The Role Of Hemolysis In The Development Of Arrhythmias In Patients With Ischemic Heart Disease After Coronary Artery Bypass Grafting Under Artificial Circulation
## I. INTRODUCTION
Coronary artery bypass surgery in patients with coronary heart disease (CHD) is frequently associated with postoperative complications, with arrhythmias being a significant concern [1, 2]. Potentially life-threatening arrhythmias, such as ventricular fibrillation and tachycardia, and third-degree atrioventricular block, as well as hemodynamically significant arrhythmias like atrial fibrillation (AF), severe bradycardia, and severe sinus tachycardia, are common. AF, a highly prevalent and dangerous postoperative arrhythmia, is frequently observed (25-65% of cases) [3] and is associated with adverse outcomes, including increased risk of heart failure progression, thromboembolism, prolonged hospitalization, and mortality [4]. Patients experiencing AF after CABG have a higher risk of mortality related to cerebrovascular accidents and myocardial infarction [4]. The pathogenesis of CABG-related arrhythmias is complex and not fully understood. Perioperative and early postoperative arrhythmias likely represent a reaction of the conduction system to the altered blood flow during the surgery, including the transition from cold cardioplegia to reperfusion [5-11]. Reoxygenation following the restoration of coronary blood flow can induce oxidative stress, metabolic disturbances, and electrical heterogeneity in the myocardium [5]. Further, the use of cardiopulmonary bypass (CPB) during CABG, necessary for maintaining blood circulation during the operation, is associated with potential red blood cell damage. This hemolysis may contribute to the development of cardiovascular complications in the postoperative period [12]. However, the specific relationship between intraoperative hemolysis (IOH) and the development of arrhythmias following CABG remains unclear in the existing literature.
## II. PURPOSE OF THE STUDY
To establish the connection of intraoperative hemolysis (IOH) with the development of cardiac rhythm disturbances in patients with coronary artery disease after coronary shunting in conditions of cardiopulmonary bypass (CB).
## III. MATERIALS AND METHODS
It was performed a prospective study of 123 patients with coronary heart disease undergoing CABG. The study was consistent with the Helsinki Declaration of the World Medical Association «Ethical Principles for
All patients underwent CB surgery in a planned manner under IR conditions. According to the level of free hemoglobin [Hb] in blood plasma, which is a marker of the degree of IOH, patients are divided into three groups: group 1 - without IOH (Hb ≤ 0.1 g/l), n=43, group 2 - with low IOH(IIOH) - with [Hb] > 0.1g/l and < 0.5 g/l, n=42, group 3 - with a high IOH (hIOH) corresponded to [Hb] ≥ 0.5 g/l, n=38. The degree of IOH was assessed by the level of free hemoglobin [Hb] in the blood plasma at the beginning of the operation, immediately after connecting the patient to the artificial device and 15 minutes before removal from the artificial device (Fig. 1), using a Hemo Cue Plasma/Low Hb analyzer, Sweden [12].
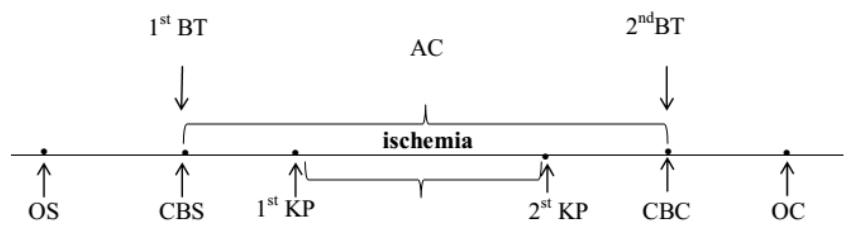
Figure 1: Diagram of the Coronary Bypass Surgery Operation
CB - Cardiopulmonary Bypass
CB - Cardiopulmonary Bypass Start
CB - Cardiopulmonary Bypass Completion
KP - Cardioplegia
OS - Operation Start
OC - Operation Completion
1st BT - First Blood Test
$2^{nd}BT$ - Second Blood Test
Patients of all groups are comparable by age and gender (Table 1).
