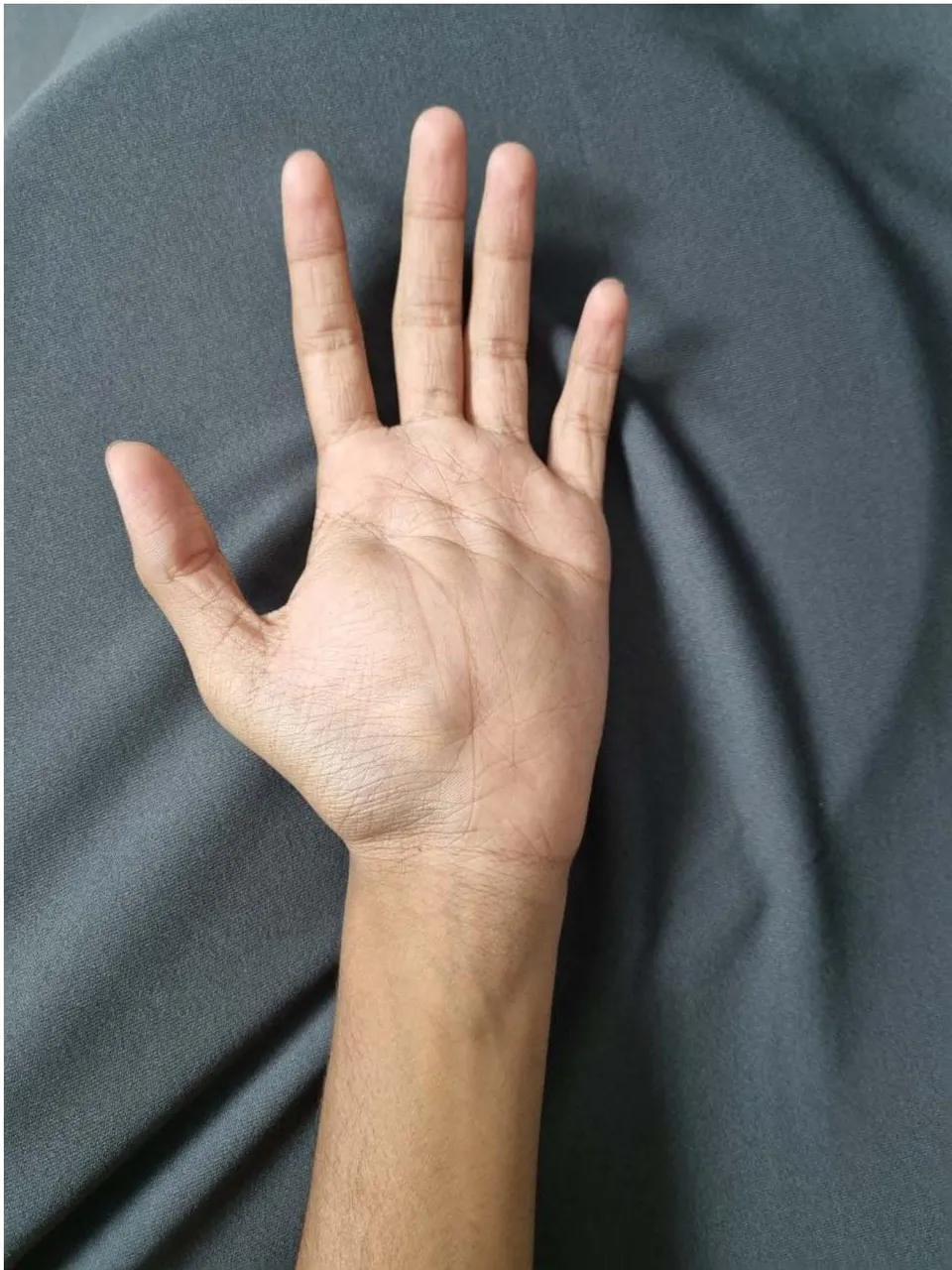
A right hand dominant 16-year-old male presented with complaints of swelling in the left palm and wrist region for the past six years, which had gradually increased in size over four years (Figure 1). Patient gave history of pain over the palm and paraesthesia over radial three digits. Patient also complained of difficulty in gripping or grasping activities. There was no history of trauma to the hand, diabetes mellitus, or hypertension. No other significant past history or family history was noted.
On physical examination, a smooth, partially mobile, fusiform-shaped, non-tender swelling, soft in consistency measuring approximately was observed over the volar aspect of the left wrist region and over the left palm, with no associated skin changes. Sensations was intact to light touch. The two point discrimination over the radial three digits was and was normal in the rest. The movements at all joints were normal, mild restriction secondary to the mass over the palm. The rest of the physical examination was unremarkable.
