## I. INTRODUCTION
According to various studies, in professional athletes, ECG changes during chronic overstrain of the cardiovascular system, requiring an in-depth examination of a cardiologist, account for up to $40\%$, while in people who go in for sports only periodically - $12\%$ [1,2]. Modern standards in the interpretation of ECG in athletes. It should provide for the determination of changes in indicators both in relation to the healthy part of the general population and
Author $\alpha$: PhD, cardiologist of the Republican Scientific and Practical Center for Sports Medicine, Tashkent, Uzbekistan.
Author $\sigma$: MD, PhD, Professor, Scientific Advisor of the director of the Republican Scientific and Practical Center for Sports Medicine, Tashkent, Uzbekistan.
Author p: Researcher, Republican Scientific and Practical Center for Sports Medicine, Tashkent, Uzbekistan.
in relation to the ECG indicators in athletes, which are defined as the norm and reflect the physiological adaptation to physical activity [3].
During routine examinations, professional athletes often reveal electrocardiographic and hemodynamic disorders, which can be both a consequence of maladjustment processes and a consequence of organic cardiological pathology [4].
In this regard, it is of interest to comprehensively analyze heart rhythm disturbances in highly qualified athletes and to determine the patterns of their development along with their influence on the general physical characteristics of athletes.
Purpose of the study: To assess the indicators of adaptation of the cardiovascular system to increased physical activity in professional football players with heart rhythm disturbances.
## II. MATERIAL AND RESEARCH METHODS
The study was conducted on the basis of the Republican Scientific and Practical Center for Sports Medicine from 2019 to 2022. In total, 138 football players were surveyed, playing for 6 professional football clubs of the highest league of the Republic of Uzbekistan. The age of the athletes at the time of the study was 18 - 37 years old, and the sports experience was 5-15 years (the experience of sports activity took into account only performances for a professional club) years.
Exclusion criteria from the study:
- Acute and exacerbation of chronic diseases at the time of the study;
- Taking any medications.
The following methods were used to examine the footballer: collection and analysis of anamnestic data; electrocardiography (ECG); veloergometry (VEM); determination of physical work ability according to the $\mathrm{PWC}_{170} / \mathrm{Kr}$ test; determination of the value of the maximum oxygen consumption (MOC).
Physical performance was assessed using the $\mathrm{PWC}_{170}$ submaximal test and its modified version - the PWCAF test according to V.L. Karpman et al. (1988) [7], adapted for people of different ages. The calculation of the MPC was also carried out using the formulas proposed by Karpman for the value of $\mathrm{PWC}_{170}$.
Statistical processing of the results was carried out using the standard MS Office 2019 software package.
## III. RESULTS
When analyzing the ECG results of 138 professional football players, numerous changes were found that can be regarded as relatively safe and do not require specific treatment. The percentage of football players who had an absolutely normal ECG at rest, according to all generally accepted criteria, was relatively low - $24.6\%$ (34 athletes). Among this group of football players, no pathological changes in the ECG were noted in the process of stress testing.
The largest proportion of the surveyed football players had ECG changes, which are not considered the norm in the general population, but occur with a fairly high frequency in professional athletes. They are typical (frequent or "benign") signs for athletes that do not require additional examination and treatment in the absence of complaints and signs of organic heart damage [6]. These include sinus bradycardia (heart rate less than 55 beats/min), deceleration of conduction along the right bundle branch, severe sinus arrhythmia, pacemaker migration within the sinus node, and 1st degree AV block. The number of football players who had at least one of these conditions was 74 (53.6%) out of 138.