Table 1: Clinical Characteristics of the Subjects
<table><tr><td>Indicator</td><td>Group 1
n=43</td><td>Group 2
n=42</td><td>Group 3
n=38</td></tr><tr><td>Age, years</td><td>60 (56; 63)</td><td>64 (58; 66)</td><td>66 (60; 68)</td></tr><tr><td>Gender (male),%</td><td>36 (87.8%)</td><td>32 (78.0%)</td><td>31 (78.0%)</td></tr><tr><td>BMI (kg/m2)</td><td>27.8(24.7; 29.2)</td><td>27.7 (24.8; 29.2)</td><td>29.1(25.9; 32.2)</td></tr><tr><td>Total protein (g/l)</td><td>69 (62; 71)</td><td>69(58; 68)</td><td>66(57; 67)</td></tr><tr><td>Glucose, mmol /L</td><td>5.0(4.5; 5.6)</td><td>5.2(4.4; 6.1)</td><td>5.3(4.5; 6.2)</td></tr><tr><td>Cholesterol, mmol /L</td><td>4.1(3.3; 5.0)</td><td>4.6(3.2; 5.7)</td><td>5.0(4.6; 5.6)</td></tr><tr><td>Urea, mmol /L</td><td>5.3(4.8; 5.6)</td><td>6.0(5.5; 7.6)</td><td>6.4(5.5; 7.2)</td></tr><tr><td>Creatinine, mmol /l</td><td>99(89; 104)</td><td>105(98; 110)</td><td>106(99; 112)</td></tr><tr><td>CRP (mg/ml)</td><td>1.2(0.8; 1.4)</td><td>1.1(0.8; 1.3)</td><td>1.0(0.6; 1.2)</td></tr></table>
Notes: Data are presented as Me $[Q_{25}; Q_{75}]$, where Me is the median, $Q_{25}$ is the value of the lower quartile; $Q_{75}$ is the value of the upper quartile.
All patients underwent surgical intervention using a standard anesthetic protocol under normothermic artificial circulation conditions with a hemodilution level of hematocrit of $25 - 30\%$.
The groups did not differ in the duration of artificial circulation and the time of myocardial ischemia $(p>0.05)$, Table 2.
Table 2: Duration of Cardiopulmonary Bypass (CB) and Myocardial Ischemia in Patients with Varying Degrees of IOH during Coronary Artery Bypass Grafting
<table><tr><td>Indicator</td><td>Group 1
n=43</td><td>Group 2
n=42</td><td>Group 3
n=38</td></tr><tr><td>Ischemia-reperfusiontime (min)</td><td>69(65; 89)</td><td>74 (68; 78)</td><td>80 (75; 94)</td></tr><tr><td>Ischemiatime (min)</td><td>46(39; 64)</td><td>58(56; 62)</td><td>59(51; 68)</td></tr></table>
Note: The data are presented in the form Me $(Q_{25};Q_{75})$, where Me is the median of the indicator; $Q_{25}$ - value of the lower quartile; $Q_{75}$ is the value of the upper quartile.
Most patients $(85\%)$ underwent mammary-coronary bypass surgery in combination with aortic-coronary bypass surgery. Mammary-coronary bypass surgery was performed in $4\%$ of patients $(p < 0.05)$, aortic-coronary bypass surgery - in $11\%$ of patients $(p$
<0.05). Groups were comparable in frequency (p> 0.05).
More often, lesions of three or more coronary arteries, CA (63.1%) and significantly less often than one CA (7.1%) were revealed, Table 3.