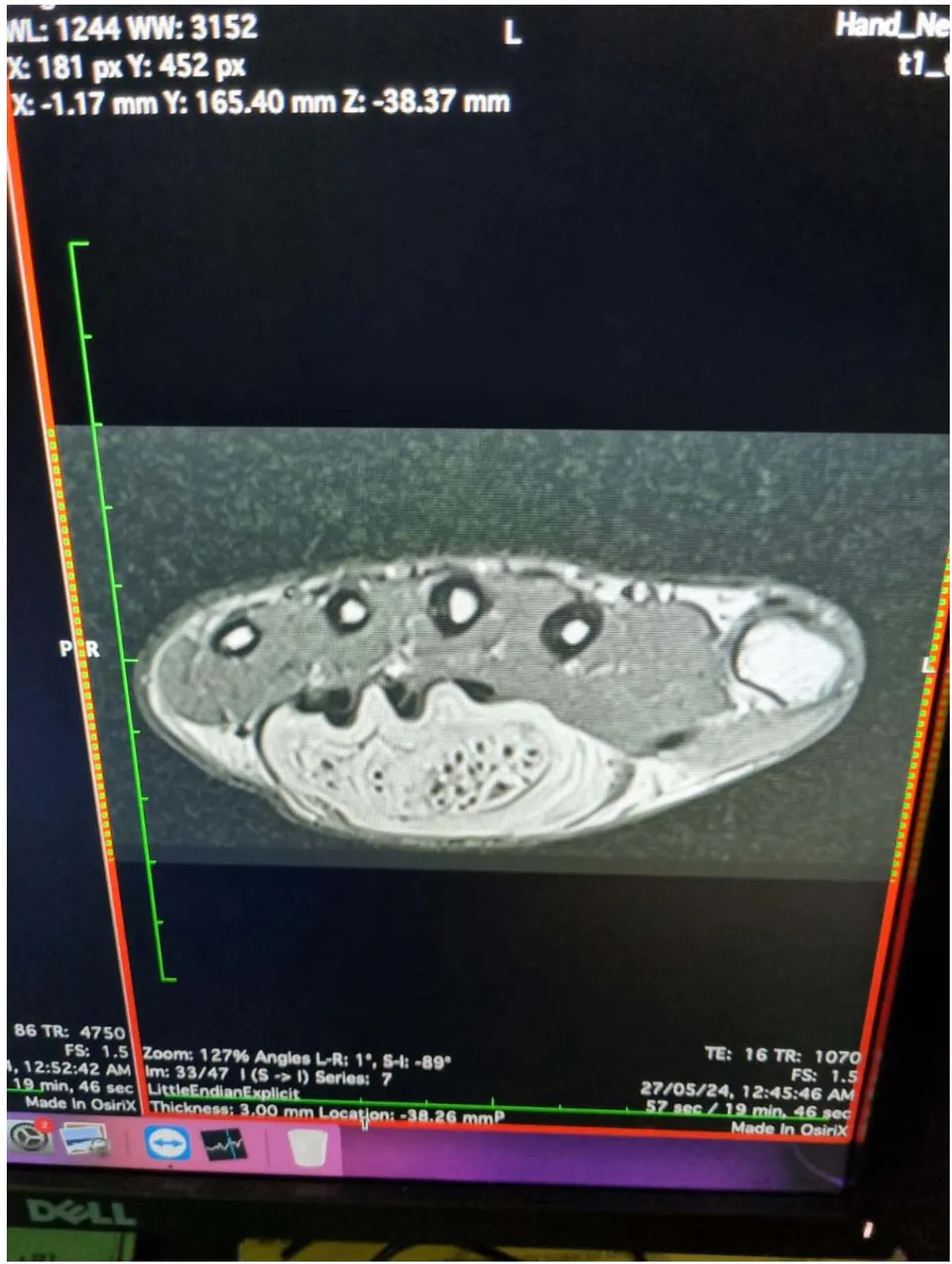
All routine blood investigations with Xray of left hand was done. Plain radiograph showed no bony abnormality. The possible differential diagnoses considered were ganglion cysts, vascular malformations, schwannomas, neurofibromas, and lipomas. An ultrasound of the wrist revealed enlarged and hypoechoic nerve fascicles surrounded by echogenic fat tissue, giving a "cable-like appearance" on axial images. MRI of the left wrist, showed diffuse thickening of nerve fascicles of the median nerve, extending from the distal forearm to the wrist and into the distal palmar region. There was diffuse and extensive interfascicular and perineural lipomatous infiltration, with the nerve fascicles shows mild diffuse enhancement on post-contrast study. The radiological diagnosis was fibro lipomatous hamartoma of the median nerve.