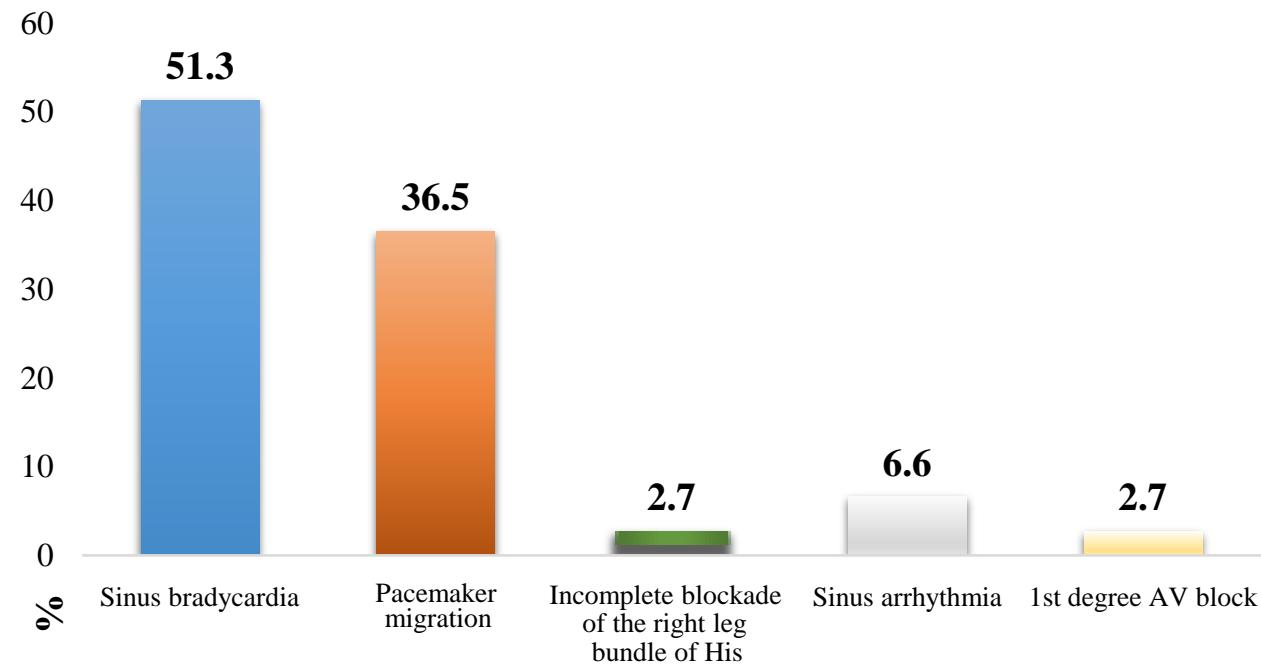 Figure 1: Distribution of "benign" rhythm disturbances.
The distribution of "benign" rhythm disturbances is shown in Figure 1. The graph shows that in the greatest number of cases, sinus bradycardia was determined - $51.3\%$. Pacemaker migration ranked second in frequency of occurrence and occurred in $36.5\%$ of football players. Other types of rhythm disturbances were much less common, sinus arrhythmia - in $6.6\%$, and incomplete right bundle branch block and 1st degree AV block - in $2.7\%$ of cases each.
The number of football players with identified "potentially dangerous" [6] heart rhythm disorders was 30 subjects (21.8%). The distribution of rhythm disturbances is shown in Figure 2.