Table 3: Characterization of Shunts in Patients with Coronary Heart Disease in Groups with Different Levels of IOH
<table><tr><td>Number of Shunts</td><td>Group1
n=43</td><td>Group 2
n=42</td><td>Group 3
n=38</td><td>p1-2</td><td>p1-3</td><td>p2-3</td></tr><tr><td>1</td><td>9,9</td><td>7,5</td><td>10,8</td><td>0,412</td><td>0,510</td><td>0,314</td></tr><tr><td>2</td><td>31,0</td><td>26,8</td><td>39,2</td><td>0,510</td><td>0,610</td><td>0,094</td></tr><tr><td>3 andmore</td><td>59,1</td><td>65,7</td><td>50,0</td><td>0,462</td><td>0,130</td><td>0,318</td></tr><tr><td>Left anterior interventricular coronary artery</td><td>87,8</td><td>100</td><td>100</td><td>0,21</td><td>0,31</td><td>0,31</td></tr><tr><td>Left circumflex artery</td><td>4,9</td><td>7,3</td><td>19,5</td><td>0,644</td><td>0,420</td><td>0,105</td></tr><tr><td>Posterior interventricular branch of left circumflex artery</td><td>14,6</td><td>39,0</td><td>61,0</td><td>0,210</td><td>0,310</td><td>0,406</td></tr><tr><td>Left marginal artery</td><td>56,1</td><td>65,9</td><td>80,5</td><td>0,172</td><td>0,22</td><td>0,324</td></tr><tr><td>Right coronary artery</td><td>24,4</td><td>58,5</td><td>61,0</td><td>0,231</td><td>0,341</td><td>0,821</td></tr><tr><td>Right interventricular branch artery</td><td>17,07</td><td>34,15</td><td>26,8</td><td>0,706</td><td>0,285</td><td>0,471</td></tr></table>
Note: Accordingly, with myocardial revascularization, three or more coronary arteries (CA) were shunted more often - $56.9\%$ of patients. The most common lesions were observed in the anterior interventricular branch of left coronary artery $(p < 0.05)$, posterior interventricular branch of the left circumflex artery $(p < 0.05)$ and the left marginal artery $(p < 0.05)$. Table 4 presents the nosological characteristics of patients.
Table 4: Nosological Characteristics of Patients with Coronary Artery Disease before Coronary Bypass Surgery with Varying Degrees of Intraoperative Hemolysis (IOH)
<table><tr><td>Indicator</td><td>Gr 1
n=43</td><td>Gr 2
n=42</td><td>Gr 3
n=38</td></tr><tr><td>Ischemic heart disease duration</td><td>8,5
(4,2; 11,4)</td><td>8,9
(4,6; 10,8)</td><td>9,5
(6,2; 12,1)</td></tr><tr><td>Durationofhypertension</td><td>10 (6; 11)</td><td>8 (5; 10)</td><td>11,5 (9; 15)</td></tr><tr><td>Functional class II</td><td>9 (20,1%)</td><td>11 (26,2%)</td><td>6 (15,8%)</td></tr><tr><td>Functional class III</td><td>34 (79,9%)</td><td>31(73,8%)</td><td>32 (84,2%)</td></tr><tr><td>Postinfarctioncardiosclerosis</td><td>37 (86,1%)</td><td>36 (85,7%)</td><td>33 (86,8%)</td></tr><tr><td>The number of myocardial infarction (2 MI) in the history</td><td>16(37,2%)</td><td>18(42,8%)</td><td>13(34,2%)</td></tr><tr><td>NYHAII</td><td>36(83,7%)</td><td>31(73,8%)</td><td>33(86,8%)</td></tr><tr><td>NYHAIII</td><td>7(16,3%)</td><td>11(26,2%)</td><td>5(13,2%)</td></tr><tr><td>Ischemic cardiomyopathy</td><td>2 (0,86%)</td><td>3 (1,26%)</td><td>2 (0,76%)</td></tr><tr><td>Historyofarrhythmias</td><td>7(16,3%)</td><td>7(16,6%)</td><td>6(15,4%)</td></tr><tr><td>Paroxysmofatrial fibrillation</td><td>0 (9%)</td><td>1(0,42)</td><td>1 (0,38%)</td></tr><tr><td>supraventricular extrasystole</td><td>4(1,72%)</td><td>2 (0,84)</td><td>2(0,76%)</td></tr><tr><td>ventricular extrasystole</td><td>1(0,43%)</td><td>1 (0,42%)</td><td>1(0,38%)</td></tr><tr><td>right His bundle branch block</td><td>1(0,43%)</td><td>1 (0,42%)</td><td>1(0,38%)</td></tr><tr><td>left His bundle branch block</td><td>1(0,43%)</td><td>2 (0,42%)</td><td>2(0,76%)</td></tr><tr><td>bloodhypertension</td><td>36 (87,8%)</td><td>38(90,2%)</td><td>38(92,7%)</td></tr><tr><td>chronicbronchitiswithoutexacerbation</td><td>7(16,3%)</td><td>9(21,4%)</td><td>12(31,6%)</td></tr><tr><td>gastropathy</td><td>18(41,9%)</td><td>17(40,5%)</td><td>20(52,6%)</td></tr><tr><td>urolithiasis</td><td>6(13,9%)</td><td>9(21,4%)</td><td>7(18,4%)</td></tr><tr><td>osteoarthritis</td><td>0(0%)</td><td>3(7,1%)</td><td>1(2,6%)</td></tr><tr><td>excessBWandobesity</td><td>36(83,7%)</td><td>31(73,8%)</td><td>33(86,8%)</td></tr><tr><td>excessBWI</td><td>22(51,2%)</td><td>18(42,9%)</td><td>18(47,4%)</td></tr><tr><td>obesity</td><td>14(32,6%)</td><td>13(31%)</td><td>15(39,5%)</td></tr></table>
Note: Quantitative data are presented in the form Me [LQ; UQ], where Me is the median, LQ is the value of the lower quartile; UQ is the value of the upper quartile, and categorical - in the form of absolute and relative frequencies of signs; for all presented indicators, differences between the studied groups were absent $(p > 0.05)$.