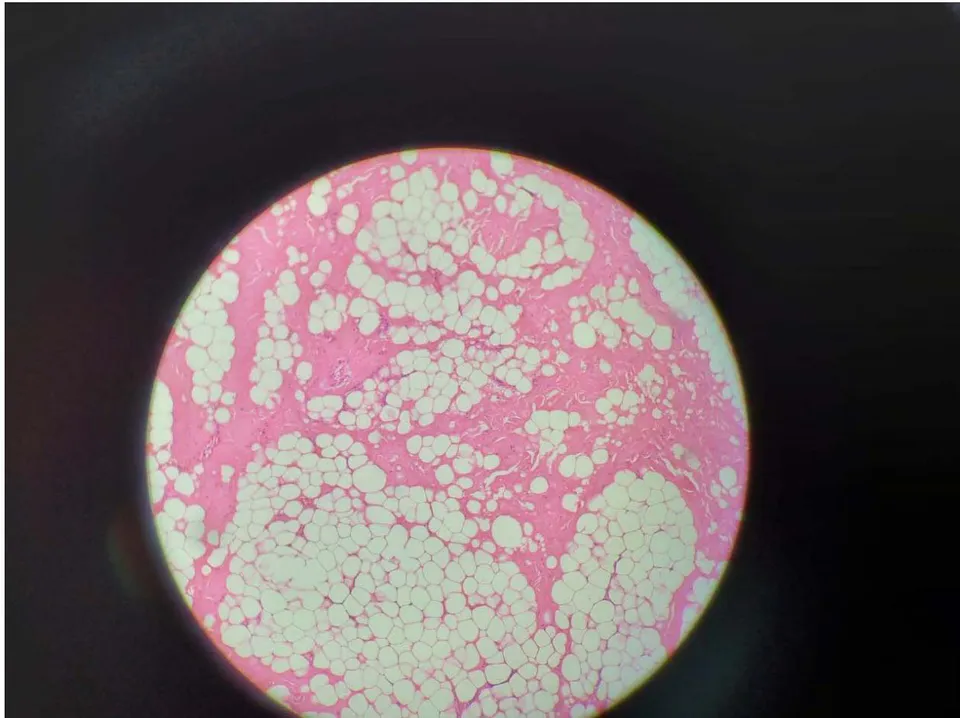
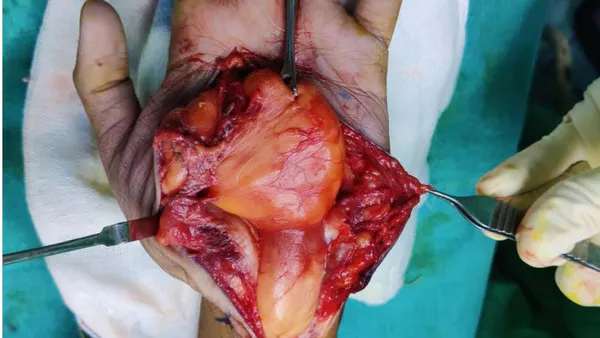
Intraoperatively, mid palmar incision extending to the wrist and distal forearm taken and exploration done. Transverse carpal ligament incised and carpal tunnel opened. A cm yellowish lipomatous mass was found encompassing the median nerve at the palm, wrist and distal half of forearm proximally and distally till the common and proper digital nerves of the left thumb, index and middle finger and common digital nerve of middle-ring fingers, as shown in Figure 4. The tumour was carefully dissected and debulked over the palm, with the continuity of the nerve proper and digital nerves maintained, as seen in Figure 5, 6. The specimen along with a part of epineurium sent for histopathological analysis, which confirmed the intraoperative diagnosis of Fibro lipomatous Hamartoma of the median nerve with extensive hyalinised collagen bundles in which single fibroblasts are randomly scattered as shown in Figure 7. The post operative image of the Left Hand and the excised specimen are seen in Figure 2, 3.
After Surgery, the patient continued to have all movements and sensations to light touch. Two point discrimination remained unchanged from pre-surgical status. Patient's post operative period was uneventful. Post operative follow-up for 1 month was uneventful.
III. DISCUSSION
LFH, affecting fewer than 200 cases involving the median nerve, was first reported in 1953 [1]. The term "lipofibromatous hamartoma" was coined in 1969 [3], and various names have been used, complicating its diagnosis [4-6]. The condition is thought to arise from congenital malformations or trauma [4, 10-14].