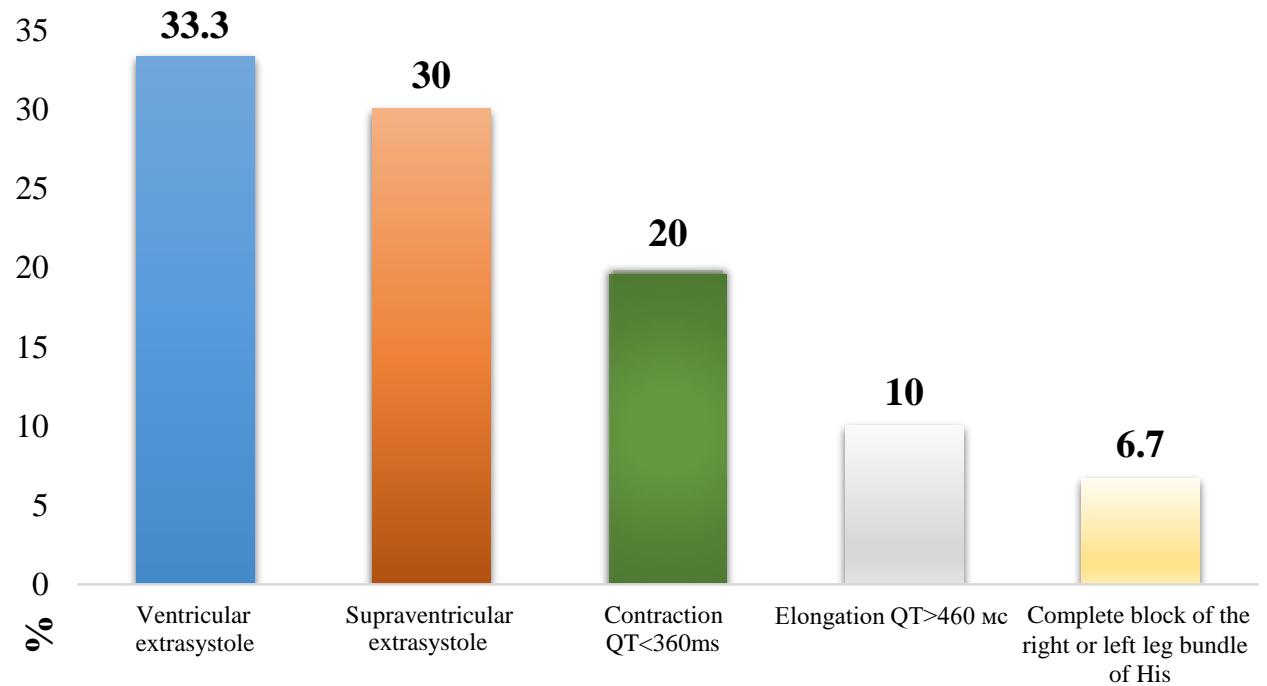 Figure 2: Distribution of "potentially dangerous" rhythm disturbances.
The graph shows that supraventricular and ventricular extrasystoles were most often detected in this group of athletes, in $30\%$ and $33.3\%$ of cases, respectively. All patients, in whom ES was detected at resting ECG, underwent further more in-depth examination during the day. As a result, it was revealed that $40\%$ of footballers have premature ventricular contraction (PVC) corresponding to grade 1 according to Lown, while $50\%$ of them have PVC corresponding to grade 2, and $10\%$ - to grade 3. In athletes with Supraventricular arrhythmia (SVA), single extrasystole (ES) prevailed $(44.4\%)$, paired ones were found in 2 athletes $(22.2\%)$, in all other cases, allorhythmia was determined by the type of tri- and quadrheminia.
The results of assessing the general physical performance and maximum oxygen consumption (MOC) in the football players we examined are presented in Table 1. The results showed that the $\mathrm{PWC}_{170}$ index in the group of "potentially dangerous" heart rhythm disturbances was significantly $(\mathsf{P} < 0.05)$ lower than in football players with "benign" heart rhythm disturbances and in the group with normal ECG. In turn, the indicators of athletes with "benign" rhythm disturbances were also significantly higher than those of athletes with a normal ECG. A similar trend was observed in the MOC. The lowest average MOC values - $48.3 \pm 1.64 \mathrm{ml} / \mathrm{min} / \mathrm{kg}$ were observed in football players with "potentially dangerous" rhythm disturbances.