Most patients had one previously suffered myocardial infarction, MI. Patient groups were comparable in the number of MI $(p > 0.05)$, the presence of ischemic cardiomyopathy $(p > 0.05)$ and a history of cardiac arrhythmias (A), $p > 0.05$. Table 4 presents the frequency and structure of cardiac arrhythmias in patients with varying degrees of intraoperative hemolysis before coronary artery bypass surgery. As you can see, before surgery, cardiac arrhythmias were found in 22 people $(17.89\%)$. Among cardiac arrhythmias, AF paroxysms, supraventricular and ventricular extrasystoles, as well as blockade of the right and left legs of the bundle of His were found. At the same time, AF paroxysms were observed in 2 $(1.63\%)$ patients, extrasystoles were found in 11 $(8.94\%)$, including supraventricular extrasystoles, and in 3 $(2.44\%)$ - ventricular extrasystoles were noted. Dysfunction of the conduction function was noted in 8 people $(6.5\%)$, including blockade of the left leg of the bundle of His was noted in 5 people $(4.07\%)$, blockade of the right leg of the bundle of His - in 3 people $(2.44\%)$. The groups were comparable in the frequency and nature of cardiac arrhythmias in the anamnesis $(p > 0.05)$.
Patients before CB (1-5 days) and after surgery (within 1-5 days) underwent daily ECG monitoring, as well as standard electrocardiography (ECG). In order to clarify the role of hemolysis in the development of postoperative arrhythmias in the studied groups of patients with different levels of IOH, we analyzed the incidence of cardiac arrhythmias in the perioperative (during the operation and during the first day after it) and in the early period (up to 1 month) and their structure.
The examined patients received standard therapy consisting of antiplatelet agents (79.7%), statins (76.4%), beta-blockers (84.6%), angiotensin-converting enzyme inhibitors (76.4%), antianginal drugs (79.7%), table 5.
The drug treatment among patients of the studied groups did not differ in the administration of clopidogrel $(\chi^2 = 5.35; p = 0.069)$, $\beta$ -blockers $(\chi^2 = 3.18; p = 0.204)$, but it differed in the reception of statins $(\chi^2 = 12.2; p = 0.006)$, inhibitors of the angiotensin-converting enzyme, ACE inhibitors $(\chi^2 = 7.13; p = 0.028)$ and antianginal drugs $(\chi^2 = 13.7; p < 0.001)$. In particular, fewer patients in the third group took statins $(57.9\%, p < 0.05)$, inhibitors $(63.2\%, p < 0.001)$ and antianginal drugs $(60.5\%, p < 0.001)$. Patients with a history of cardiac arrhythmias (paroxysmal AF) were treated with antiarrhythmic drugs 5-7 days before surgery.