LFH preferentially affects the median nerve, leading to symptoms consistent with nerve compression and carpal tunnel syndrome. Historically, complete excision was the standard treatment, often resulting in significant sensory and motor deficits [24]. Today, conservative management may be preferred in select cases.
IV. CONCLUSION
Fibro lipomatous hamartoma of the median nerve is a rare congenital condition that commonly affects the median nerve. Understanding this condition aids in accurate diagnosis, potentially reducing the need for invasive procedures like biopsies.
Campbell CS, Wulf RF. Lipoma Producing a Lesion of the Deep Branch of the Radial Nerve. J Neurosurg. 1954;11:310-311.
Fitoussi F, Ilharreborde B, Johanno P. Macrodactylie. Chir Main. 2009;28:129-37.
Meyer BU, Roricht S, Schmitt R. Bilateral fibrolipomatous hamartoma of the median nerve with macrocheiria and late-onset nerve entrapment syndrome. Muscle Nerve. 1998;21:656-8.
Feyerabend T, Schmitt R, Lanz U, Warmuth-Metz M. CT morphology of benign median nerve tumors. Report of three cases and a review. Acta Radiol. 1990;31:23-5.
Nahra ME, Bucchieri JS. Ganglion cysts and other tumor related conditions of the hand and wrist. Hand Clin. 2004;20:249-60.
Woertler K. Tumors and tumor-like lesions of peripheral nerves. Semin Musculoskelet Radiol. 2010;14:547-58.
Basheer H, Rabia F, el-Helw K. Neurofibromas of digital nerves. J Hand Surg Br. 1997;22:61-3.
Razzaghi A, Anastakis DJ. Lipofibromatous hamartoma: review of early diagnosis and treatment. Can J Surg. 2005;48:394-9.
Fnini S, Hassoune J, Garche A, Rahmi M, Largab A. Giant lipoma of the hand: case report and literature review. Chir Main. 2010;29:44-7.
Perrin RG, Guha A. Malignant peripheral nerve sheath tumors. Neurosurg Clin North Am. 2004;15:203-16.
Chand G, Chowdhury V, Singh S. Median nerve hamartoma: findings on magnetic resonance imaging. Ann Indian Acad Neurol. 2008;11:259-60.
Declercq H, Deman R, Vanherck G, Tanghe W, Lateur L. Case report-diagnosis-fibrolipoma of the median. Skeletal Radiol. 1993;22:610-613.
Evans HA, Donnelly LF, Johnson ND, Blebea JS, Stern PJ. Fibrolipoma of the median nerve: MRI. Clin Radiol. 1997;52:304-7.
Lowenstein J, Chandnani V, Tomaino MM. Fibrolipoma of the median nerve: a case report and review of the literature. Am J Orthop (Belle Mead NJ) 2000;29:797-8.
Pang HN, Puhaindran M, Yong FC. Fibrolipoma of multiple nerves in the wrist. Singapore Med J. 2009;50:283-86.
Afshar A. Carpal tunnel syndrome due to lipofibromatous hamartoma of the median nerve. Arch Iran Med. 2010;13:45-7.
Bains R, Kotwal A, Saeed W. Recurrent carpal tunnel syndrome in a child due to fibrolipomatous hamartoma of the median nerve successfully
- treated by limited excision and decompression. J Plast Reconstr Aesth Surg. 2006;59:1394-7.
Colombat M, Carton S, Dunaud JL. Unevolumine use tumefaction delapaumedelamain. Ann Pathol. 1999;19:543-4.
Louis DS, Hankin FM, Greene TL, Dick HM. Lipofibromas of the median nerve: Long-term follow-up of four cases. J Hand Surg Am. 1985;10:403-8.
Bergman FO, Blom SE, Stenstrom SJ. Radical excision of a fibro-fatty proliferation of the median nerve, with no neurological loss symptoms. Plast Reconstr Surg. 1970;46:375-80.
Mason ML. Presentation of cases: Proceedings of the American Society for Surgery of the Hand. J Bone Joint Surg Am. 1953;35A:273-4.
Emmett AJ. Lipomatous hamartoma of the median nerve in the palm. Br J Plast Surg. 1965;18:208-13.
Johnson RJ, Bonfigli M. Lipofibromatous hamartoma of median nerve. J Bone Joint Surg Am. 1969;51:984-90.
Mikhail IK. Median nerve lipoma in the hand. J Bone Joint Surg Br. 1964;46:726-30.
Declaration
The written informed consent of the participant was obtained and that the study was approved by an institutional ethics board. All studies were carried out in accordance with the World Medical Association Declaration of Helsinki, covering the latest revision date.
Conflict of interest: none
Funding: none
Figures