Table 1: Physical performance and MOC in football players in the study groups
<table><tr><td></td><td>Group with "potentially dangerous" heart rhythm disorders n = 30</td><td>Group with "benign" rhythm disturbances n = 74</td><td>Group with normal ECG n = 34</td></tr><tr><td>PWC170(kgm/min/kg)</td><td>16.75 ± 0.45 * ^</td><td>19.9 ± 1.42 *</td><td>18.2 ± 1.38</td></tr><tr><td>MOC(ml/min/kg)</td><td>48.3 ± 1.64 * ^</td><td>57.64 ± 2.42 *</td><td>53.46 ± 1.82</td></tr></table>
## IV. DISCUSSION
Heart rate variability under conditions of adaptation of the body to tense muscular activity is a manifestation of the physiological mechanism of mobilization of the functional reserves of the heart. An increase in the functional reserve during adaptation of the body to continuous muscular activity occurs in 2 ways: by increasing the reserve level during urgent adaptation and as a result of long-term adaptation, which is characterized by a decrease in the initial level of functioning. Mobilization of functional reserves of urgent adaptation to physical activity is characterized by a period of functional stress [5,6, 7].
The process of mobilization of functional reserves with increased muscular activity has a direct dependence on the level of functioning of the body, and inverse dependence on the level of mobilization of functional reserves. The decrease in heart rate variability characterizes the degree of increased mobilization of the body's functional reserves. The independent development of cardiac arrhythmias without the presence of certain diseases may be associated with an abnormal location of the pathways in the heart, which can be manifested by the presence of additional pathways and the peculiarities of the sensitivity of pacemaker cells to adrenergic influences [8,9,10].
Thus, according to the concept proposed above, the results of the studies carried out can be explained by the fact that more significant heart rhythm disturbances in the group with "potentially dangerous" rhythm disturbances are a manifestation of maladjustment of the football player's body to physical activity, which is confirmed by reduced indicators of physical workability and aerobic performance (MOC). "Benign" ECG abnormalities, in turn, are a manifestation of an increase in the body's adaptation to increased physical activity in athletes with "benign" rhythm disturbances, which was confirmed by the highest indices of physical performance and aerobic performance (MOC).
## V. CONCLUSION
Thus, on the basis of functional tests of veloergometry (VEM), it was found that a group of football players with potentially dangerous rhythm disturbances showed a statistically significant decrease in physical performance and MOC. The presence of "benign heart rhythm disturbances" in football players is an indicator of a high level of physiological adaptation of the cardiovascular system of athletes to increased physical activity.
Generating HTML Viewer...
References
9 Cites in Article
L Balykova,S Ivyansky,E Gromova (2016). and other Pathogenetic aspects of the formation of maladaptive changes in the cardiovascular system, mediated by physical activity.
E Gavrilova (2015). Heart rate variability and sports.
N Garganeeva,I Taminova,V Kalyuzhin,E Kalyuzhina,I Smirnova (2012). Predictive factors of cardiovascular changes depending on the type and intensity of physical activity in professional athletes.
P Aagaard,S Sharma,D Mcnamara (2018). Risk of arrhythmia and conduction disease in former national football league players.
Kawtar Bennis,Fatima Labbi,Mohamed Bennani,Ilham Touhami,Ahmed Bennis (2010). 143 Echocardiographic assessment of cardiac remodeling in the high-level football player.
B Benito,G Gay-Jordi,A Serrano-Mollar (2011). Cardiac arrhythmogenic remodeling in a rat model of long-term intensive exercise training.
D Corrado,A Pelliccia,H Heidbuchel (2010). Recommendations for interpretation of 12-lead elec trocardiogram in the athlete.
Kimberly Harmon,Monica Zigman,Jonathan Drezner (2015). The effectiveness of screening history, physical exam, and ECG to detect potentially lethal cardiac disorders in athletes: A systematic review/meta-analysis.
Yasser Nassar,Maha Saber,Ayman Farhan,A Moussa,Ahmed Elsherif (2011). One year cardiac follow up of young world cup football team compared to nonathletes.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Surayyo Z. Yuldasheva. 2026. \u201cThe Role of Predictors in the Development of Arrhythmia and Cardiac Conduction Disorders in Highly Qualified Football Players\u201d. Global Journal of Medical Research - F: Diseases GJMR-F Volume 23 (GJMR Volume 23 Issue F4): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.