Table 5: Characterization of Drug Therapy for Examined Patients with Coronary Artery Disease before Coronary Artery Bypass Surgery with Varying Degrees of IOH
<table><tr><td>Index (%)</td><td>Gr 1
n=43</td><td>Gr 2
n=42</td><td>Gr 3
n=38</td><td>Gr 1-3
n=123</td><td>x2</td><td>p</td></tr><tr><td>betablockers</td><td>86,0</td><td>90,5</td><td>76,3</td><td>84,6</td><td>3,18</td><td>0,204</td></tr><tr><td>ACE inhibitors</td><td>88,4</td><td>76,2</td><td>63,2°</td><td>76,4</td><td>7,13</td><td>0,028</td></tr><tr><td>statins</td><td>90,7</td><td>78,6</td><td>57,9°•</td><td>76,4</td><td>12,2</td><td>0,006</td></tr><tr><td>antianginal</td><td>93,0</td><td>83,3</td><td>60,5°•</td><td>79,7</td><td>13,7</td><td>0,0001</td></tr><tr><td>antiplateletagents</td><td>88,4</td><td>81,0</td><td>68,4</td><td>79,7</td><td>5,35</td><td>0,069</td></tr></table>
To prevent arrhythmias during the operation, lidocaine was infused in a cardioplegic solution (1-1.5 mg/kg/min). After the operation, antiarrhythmic drugs were administered to arrest AF paroxysm (AF - 5 mg /kg intravenously dropwise for 60 min). Patients after CB took $\beta$ -blockers (atenolol 25-50 mg/day, metoprolol at a dose of 25-50 mg/day, bisoprolol at a dose of 2.5-5 mg/day) depending on the level of blood pressure. In patients with atrial flutter and ventricular tachycardia in the perioperative period, temporary atrial pacemaker was performed, which was maintained for 72 hours with a frequency of 10 beats/min more than their own heart rate.
Statistical data processing was carried out using the program Statistica 10.0 for Windows (StatSoft, Inc., USA). Given the abnormality of the distribution of attributes, nonparametric methods of descriptive statistics were used for processing: quantitative data are presented in the form Me [LQ; UQ], where Me is the median, LQ is the value of the lower quartile; UQ is the value of the upper quartile; categorical data are presented in the form of absolute and relative frequencies. When comparing the medians of quantitative variables of several independent groups, the Kruskell-Wallis test was used, to compare categorical data, the exact Fisher test, the $\chi^2$ criterion, with the Yeats correction at low frequencies were used. The strength of the relationship between the indicators was estimated using a correlation analysis based on the association coefficient (Kendall criterion) by its value (rs $\leq 0.25$ - weak; $0.25 < \mathrm{rs} < 0.75$ - moderate and $\geq 0.75$ - strong). In order to check the dependence of the incidence of arrhythmias on the degree of $\mathrm{logG}$, determined by the level of free hemoglobin, a logistic regression analysis and ROC analysis were performed in the statistical program SPSS Statistics 21.0 (SPSS, USA). Differences were considered significant at p $< 0.05$.
## IV. RESULTS
Of the 123 examined with CB, 29 (23.6%; $p < 0.001$ ) patients had cardiovascular complications. Moreover, complications in the perioperative period were noted in 17 people (13.8%, $p > 0.05$ ), in the early period - in 13 people (10.6%, $p > 0.05$ ). More often, in the operated patients, arrhythmias were revealed in 27 patients (21.95%, $p < 0.001$ ), less often - heart failure progression - in 12 patients (9.8%, $p < 0.001$ ), 5-person CB-associated myocardial infarction developed (4.1%; $p = 0.003$ ), and stroke in 2 patients (1.6%, $p = 0.323$ ).
The most common complications of CB during myocardial revascularization in patients with coronary artery disease were various types of arrhythmias, which were observed both in the perioperative period and during the month of observation - an early period (Table 6).
Table 6: The Frequency of Arrhythmias in Patients with Coronary Heart Disease after CB Surgery with Varying Degrees of Intraoperative Hemolysis (IOH)
<table><tr><td rowspan="2">Types of
Complications</td><td colspan="2">Group 1
n=43</td><td colspan="2">Group 2
n=42</td><td colspan="2">Group 3
n=38</td><td colspan="2">All
n=123</td><td rowspan="2">x2</td><td rowspan="2">p</td></tr><tr><td>n</td><td>%</td><td>n</td><td>%</td><td>n</td><td>%</td><td>n</td><td>%</td></tr><tr><td>Arrhythmias</td><td>2</td><td>4,7</td><td>5</td><td>11,9</td><td>20</td><td>52,6</td><td>27</td><td>22,0</td><td>21,95</td><td>0,000</td></tr></table>
After surgery, arrhythmias developed in 27 (21.95%) patients. At the same time, 5 (4.9%) patients had life-threatening arrhythmias (ventricular fibrillation, ventricular tachycardia), 7 (5.7%) patients had hemodynamically significant arrhythmias - atrial fibrillation and flutter, supraventricular tachycardia. Atrial fibrillation was the most common type of postoperative arrhythmias (5.7%, p<0.001), which is consistent with the literature. In 11 (8.9%) patients after CB, other types of arrhythmias (supraventricular extra systoles and ventricular extra systoles of I-II classes (according to the classification of Myerburg RJ, 1984), as well as AV blockade of the 1st or 2nd degree) were observed, accounting for about half of the occurring during and after surgery arrhythmias.
Most often, arrhythmias were observed in patients with a high degree of IOH (Table 7).
In the group with high IOH, the frequency of arrhythmias was $52.6\%$, which is higher than in the group with low IOH - $11.9\%$, $p < 0.001$ and in the group without IOH - $2.32\%$, $p < 0.001$ (table 8).
Table 7: Frequency and Structure of Arrhythmias in Patients with Coronary Artery Disease after CB with Different Degree in Intraoperative Hemolysis (IOH)
<table><tr><td>Types of Arrhythmias</td><td>n</td><td>Group 1
n=43
without IOH</td><td>n</td><td>Group 2
n=42</td><td>n</td><td>Group 3
n=38</td><td>x2</td><td>p</td></tr><tr><td>Total Arrhythmias</td><td>2</td><td>4,65</td><td>5</td><td>11,900···</td><td>20</td><td>52,600···</td><td>28,75</td><td>0,0000</td></tr><tr><td>Ventricular fibrillation</td><td>-</td><td>-</td><td>1</td><td>2,38</td><td>2</td><td>5,26</td><td>4,547</td><td>0,1020</td></tr><tr><td>Ventricular tachycardia</td><td>-</td><td>-</td><td>-</td><td>-</td><td>3</td><td>7,89</td><td>6,878</td><td>0,032</td></tr><tr><td>Atrial fibrillation</td><td>2</td><td>2,32</td><td>3</td><td>7,18</td><td>13</td><td>34,2000···</td><td>14,132</td><td>0,132660</td></tr><tr><td>Atrial flutter</td><td>-</td><td>-</td><td>1</td><td>2,38</td><td>1</td><td>2,63</td><td>1,100</td><td>0,5760</td></tr><tr><td>Supraventriculartachy cardia</td><td>-</td><td>-</td><td>-</td><td>-</td><td>1</td><td>2,63</td><td>2,255</td><td>0,3238</td></tr></table>
As can be seen from the table, in patients of the second (IIOH) and third (hIOH) groups, arrhythmias were more common than in the first group (without IOH), $p < 0.001$, and in patients of the 3rd group more often than in the second group, $p < 0.001$. Moreover, a significant part of arrhythmias (10.5%) in patients of the third group belonged to life-threatening arrhythmias and hemodynamically significant arrhythmias (13.2%). In 21.1% of patients with hIOH, other types of arrhythmias were noted ( $p < 0.05$ ).
On the 1st day after CB (perioperative period), arrhythmias were noted in 14 patients, $11.4\%$, $p < 0.00$. Most often $(26.31\%)$ of perioperative period arrhythmias were noted in the third group with hIOH, $p < 0.001$. Lifethreatening and hemodynamically significant arrhythmias in this period in the group with a high degree of IOH accounted for about half of all arrhythmias, which is significantly more than in the 1st and 2nd groups, $p < 0.001$.
In the early period, arrhythmias developed in $10.6\%$ of examined patients with CB. In the group with hIOH, arrhythmias were observed in 10 $(26.3\%)$ patients, in the group with IIOH – in 3 people $(7.14\%, p < 0.001)$, in the group without IOH - arrhythmias were not observed $(p < 0.001)$.
Correlation analysis using the non-parametric Kendall criterion (Rs) revealed the presence of associations between the indicator characterizing the degree of IOH - [Hb] in blood plasma and the frequency of arrhythmias in the postoperative period (Rs = 0.70, p <0.001), including in perioperative period (Rs = 0.46; p <0.001) and in the early period (Rs = 0.33; p <0.001) afterCB.
A correlation analysis revealed a moderate associative relationship between postoperative arrhythmias and a history of arrhythmias (Rs=0.4167, p=0.000003). There were also weak associations of the frequency of arrhythmias with the duration of the operation (Rs = 0.21, p = 0.018) and the time of clamping of the aorta (cardioplegia, Rs = 0.19, p = 0.026).
Based on logistic regression and ROC analysis, data were obtained that testify to the significance of the [Hb] indicator in assessing the likelihood of arrhythmias (Fig. 2).
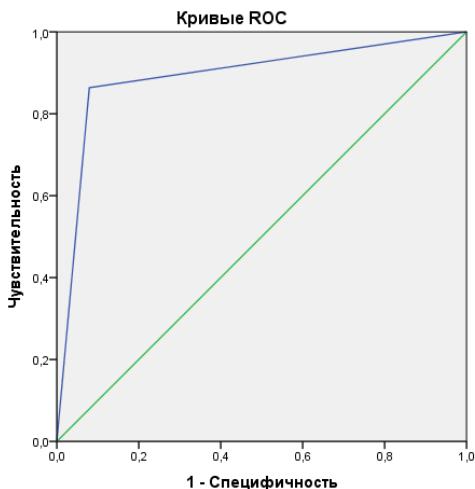
HanaohalbHeI cerMeHTbΦOpMpyOTc COBnadeHnRM. Fig. 2: ROC Curve Characterizing the Sensitivity and Specificity of the Method for Assessing the Likelihood of Developing Postoperative Arrhythmias by the Concentration of Free Hemoglobin in Blood Plasma
A high risk of developing arrhythmias in patients with coronary heart disease after CB was determined with a value of $[Hb] > 0.85$ g/l (sensitivity - $86.4\%$, specificity - $92.7\%$, PPV (predictive value of a positive result) = $96.9\%$, NPV (predictive value of a negative result) = $70.4\%$, area under the ROC-curve (AUC) = 0.892 (0.803-0.981), $95\%$ confidence interval.
Discussion. As noted earlier, before the operation, cardiac arrhythmias occurred in 22 people $(17.89\%)$. Among arrhythmias, AF paroxysms, supraventricular and ventricular extra systoles, as well as blockade of the right and left legs of the bundle of His were found. AF paroxysms were observed in 2 people (in 1 - in groups with IIOH and in 1 - in group with hIOH.
The groups were comparable in history and frequency of arrhythmias in history $(p > 0.05)$. However, the incidence of arrhythmias in postoperative the period was highest in the third group with hIOH, and in the second group with IIOH it was greater than in the group without IOH. According to the literature, the occurrence of arrhythmias associated with CB is caused by the restoration of blood flow in the ischemic zone, as a result of which the resumption of oxygenation initiates the development of oxidative stress. Action a reactive forms of oxygen and nitrogen leads to structural and metabolic disturbances, manifested by damage to cell membranes, electrolyte imbalance, forming a state of electrical myocardial heterogeneity, impaired excitability, pulse generation and conduction in the heart. Posttraumatic remodeling of heart chambers can contribute to the development of arrhythmias [6,7,9].
It was shown that not only the frequency of arrhythmias in groups after CB has changed, but also the structure. Transformation of less life-threatening arrhythmias (extrasystole, blockade of the bundle of His) into arrhythmias was noted, which had more serious consequences for hemodynamics and posed a greater threat to the lives of patients (atrioventricular block of the 1st degree, atrial fibrillation and flutter, paroxysmal ventricular and supraventricular ventricles).
Some authors have identified the relationship between arrhythmias and the features of surgical treatment (inadequate myocardial protection during surgery, due to the composition of the cardioplegic solution used, the direction of its administration, temperature, and the duration of cardioplegia). A positive correlation was revealed between the occurrence of arrhythmias and the duration of IR, the intensity of inotropic support, blood transfusion, and the level of leukocytosis after surgery. Other authors have not found such a dependence on the duration of artificial circulation.
CB has been shown to be most conducive to the development of arrhythmias in patients who had morphological changes in the heart (post-infarction cardiosclerosis) and a history of arrhythmias.
Studies on the study of arrhythmias after CB using correlation, as well as logistic and ROC analysis revealed the dependence of the frequency of arrhythmias on the level of free hemoglobin as an indicator of the degree of intraoperative hemolysis. The destruction of red blood cells due to their mechanical damage in the artificial circuits of the exerts a pathogenic effect on the state of the rhythmogenic function of the cardiac conduction system and myocardial excitability, predisposing to the development of arrhythmias. The largest number of arrhythmias in the group with a high level of free hemoglobin, as well as the presence of correlation between the frequency of arrhythmias and [Hb] In the blood plasma at the end of the operation, as well as the results of the logistic and ROC analysis, indicate the important role of intraoperative hemolysis in their occurrence in perioperative and early periods. The pathogenetic role of free hemoglobin in the development of rhythm disturbances in CB, it is advisable to develop a set of perioperative preventive measures aimed at chelation of free iron, which reduce the activity of oxidative processes. Elimination of patient-dependent risk factors for increased hemolysis (smoking, alcohol consumption, normalization of blood pressure, body weight and cholesterol) is also important for the prevention of cardiac arrhythmias, as one of the most common complications of coronary artery bypass surgery.
## V. CONCLUSIONS
1. Postoperative arrhythmias occur in approximately $22\%$ of patients undergoing CABG with cardiopulmonary bypass. A substantial portion of these arrhythmias are life-threatening or cause significant hemodynamic compromise and organ hypoperfusion.
2. Analysis demonstrated a strong correlation $(p < 0.001)$ between the incidence of postoperative arrhythmias and the degree of intraoperative hemolysis. Specifically, a higher plasma hemoglobin level of $0.5\mathrm{g / l}$ or greater was associated with a significantly increased risk of arrhythmias. A critical threshold for heightened arrhythmia risk was identified at free hemoglobin levels exceeding $0.85\mathrm{g / l}$.
3. These findings suggest that monitoring free plasma hemoglobin levels during CABG procedures may serve as a crucial indicator for predicting and preventing postoperative arrhythmias, and potentially guiding interventions to correct any hemodynamic complications.
Generating HTML Viewer...
References
7 Cites in Article
Luke Kim,Patrick Looser,Rajesh Swaminathan,Robert Minutello,S Wong,Leonard Girardi,Dmitriy Feldman (2007). Outcomes in patients undergoing coronary artery bypass graft surgery in the United States based on hospital volume, 2007 to 2011.
R Looser,R Swaminathan,Minutello (2016). Unknown Title.
E Maksimovich (2018). Aritmii u pacientov s IBS posle koronarnogo shunktirovaniya i raznoj spen`yu intraoperacionnogo gemoliza.
Shuab Omer,Lorraine Cornwell,Ankur Bakshi,Eric Rachlin,Ourania Preventza,Todd Rosengart,Joseph Coselli,Scott Lemaire,Nancy Petersen,Greg Pattakos,Faisal Bakaeen (2016). Incidence, Predictors, and Impact of Postoperative Atrial Fibrillation after Coronary Artery Bypass Grafting in Military Veterans.
Maksimovich Ye (2017). Early complications after coronary bypass operation/Maksimovich Ye.
E Fengsrud (2017). Pre-and postoperative atrial fibrillation in CABG patients have similar prognostic impact/E. Fengsrud, A. Englund.
C Valeri,H Macgregor,G Ragno,N Healey,J Fonger,S Khuri (2006). Effects of centrifugal and roller pumps on survival of autologous red cells in cardiopulmonary bypass surgery.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Maksimovich Yelizaveta N.. 2026. \u201cThe Role Of Hemolysis In The Development Of Arrhythmias In Patients With Ischemic Heart Disease After Coronary Artery Bypass Grafting Under Artificial Circulation\u201d. Unknown Journal GJMR-I Volume 25 (GJMR Volume 25 Issue I1): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
The Role Of Hemolysis In The Development Of Arrhythmias In Patients With Ischemic Heart Disease After Coronary Artery Bypass Grafting Under Artificial Circulation
Maksimovich Yelizaveta N.Grodno State Medical University